Page 8 of 15
EN1.2 | Pathophysiology of Common ENT Disorders — SDL Guide (Part 3)
Nasal Polyposis: Ethmoidal and Antrochoanal Types
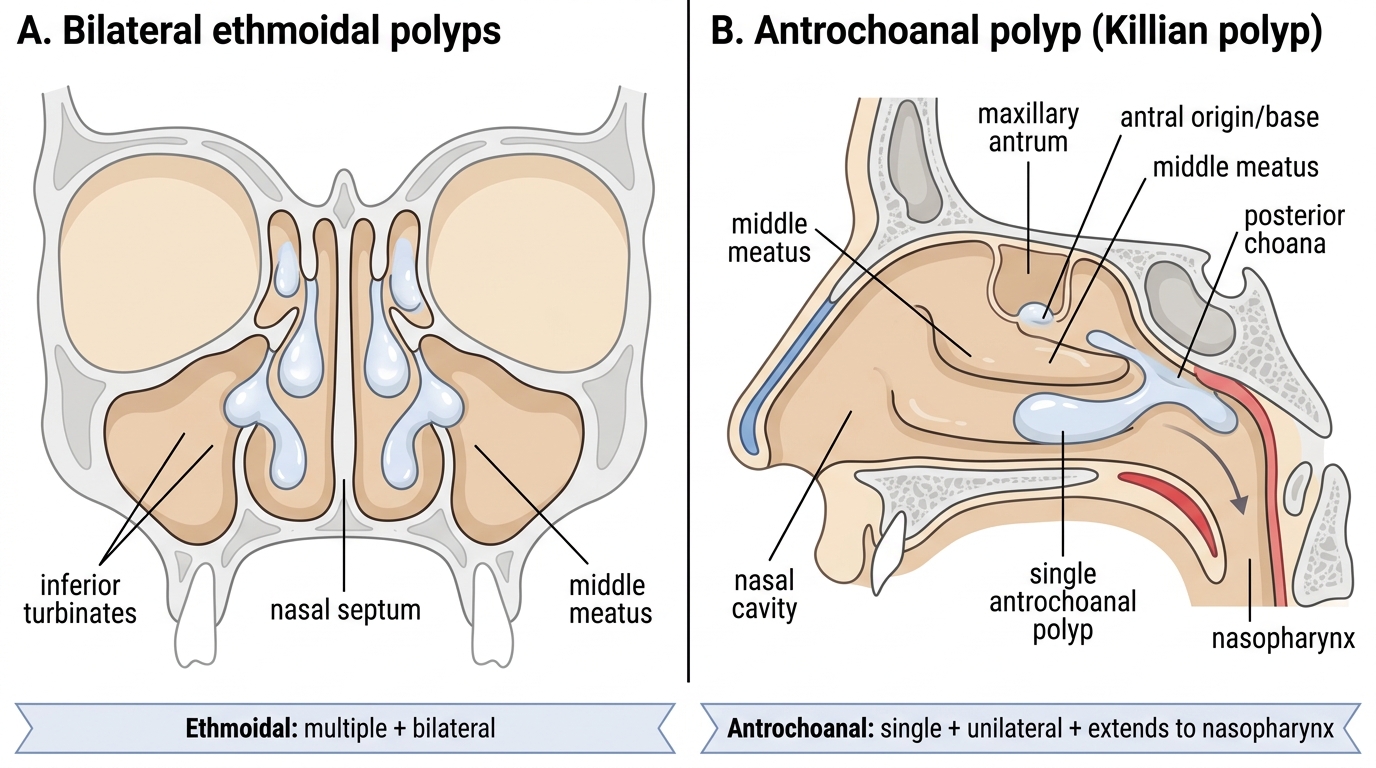
Nasal polyps are smooth, pale, pedunculated masses of oedematous nasal mucosa arising from the sinuses or nasal cavity. The critical clinical distinction in nasal polyposis is not merely academic — it determines whether you are dealing with a bilateral, recurrent, allergy-driven disease of the sinuses (requiring long-term management) or a single unilateral benign growth that can be definitively cured by surgery. The distinction is memorised by two contrasting pairs: bilateral/multiple vs unilateral/single, and adults/allergy vs young patients/antrum.
