Page 12 of 20
EN4.46 | HIV Manifestations in ENT — SDL Guide
Learning Objectives
- Describe the spectrum of HIV-related manifestations in the ear, nose, throat, and neck
- Recognise the characteristic clinical features of oral candidiasis, oral hairy leukoplakia, Kaposi's sarcoma, and HIV-associated lymphoepithelial cysts
- Identify appropriate investigations for ENT manifestations in HIV including CD4 count, culture, biopsy, and audiometry
- Distinguish between ENT lesions seen in HIV and their non-HIV mimics
- Outline the principles of management of common ENT manifestations in HIV, including the role of antiretroviral therapy
INSTRUCTIONS
HIV infection has profound effects on every region of the head and neck, because the mucosal surfaces of the upper aerodigestive tract and the lymphatic system of the neck are among the first and most consistently affected sites as CD4+ T-cell counts decline. ENT manifestations may be the presenting feature that leads to an HIV diagnosis, or they may be recurring problems in a known HIV-positive patient on or off antiretroviral therapy. At the MBBS level, competency EN4.46 requires knowledge of the clinical features, investigations, and management principles of these manifestations — and the ability to recognise patterns that should prompt HIV testing in a patient not previously diagnosed.
References
- Dhingra PL, Dhingra S — Diseases of Ear, Nose & Throat, 8th ed., Chapter: HIV and ENT (textbook)
- Hazarika P — Textbook of Ear, Nose & Throat, 4th ed., Chapter on HIV Manifestations in ENT (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed., Vol 2, Chapter: HIV and the Head and Neck (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 32-year-old man presents to the ENT outpatient department with two months of progressive difficulty swallowing and a white coating on his tongue. He has also noticed several painless purple-brown spots on the hard palate over the past month, and his collar size has increased — he attributes this to weight gain, but on examination he has bilateral firm, non-tender cervical and parotid swellings. He denies fever, night sweats, or weight loss. His oral temperature is normal. You look in his mouth: white removable plaques cover the tongue and buccal mucosa, and two violaceous lesions are visible on the hard palate. You gently wipe one plaque — it comes off, leaving a raw bleeding surface. Now look at the bilateral parotid swellings and neck nodes, the oral thrush, and the violaceous palatal lesions together. You are looking at a constellation of findings that should immediately make you consider HIV as the unifying diagnosis.
WHY THIS MATTERS
India has a significant HIV burden, and the head and neck is one of the most commonly affected regions of the body in HIV disease — estimates suggest that 30–80% of HIV-positive individuals develop at least one oral manifestation during the course of their illness, with the prevalence and severity correlating inversely with CD4 count. This means that ENT manifestations are not just a footnote in HIV care — they are often the presenting features that first bring a patient to medical attention. An ENT surgeon or MBBS doctor who recognises the clinical patterns of oral candidiasis, oral hairy leukoplakia, Kaposi's sarcoma, and HIV-associated neck lymphadenopathy is in a position to initiate HIV testing and potentially change the course of a patient's disease by enabling early antiretroviral therapy. Beyond diagnosis, recurring or treatment-refractory ENT conditions (sinusitis that does not respond to standard antibiotics, oral ulcers that keep returning, hearing loss in a young person) should always raise the question: could this patient be immunocompromised, and should HIV be excluded?
RECALL
Recall the basics of HIV immunopathology from your Physiology and Microbiology modules. HIV (Human Immunodeficiency Virus) is an RNA retrovirus that targets CD4+ T lymphocytes by binding the CD4 receptor. Over years of untreated infection, the CD4 count falls from the normal range (500–1500 cells/μL) through an immunologically asymptomatic phase, then through the symptomatic phase as counts fall below 350–500, and into AIDS (Acquired Immunodeficiency Syndrome) when the CD4 count drops below 200 cells/μL or an AIDS-defining illness occurs. The mucous membranes of the oropharynx are part of the mucosal immune system (MALT — mucosa-associated lymphoid tissue) and are particularly vulnerable to immune failure. Waldeyer's ring (palatine tonsils, adenoids, lingual tonsil, tubal tonsils) is a site of active HIV replication and viral reservoir even in patients on antiretroviral therapy with undetectable plasma viral loads. Recall also that Epstein-Barr virus (EBV) and Human Herpesvirus-8 (HHV-8/KSHV) are key co-pathogens in HIV-related head and neck disease.
