Page 6 of 15
EN1.2 | Pathophysiology of Common ENT Disorders — SDL Guide
Learning Objectives
- Describe the pathophysiology of tubotympanic and atticoantral chronic otitis media, including the mechanism of cholesteatoma formation and its complications
- Explain the pathophysiology of otosclerosis and its effect on hearing
- Describe the pathophysiology of acute and recurrent adenotonsillitis, its complications, and the consequences of adenoid hypertrophy
- Distinguish the pathophysiology of ethmoidal nasal polyposis from that of antrochoanal (Killian's) polyp, including their laterality and aetiology
- Correlate pathophysiological mechanisms with clinical examination findings and principles of management for each disorder
INSTRUCTIONS
This module builds directly on the anatomical map from EN1.1 and applies it to the pathophysiology of four clinically important ENT diseases specified in the NMC EN1.2 competency: Chronic Otitis Media, Otosclerosis, Adenotonsillitis, and Nasal Polyposis. For each disease, understanding the pathophysiology — not just the name — explains why the clinical presentation looks the way it does and why treatment must be what it is.
References
- Dhingra PL — Diseases of Ear, Nose & Throat, 7th ed., Chs 7–10 (COM/cholesteatoma), Ch 11 (Otosclerosis), Chs 30–31 (Tonsils/adenoid), Chs 21–22 (Nasal polyps) (textbook)
- Hazarika P — Textbook of Ear, Nose and Throat: Diseases, 4th ed., Sections on COM, Otosclerosis, Tonsillitis, Nasal Polyposis (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol. 3 Otology, Vol. 2 Rhinology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old man presents to your outpatient clinic with a 10-year history of right ear discharge and progressive hearing loss. He has had several courses of eardrops and antibiotics with temporary improvement, but the discharge always returns. Today, he also reports a new onset of right-sided facial weakness and dizziness. His wife noticed that his right eye is not closing properly. You examine the ear: there is a foul-smelling, creamy discharge filling the right EAC, and once it is cleaned, you see a whitish mass in the upper part of the drum with a small perforation at the margin. What is the mass? Why is his face drooping? And what did the referring doctor get wrong when they treated this for years as a simple ear infection?
WHY THIS MATTERS
Chronic ear disease is one of the commonest causes of preventable hearing loss in India, and the distinction between its two major types — tubotympanic ('safe') and atticoantral ('unsafe') — is arguably the single most important clinical differentiation in ENT. A doctor who cannot make this distinction risks treating a life-threatening disease with eardrops while cholesteatoma quietly erodes the facial nerve canal, the tegmen, and the wall of the sigmoid sinus. The NMC EN1.2 competency specifically requires you to describe the pathophysiology of Chronic Otitis Media, Otosclerosis, Adenotonsillitis, and Nasal Polyposis — four of the commonest ENT disorders you will encounter in your career. Understanding why a disease behaves the way it does is not just academic: it determines whether your management is a grommet insertion or an emergency mastoidectomy, a penicillin prescription or an incision-and-drainage, a nasal spray or an endoscopic sinus operation.
RECALL
Recall from EN1.1 that the tympanic membrane has two distinct regions: the pars tensa (the main drum, with a middle fibrous layer providing structural rigidity) and the pars flaccida (Shrapnell's membrane — the small upper portion between the malleal folds, lacking the fibrous layer and therefore structurally weaker). Recall that the Eustachian tube connects the middle ear to the nasopharynx and its primary function is to equalise air pressure between the middle ear and the atmosphere. Eustachian tube dysfunction — failure to open and ventilate the middle ear — creates negative pressure, which retracts the tympanic membrane. When negative pressure acts on the structurally weaker pars flaccida, a retraction pocket forms in the attic (epitympanum) — the first step in cholesteatoma formation. Recall also from PY that chronic inflammation leads to cytokine-mediated tissue remodelling, granulation tissue, and epithelial metaplasia — mechanisms you will now see at work in the diseased middle ear and nasal mucosa.