Ethmoidal (Bilateral) Nasal Polyps
Ethmoidal polyps arise from the mucosa of the ethmoidal sinuses, primarily in the region of the middle meatus and the ostiomeatal complex. They are driven by chronic eosinophilic inflammation — an allergic or non-allergic eosinophilic mechanism that produces oedema of the sinus mucosa, exudation of eosinophilic fluid into the submucosa, and gradual prolapse of the oedematous mucosa into the nasal cavity as a polyp. Grossly, ethmoidal polyps are pale, glistening, semi-translucent, multiple, and bilateral (because the eosinophilic process affects both ethmoidal complexes). They are typically insensate (no pain on probing — differentiating them from turbinate tissue, which is sensitive) and mobile.
Important associations of ethmoidal polyposis:
- Allergic rhinitis: most common co-morbidity; perennial allergy drives the eosinophilic process.
- Asthma: approximately 30% of patients with nasal polyps have asthma; the 'unified airway' concept — the same eosinophilic/allergic inflammation affecting both upper and lower airways.
- Samter's triad (Aspirin-Exacerbated Respiratory Disease, AERD): the triad of aspirin/NSAID sensitivity + asthma + nasal polyposis. The mechanism is arachidonic acid pathway dysregulation: COX-1 inhibition by aspirin blocks prostaglandin E2 (which normally suppresses eosinophilia), shunting the pathway toward leukotriene overproduction — producing bronchospasm and nasal symptoms within hours of aspirin ingestion. Samter's triad patients have the most severe and recurrent polyposis.
- Treatment: topical intranasal corticosteroids (mometasone, fluticasone) are first-line — they suppress eosinophilic inflammation and can significantly reduce polyp size; systemic corticosteroids for acute exacerbations; functional endoscopic sinus surgery (FESS) for polyps that do not respond to medical therapy or that are obstructing the sinus ostia/causing anosmia. Ethmoidal polyps recur after surgery — patients require long-term medical management post-FESS.
Antrochoanal Polyp (Killian's Polyp)
The antrochoanal polyp is entirely different in pathogenesis, laterality, and behaviour. It arises as a single, unilateral cyst-like lesion from the mucosa of the maxillary antrum (maxillary sinus), expands through the sinus ostium (usually through an accessory ostium or through the enlarged natural ostium), passes through the middle meatus, and extends posteriorly through the posterior choana into the nasopharynx. On posterior rhinoscopy or nasendoscopy, it appears as a smooth, firm, pale mass at the choanal opening or hanging in the nasopharynx.
Distinguishing features of the antrochoanal polyp:
- Unilateral and single — this is the defining feature; bilateral or multiple polyps are not antrochoanal.
- Commoner in children and young adults — versus ethmoidal polyps which are predominantly in adults.
- Not strongly associated with allergy — aetiology is debated; chronic maxillary sinusitis and cystic degeneration of the antral mucosa are proposed mechanisms.
- Extends to the nasopharynx — a large antrochoanal polyp fills the posterior nasal cavity and may cause significant unilateral nasal obstruction + mouth breathing; on posterior rhinoscopy it may be the most prominent finding.
- Does NOT recur after complete removal — if the antral base (the stalk within the maxillary sinus) is completely removed endoscopically, surgical cure is achieved. This contrasts sharply with ethmoidal polyps, which recur even after thorough FESS.
- Treatment: endoscopic polypectomy removing the entire polyp including the antral base (via the middle meatus, with a wide middle meatal antrostomy to access the sinus and remove the stalk).
Ethmoidal Polyps vs Antrochoanal Polyp
SELF-CHECK
A 10-year-old boy presents with unilateral right nasal obstruction and mouth breathing for 4 months. On examination, a smooth, pale, insensate mass is seen in the right posterior nasal cavity and extends into the nasopharynx on flexible nasendoscopy. The left nasal cavity is clear. Which diagnosis and management is MOST appropriate?
A. Bilateral ethmoidal nasal polyposis — prescribe intranasal corticosteroids and review in 8 weeks
B. Antrochoanal polyp (Killian's polyp) — refer for endoscopic polypectomy including removal of the antral base
C. Antrochoanal polyp — prescribe topical steroids as first-line treatment (surgical approach has high recurrence)
D. Juvenile nasopharyngeal angiofibroma — take a biopsy immediately to confirm the diagnosis
Reveal Answer
Answer: B. Antrochoanal polyp (Killian's polyp) — refer for endoscopic polypectomy including removal of the antral base
A unilateral, single, smooth pale mass in the nasal cavity of a child/young adolescent that extends into the nasopharynx is an antrochoanal polyp (Killian's polyp) until proven otherwise. It is unilateral and single (ruling out ethmoidal polyps, which are bilateral and multiple). The definitive treatment is endoscopic polypectomy including removal of the maxillary antral base — when complete, it does not recur. Option A is wrong (ethmoidal polyps are bilateral). Option C is wrong — topical steroids are NOT the primary treatment for antrochoanal polyp (unlike ethmoidal polyps). Option D is extremely dangerous: in an adolescent male, a vascular mass in the nasopharynx could be a Juvenile Nasopharyngeal Angiofibroma (JNA) — DO NOT BIOPSY (catastrophic haemorrhage). However, JNA is characteristically in adolescent males with recurrent epistaxis, and a smooth, pale, insensate mass in a child more consistent with polyp features. In practice, nasopharyngeal masses should be assessed with CT/MRI before biopsy.