Clinical Presentation: ENT Manifestations as the Window to HIV
The clinical presentation of HIV in the head and neck spans a remarkably wide range — from the early, relatively minor changes of oral candidiasis and recurrent aphthous ulcers seen at CD4 counts of 200–500, to the potentially life-threatening conditions of Kaposi's sarcoma of the larynx and non-Hodgkin lymphoma causing airway compromise at very low CD4 counts. The most important clinical skill at this level is pattern recognition — learning to see a group of head and neck findings as a coherent clinical picture consistent with immunodeficiency, rather than treating each lesion in isolation. This is not just an academic exercise; in practice, a doctor who recognises that oral hairy leukoplakia plus bilateral parotid swellings plus cervical lymphadenopathy form a single clinical constellation will test for HIV and enable early intervention, while a doctor who treats each finding separately will miss the diagnosis. The presentation is broadly organised by stage of immunosuppression, with the CD4 count providing the immunological context for interpreting which conditions are possible.
The patterns most important to recognise are:
Early (CD4 relatively preserved, 200–500 cells/μL):
- Oral candidiasis: white removable plaques (pseudomembranous type) or erythematous patches on the tongue, buccal mucosa, or palate.
- Oral hairy leukoplakia (OHL): corrugated white patches on the lateral borders of the tongue that cannot be wiped off (unlike candida).
- Recurrent aphthous ulcers: painful oral ulcers, often larger (major type) and more refractory than in HIV-negative individuals.
- Persistent generalised lymphadenopathy (PGL): bilateral, non-tender cervical and axillary lymphadenopathy in an asymptomatic patient.
Intermediate/advancing immunosuppression (CD4 100–200 cells/μL):
- Kaposi's sarcoma (KS) of the oral cavity and oropharynx: violaceous (purple-red) patches or nodules on the hard palate, gingiva, or oropharyngeal mucosa — the most common AIDS-defining malignancy, caused by HHV-8.
- HIV-associated lymphoepithelial cysts: bilateral fluctuant swellings of the parotid glands, caused by intraglandular lymphoid hyperplasia with cystic change.
- Recurrent and refractory sinusitis: standard pathogens (Streptococcus pneumoniae, Haemophilus influenzae) initially, with fungal sinusitis (Aspergillus, mucormycosis) emerging at very low CD4 counts.
Advanced HIV/AIDS (CD4 <100 cells/μL):
- Non-Hodgkin lymphoma (NHL) of the neck or Waldeyer's ring: B-cell NHL is the commonest lymphoma in HIV; presents as a rapidly enlarging painless neck mass or tonsillar enlargement — biopsy is essential.
- Candidal laryngitis: hoarseness, dysphagia, stridor in severely immunocompromised patients.
- Sensorineural hearing loss: multifactorial — opportunistic infections affecting the cochlea, ototoxic medications (aminoglycosides for TB, cisplatin for KS chemotherapy), and direct HIV neurotoxicity.
Immunopathology: How HIV Disrupts Host Defences in the Head and Neck
The head and neck is a particularly vulnerable region in HIV disease because the mucosal surfaces, lymphatic system, and sensory structures of this region depend critically on CD4+ T-cell-mediated immunity for defence against both common and opportunistic pathogens.
CD4 depletion and opportunistic infections in the head and neck:
As the CD4 count falls, the spectrum of pathogens that can colonise and infect the head and neck mucosal surfaces expands progressively. At CD4 counts above 500, normal mucosal defence is relatively intact and infections are predominantly from common organisms. As CD4 falls below 200, Candida albicans — a normal oral commensal — transitions from coloniser to opportunistic pathogen, producing the clinical syndromes of oral candidiasis. Oral hairy leukoplakia is driven by Epstein-Barr virus (EBV) reactivation in the squamous epithelium of the lateral tongue — the EBV replication is unchecked because CD8+ cytotoxic T-cells (which control EBV-infected cells) are functionally impaired by the HIV-driven immune dysregulation.
HHV-8 and Kaposi's sarcoma:
Kaposi's sarcoma is caused by Human Herpesvirus-8 (HHV-8, also called KSHV — Kaposi's Sarcoma-associated Herpesvirus). HHV-8 infects endothelial cells and drives spindle-cell transformation and angiogenesis, producing the characteristic violaceous vascular neoplasm. In HIV-immunosuppressed patients, the loss of immunosurveillance allows uncontrolled HHV-8 replication and KS development. The oral cavity — particularly the hard palate — is the most common non-cutaneous site. Systemic KS can involve the respiratory tract, gastrointestinal tract, and lymph nodes.