Why Pathophysiology of ENT Disorders Drives Clinical Thinking
The four ENT diseases specified in EN1.2 — Chronic Otitis Media, Otosclerosis, Adenotonsillitis, and Nasal Polyposis — share a common underlying theme: they are all diseases of chronic inflammation and structural remodelling affecting specific anatomical sites in the ENT region, and in each case the pathophysiological mechanism determines the clinical presentation, the complications, and the appropriate treatment. Understanding this theme prevents the most dangerous errors in ENT clinical practice.
Consider Chronic Otitis Media (COM): it is not simply 'a hole in the eardrum.' Two different pathological processes can both produce a perforated eardrum and ear discharge, but one is a mucosal disease that rarely causes serious complications and can often be treated medically, while the other is driven by an expanding keratinising squamous epithelial cyst — a cholesteatoma — that erodes bone and can kill the patient through intracranial extension. The clinical presentations overlap enough that a cursory examination misses the distinction. Only a clinician who understands the pathophysiology can be trusted to distinguish them.
Similarly, understanding that otosclerosis causes conductive hearing loss through a specific mechanism — bony fixation of the stapes footplate — rather than through ear infection or a membrane perforation, explains why it cannot be treated with antibiotics and why its surgical treatment (stapedectomy) specifically addresses the fixed footplate. Understanding that ethmoidal nasal polyps are driven by eosinophilic inflammation in adults and tend to be bilateral, while an antrochoanal polyp arises unilaterally from the maxillary antrum in a younger patient, determines whether you recommend topical steroids or endoscopic surgery to the maxillary antrum.
This module is structured around the mechanism of each disease — because mechanism is the bridge between anatomy and clinical decision-making.
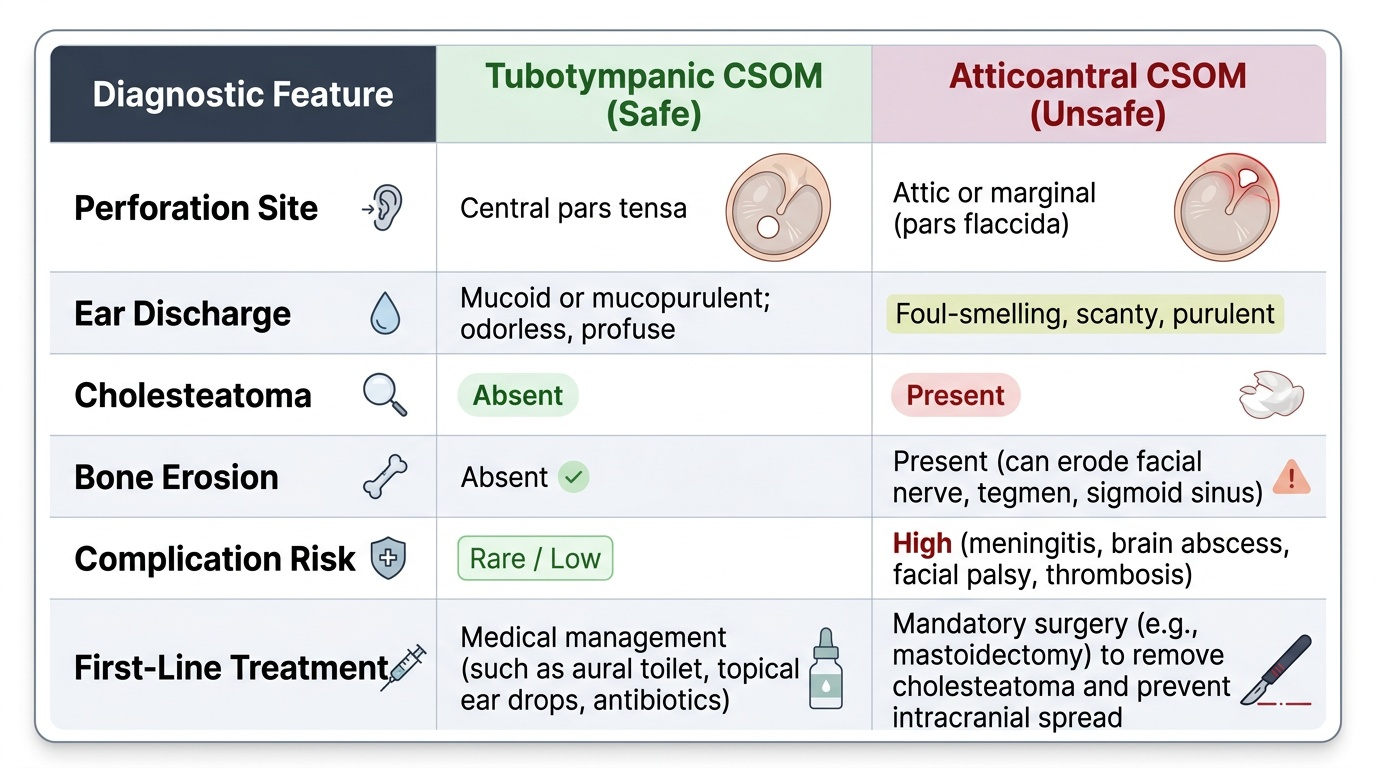
Chronic Otitis Media: Tubotympanic (Safe) Type
Chronic Otitis Media (COM) is defined as a chronic inflammatory condition of the middle ear cleft (middle ear cavity, Eustachian tube, and mastoid air cells) with a non-intact tympanic membrane for at least three months. The two types of COM differ in their pathological mechanism, anatomical site, complications, and treatment, and correctly distinguishing them is mandatory in clinical practice.