CLINICAL PEARL
The clinical pearl for this module has two parts, one for each ear-disease and one for the nose. For COM: the single most dangerous error in ENT is treating atticoantral CSOM as if it were tubotympanic. The otoscopic distinction is: if the perforation touches the bony wall of the EAC (marginal), or is in the attic (pars flaccida), or you see any white pearly material or foul-smelling discharge — that ear needs a CT scan and surgical referral, not eardrops. The motto: 'Foul smell and attic hole — always refer, never just control.' For nasal polyps: whenever you encounter a unilateral nasal mass in an adolescent male, DO NOT BIOPSY before imaging. Juvenile nasopharyngeal angiofibroma (JNA) is exquisitely vascular, and an ill-considered biopsy can cause catastrophic, life-threatening haemorrhage. The diagnosis is made on contrast-enhanced CT or MRI (showing the characteristic skull base erosion and intense enhancement), not on tissue biopsy at clinic.
Comparing the Four Diseases: Examination and Investigation
Each of the four EN1.2 diseases has a characteristic examination profile and investigation pattern that follows directly from its pathophysiology. A student who understands the mechanism can predict what the examination and investigations will show, rather than memorising arbitrary lists.
The clinician who understands pathophysiology will not be surprised by what they find: if stapes fixation prevents normal transmission of sound energy, the audiogram must show a conductive hearing loss without a membrane perforation; if a cholesteatoma is eroding the long process of the incus, the audiogram will show worse hearing loss than the perforation alone would explain; if the middle ear is filled with viscous glue, the tympanogram compliance curve must be flat. This 'predictive' approach — deriving expected findings from the mechanism — is both more reliable at the bedside and more memorable in examinations than trying to memorise disconnected findings for each disease.
Otoscopy findings:
- Tubotympanic CSOM: central perforation of the pars tensa (rim of TM around the perforation); middle ear mucosa visible through the hole (may appear pink and inflamed); mucoid/mucopurulent discharge in the EAC; ossicles may be visible if the perforation is large.
- Atticoantral CSOM: attic perforation (pars flaccida retraction pocket with keratin debris) or marginal perforation (touching the bony annulus at the posterior-superior quadrant); white pearly mass (cholesteatoma) or granulation tissue; foul-smelling discharge.
- Otosclerosis: normal-appearing tympanic membrane — no perforation, no retraction, no discharge. The classic sign (present in only approximately 10% of cases but highly specific when present) is a flamingo-pink blush seen through the anterior TM, reflecting the increased vascularity of the active otospongiotic focus (Schwartze sign). This absence of any visible TM abnormality in a patient with progressive conductive hearing loss is a major diagnostic clue.
- OME (from adenoid hypertrophy): amber or yellowish TM (as the fluid level or bubbles show through the translucent drum); retracted TM (concave, with the handle of malleus appearing more horizontal); absent cone of light; sluggish or absent TM movement on Siegel's speculum pneumatic otoscopy.
Audiometry:
- CSOM tubotympanic: conductive hearing loss (air-bone gap, bone conduction normal) — size proportional to the perforation size and ossicular discontinuity.
- CSOM atticoantral with ossicular erosion: conductive or mixed hearing loss; if labyrinth is invaded, SNHL component.
- Otosclerosis: conductive hearing loss with normal TM on otoscopy; Carhart notch (dip in bone conduction at 2000 Hz — a mechanical artefact of stapes fixation).
- OME: mild to moderate conductive hearing loss (15–35 dB HL).
Tympanometry:
- Normal: Type A (normal compliance peak near 0 daPa).
- OME or perforation: Type B (flat, no compliance peak — middle ear filled with fluid or the ear is open).
- Otosclerosis: Type As (reduced compliance/'shallow' peak — stapes fixation reduces TM/ossicular system compliance).
- Eustachian tube dysfunction: Type C (peak shifted to negative pressure, -100 to -300 daPa).