Lymphoid tissue involvement — Waldeyer's ring:
The tonsillar lymphoid tissue of Waldeyer's ring contains high concentrations of CD4+ T-cells and follicular dendritic cells — both primary targets of HIV. HIV actively replicates within Waldeyer's ring lymphoid tissue even in patients with apparently controlled plasma viral loads, making tonsillar tissue a viral reservoir. The progressive destruction of this lymphoid architecture disrupts local mucosal immunity, increasing susceptibility to upper respiratory infections and pharyngeal colonisation by pathogenic organisms.
Hearing loss mechanisms in HIV:
Sensorineural hearing loss in HIV is multifactorial: direct cochlear damage from HIV neurotropism, opportunistic infections (CMV cochleitis, cryptococcal meningitis affecting the auditory nerve), and ototoxic medications used in HIV-associated conditions — aminoglycosides (used for opportunistic TB, Mycobacterium avium complex) and cisplatin (used for KS chemotherapy). Both conductive hearing loss (from recurrent otitis media due to impaired mucosal immunity) and sensorineural loss occur with increasing frequency as CD4 counts fall.
SELF-CHECK
A 28-year-old man presents with white patches on the lateral borders of his tongue that are firm, corrugated, and cannot be wiped off. He has no fever and takes no medications. The patches have been present for 6 weeks. The diagnosis and the virus responsible are:
A. Oral candidiasis (pseudomembranous); Candida albicans
B. Oral hairy leukoplakia; Epstein-Barr virus (EBV)
C. Lichen planus; autoimmune T-cell mediated
D. Leukoplakia (pre-malignant); dysplastic squamous epithelium
Reveal Answer
Answer: B. Oral hairy leukoplakia; Epstein-Barr virus (EBV)
Oral hairy leukoplakia (OHL) classically presents as white corrugated (hairy) patches on the lateral borders of the tongue that cannot be wiped off — this is the critical distinguishing feature from oral candidiasis (pseudomembranous thrush), which produces white plaques that wipe off leaving a raw surface. OHL is caused by unchecked replication of Epstein-Barr virus (EBV) in the squamous epithelium of the tongue lateral margins — a sign of significant immunosuppression (typically CD4 <350 cells/μL) and strongly associated with HIV. It is pathognomonic of immune compromise. Lichen planus produces a lacy white pattern (Wickham's striae) on the buccal mucosa, not the lateral tongue, and is typically bilateral. Pre-malignant leukoplakia does not have the hairy corrugated surface and cannot be attributed to a specific virus.
Clinical Assessment of ENT Manifestations in HIV
The clinical assessment of a patient with known or suspected HIV must include a systematic head-to-toe ENT examination — because multiple sites are often involved simultaneously and the pattern of involvement across sites provides diagnostic and staging information that no single finding can deliver in isolation. A complete ENT assessment in the HIV-positive patient is not simply a checklist of lesions; it is a structured diagnostic encounter in which each region's findings are interpreted in the context of the patient's CD4 count, viral load, and current ART status. Without this context, an oral white lesion looks identical in an AIDS patient and a patient on short-term antibiotics; with it, the significance and urgency of the finding becomes immediately clear. The five anatomical regions that must be systematically assessed are: the oral cavity and oropharynx, the neck and parotid glands, the ears, the nasal cavity and sinuses, and the larynx.
Oral cavity and oropharynx:
- Inspect the tongue (dorsum, lateral borders, ventral surface), buccal mucosa, hard and soft palate, gingiva, floor of mouth, and tonsillar pillars under adequate lighting.
- White lesions: can they be wiped off? Wiped off = candida. Cannot be wiped off on lateral tongue = OHL. Cannot be wiped off on buccal mucosa with lacy pattern = lichen planus.
- Purple/red lesions on the hard palate or gingiva: flat violaceous patches = Kaposi's sarcoma; firm nodule = may also be KS, or NHL.
- Ulcers: aphthous pattern (round, punched-out, grey base) vs irregular ulcers (suggest NHL, CMV, fungal).
- Gingival disease: linear gingival erythema (HIV gingivitis) or necrotising ulcerative gingivitis/periodontitis — exaggerated, rapid-onset periodontal disease is characteristic of HIV.
Neck and parotid examination:
- Lymph nodes: persistent generalised lymphadenopathy = bilateral, multiple group, non-tender, firm nodes. Any single asymmetric, rapidly enlarging, or hard node raises concern for NHL or KS.