Pathogenesis of Tubotympanic CSOM
The tubotympanic (mucosal) type begins with Eustachian tube dysfunction — typically from recurrent acute otitis media in childhood, repeated upper respiratory tract infections, or adenoid hypertrophy blocking the Eustachian tube orifice. Repeated episodes of AOM cause the pars tensa to become inflamed and eventually to perforate. Once a central perforation of the pars tensa is established, the middle ear mucosa is exposed to the external environment, becomes chronically inflamed (mucosal metaplasia, goblet cell hyperplasia), and produces the characteristic mucoid or mucopurulent discharge that drains through the perforation into the EAC. Critically, the disease remains confined to the mucosa — it does NOT produce squamous epithelium, does NOT form cholesteatoma, and does NOT erode bone (hence 'safe'). The perforated drum reduces the area available for sound pressure transmission to the ossicular chain, and the disrupted middle ear air-pressure system reduces ossicular mobility, producing a conductive hearing loss typically in the 20–40 dB HL range.
Key features (must be memorised for both clinical examination and examinations):
- Perforation site: central, in the pars tensa — the margin of the perforation has a remnant of pars tensa all the way to the handle of the malleus. There is an annular (rim) of normal TM surrounding it.
- Discharge: mucoid or mucopurulent, non-foul-smelling (serous/mucinous glands of the middle ear mucosa).
- Cholesteatoma: absent.
- Complications: uncommon; when they occur, they are usually mild (conductive hearing loss, secondary infections). Dangerous intracranial complications are rare.
- Treatment approach: initial medical management (aural toilet, topical antibiotics — ciprofloxacin drops are preferred over aminoglycosides, which are ototoxic, for ears with perforations); surgical repair of the perforation (myringoplasty) once the ear is dry for at least 3 months.
Chronic Otitis Media: Atticoantral (Unsafe) Type and Cholesteatoma
The atticoantral type is fundamentally different from the tubotympanic type in its mechanism, its destructive potential, and its mandatory surgical management. This is the 'unsafe' type — a name that undersells its danger: untreated atticoantral CSOM with cholesteatoma can erode the facial nerve canal causing facial palsy, erode the tegmen causing meningitis and brain abscess, and erode the sigmoid sinus wall causing sigmoid sinus thrombosis. Every clinician must be able to identify it.