CT scan of the temporal bone:
Indicated when atticoantral CSOM is suspected. High-resolution CT (HRCT) temporal bone demonstrates bone erosion (scutum, ossicles, tegmen, sigmoid sinus plate, facial nerve canal, semicircular canals). This is the preoperative planning scan for mastoidectomy — it maps the extent of disease and identifies which landmarks are at risk during surgery.
Nasal endoscopy:
Ethmoidal polyps: smooth, pale, glistening masses in the middle meatus, bilateral. Antrochoanal polyp: single unilateral polyp tracked from the middle meatus to the choana. A mass in the nasopharynx in an adolescent male: CT or MRI before ANY biopsy (JNA must be excluded).
Diagnosis and Differential Diagnosis
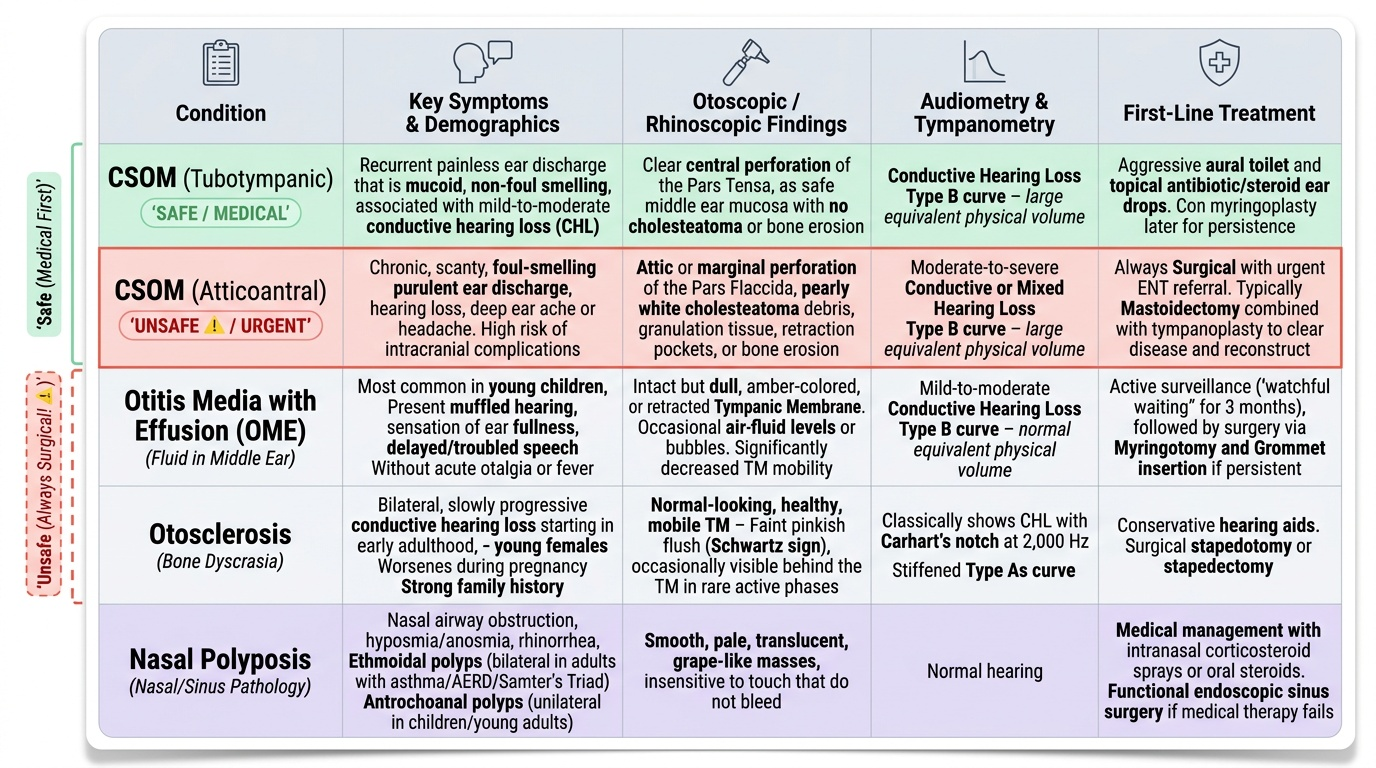
The four disorders in EN1.2 each present with overlapping symptoms — hearing loss, nasal obstruction, and throat symptoms — but can be distinguished by combining the history (age, duration, laterality), otoscopic/rhinoscopic findings, and audiometry/tympanometry. The following table encodes the key differentiating features. Memorising this framework enables rapid differential diagnosis at the bedside and in examination settings.