- Parotid glands: bilateral soft, fluctuant parotid swellings = HIV-associated lymphoepithelial cysts (benign); bilateral firm enlargement without fluctuance = sarcoidosis, lymphoma.
Ear: Otoscopy — middle ear effusion, perforations (recurrent OM), otitis externa; whisper test or pure-tone audiometry for hearing loss.
Nose and sinuses: Anterior rhinoscopy — nasal polyps (often bilateral in allergic rhinitis but can be unilateral in HIV-related fungal sinusitis); examine for mucosal pallor or ulceration. Sinus tenderness on palpation.
Staging investigations to guide ENT assessment:
The CD4 count and plasma viral load provide the immunological context for interpreting clinical findings and guide the expected spectrum of pathogens. A CD4 count of 400 with oral candidiasis suggests early-moderate immunosuppression; the same candida with a CD4 of 50 suggests advanced AIDS with risk of other opportunistic infections.
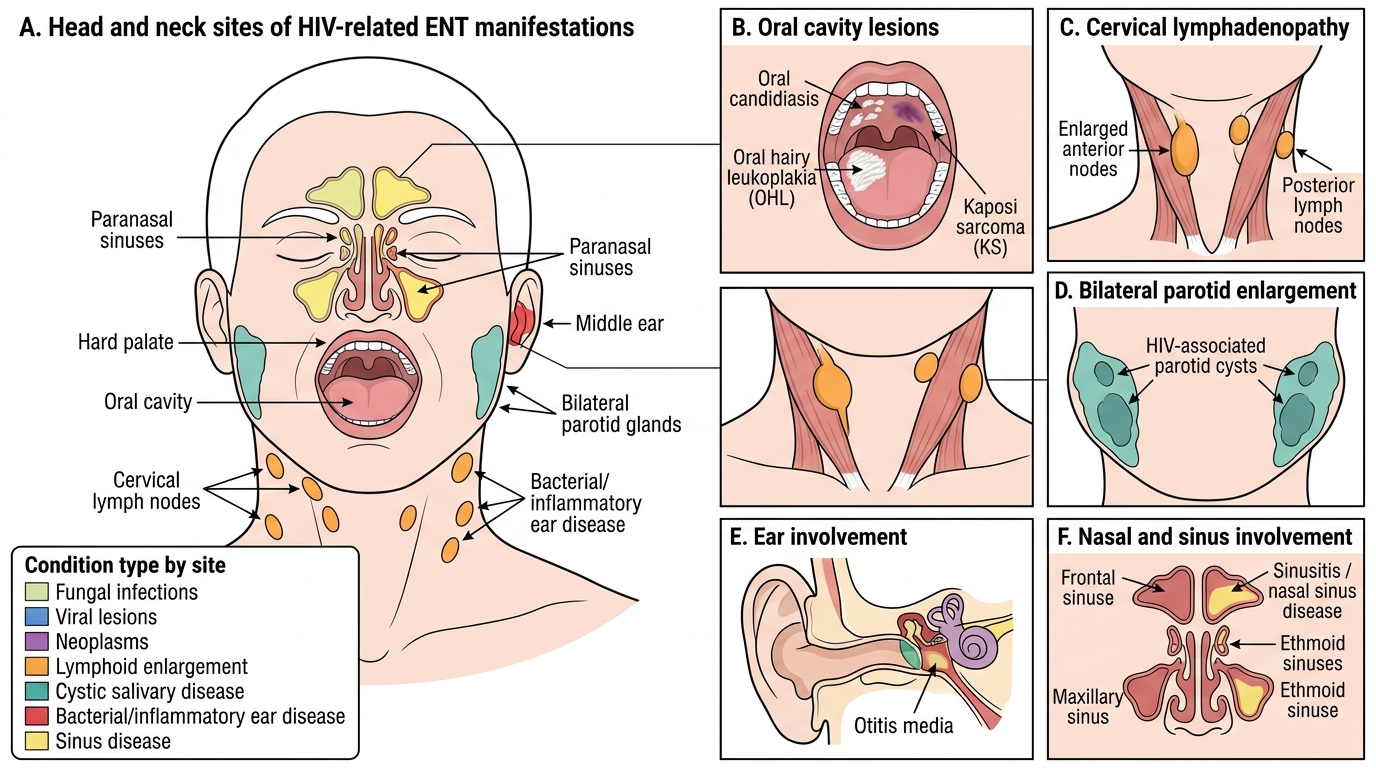
HIV-Related ENT Manifestations in the Head and Neck