Provided image
Pathogenesis of Atticoantral CSOM and Cholesteatoma
The atticoantral type begins in the pars flaccida (Shrapnell's membrane — recall from EN1.1 that this upper portion of the TM lacks the fibrous layer, making it susceptible to retraction under negative pressure). Eustachian tube dysfunction creates chronic negative middle ear pressure, which draws the pars flaccida inward, creating a retraction pocket in the attic (epitympanum — the space above the level of the tympanic annulus). This retraction pocket is lined by squamous epithelium (from the outer skin layer of the TM). Squamous epithelium is a self-renewing sheet that normally migrates outward (the self-cleaning mechanism of the EAC). When trapped in a retraction pocket, this epithelium cannot migrate normally — it desquamates, and the accumulated keratin debris forms a cholesteatoma (literally: 'cholesterol tumour' — a misnomer, as it contains keratin, not cholesterol; the name persists historically). The cholesteatoma sac continues to expand as new squamous epithelium is added and keratin accumulates. Critically, the expanding cholesteatoma sac releases collagenolytic enzymes (matrix metalloproteinases) and cytokines (TNF-α, IL-1) that actively erode the surrounding bone — the hallmark destructive property that makes cholesteatoma dangerous.
Sites and sequence of bone erosion by cholesteatoma:
Cholesteatoma typically begins in the attic and then expands in predictable directions, eroding bone as it progresses:
1. Ossicles (most commonly first): the long process of the incus is the most frequently eroded ossicular element, followed by the stapes superstructure — producing conductive hearing loss.
2. Tegmen tympani (roof of the middle ear, separating it from the middle cranial fossa dura): erosion → intradural spread → epidural abscess, meningitis, temporal lobe abscess.
3. Lateral wall of the sigmoid sinus: erosion → sigmoid sinus thrombophlebitis (Bezold's abscess possible via inferior extension).
4. Facial nerve canal (tympanic or mastoid segment): erosion → facial palsy — the presentation in our opening case.
5. Lateral semicircular canal (horizontal SCC): erosion → labyrinthitis (sensorineural hearing loss + vertigo).
6. Cochlea: severe SNHL.
Key features:
- Perforation site: attic (pars flaccida) or marginal (posterior-superior pars tensa, near the posterior annulus) — the margin of the perforation touches the bony wall of the EAC without a rim of normal TM. This is the critical otoscopic finding.
- Discharge: scanty, foul-smelling (keratin debris infected by anaerobic bacteria — Pseudomonas, Bacteroides, Proteus).
- Cholesteatoma: a white, pearly mass visible in the attic or posterior-superior quadrant; glistening keratin debris.
- Bone erosion: scutum (attic wall), ossicles — identifiable on CT of temporal bone.
- Treatment: ALWAYS surgical — mastoidectomy (canal wall up or canal wall down, depending on disease extent and patient factors). Medical treatment alone is never appropriate for atticoantral CSOM with cholesteatoma.
SELF-CHECK
A 28-year-old woman has had left ear discharge for 7 years. Otoscopy shows a large central perforation of the left pars tensa with mucopurulent discharge and an otherwise healthy middle ear mucosa. Audiometry shows 30 dB conductive hearing loss. No cholesteatoma is visible. Which statement is MOST accurate?
A. This is atticoantral (unsafe) CSOM — arrange urgent mastoidectomy
B. This is tubotympanic (safe) CSOM — treat medically, consider myringoplasty when the ear is dry
C. This is CSOM unsafe type because the hearing loss is 30 dB — refer immediately for surgery
D. The absence of foul smell rules out any form of CSOM — reassure and discharge
Reveal Answer
Answer: B. This is tubotympanic (safe) CSOM — treat medically, consider myringoplasty when the ear is dry
Central perforation of the pars tensa + mucoid/mucopurulent (not foul-smelling) discharge + no cholesteatoma visible = tubotympanic (mucosal/'safe') type CSOM. Conductive hearing loss of 20–40 dB is expected from the perforation — it is not, by itself, a criterion for unsafe type. The 'unsafe' distinction requires an attic/marginal perforation AND/OR visible cholesteatoma (white pearly mass, foul-smelling discharge, bone erosion). Option A is wrong — central perforation without cholesteatoma is not atticoantral disease. The patient should receive aural toilet and topical antibiotics initially, and be considered for myringoplasty when dry for 3 months.