Arriving at the correct diagnosis requires the clinician to integrate four information streams simultaneously: the patient's age and demographic profile (otosclerosis in a young Caucasian woman; antrochoanal polyp in a child; ethmoidal polyps in an adult with asthma), the anatomical site of the pathology (central vs attic/marginal perforation; unilateral vs bilateral nasal mass), the quality of any discharge or secretion (mucoid vs foul-smelling; bilateral vs unilateral), and the audiometric and tympanometric profile. A systematic approach that addresses all four streams prevents the most common clinical errors — the most dangerous of which is misclassifying atticoantral CSOM as tubotympanic and treating with eardrops.
Provided image
For chronic ear disease, the crucial differential is between tubotympanic and atticoantral CSOM — two conditions that both produce a perforated eardrum and ear discharge but differ fundamentally in safety and management:
- Tubotympanic: central perforation + mucoid/non-foul discharge + no cholesteatoma = safe = medical management first
- Atticoantral: attic/marginal perforation + foul discharge + cholesteatoma/granulations + bone erosion = unsafe = always surgical
For conductive hearing loss with a normal-looking TM, the differential includes otosclerosis vs ossicular fixation from a different cause vs tympanosclerosis:
- Otosclerosis: normal TM, bilateral progressive CHL in 2nd–4th decade, Type As tympanogram, Carhart notch
- Tympanosclerosis: white calcified plaques visible on the TM; thickened TM
- Congenital ossicular fixation: present from birth, no EAR history
For nasal polyposis, the most important differential is:
- Bilateral/multiple polyps in an adult with allergy/asthma history = ethmoidal polyps (chronic eosinophilic sinusitis)
- Unilateral/single mass in young patient from maxillary antrum = antrochoanal polyp
- Unilateral mass in nasopharynx in adolescent male with epistaxis = JNA (DO NOT BIOPSY — imaging first)
- Unilateral nasal mass in adult >40 years = inverted papilloma (locally invasive; associated with HPV; requires en bloc surgical excision; 5–10% malignant transformation risk)
| Feature | Tubotympanic CSOM | Atticoantral CSOM | OME (glue ear) | Otosclerosis |
|---|---|---|---|---|
| Perforation | Central, pars tensa | Attic or marginal | None (TM intact) | None (TM intact) |
| Discharge | Mucoid/mucopurulent | Foul-smelling, scanty | None | None |
| Cholesteatoma | Absent | Present | Absent | Absent |
| TM appearance | Perforation visible | Retraction pocket/keratin | Amber/retracted TM | Normal |
| Hearing loss type | Conductive | Conductive/mixed | Conductive | Conductive |
| Tympanogram | Type B (perforation) | Type B | Type B | Type As |
| Audiogram feature | Air-bone gap | Air-bone gap ± SNHL | Air-bone gap (mild) | Carhart notch 2000 Hz |
| Complication risk | Low | High (CN VII palsy, meningitis) | Low | Low |
| Treatment | Medical + myringoplasty | Always surgery | Watchful wait/grommets/adenoidectomy | Hearing aid or stapedectomy |
SELF-CHECK
A 32-year-old woman presents with bilateral progressive hearing loss since her first pregnancy 4 years ago. Both ears look entirely normal on otoscopy — no perforation, no discharge, no retraction. Pure-tone audiometry shows bilateral conductive hearing loss with a notch at 2000 Hz on bone conduction testing. Tympanometry shows Type As bilaterally. The most likely diagnosis is:
A. Bilateral OME (glue ear) — refer for grommets
B. Bilateral CSOM tubotympanic — begin topical antibiotics
C. Otosclerosis — refer for audiological/surgical assessment
D. Bilateral vestibular neuritis — MRI of internal auditory canal
Reveal Answer
Answer: C. Otosclerosis — refer for audiological/surgical assessment
The triad of bilateral progressive CONDUCTIVE hearing loss + normal-looking tympanic membranes + Carhart notch at 2000 Hz + Type As tympanogram is pathognomonic of OTOSCLEROSIS. Pregnancy is a recognised aggravating factor (oestrogen stimulates the otospongiotic process). Type As tympanogram (reduced compliance) reflects stapes fixation. OME would show Type B tympanogram and an abnormal TM (amber-coloured, retracted). CSOM would show a perforation. Vestibular neuritis causes sensorineural (not conductive) hearing loss and is typically unilateral and associated with acute vertigo. Otosclerosis management: hearing aid as first option; surgical stapedectomy/stapedotomy for candidates who prefer surgery over hearing aids.