Page 1 of 20
EN4.40 | Hoarseness of Voice — SDL Guide
Learning Objectives
- Elicit, document and present a systematic history of hoarseness of voice including duration, character, associated features and risk factors
- Describe the clinical features that distinguish benign vocal cord lesions, inflammatory conditions, vocal cord palsy and laryngeal malignancy
- Choose appropriate investigations for a patient presenting with hoarseness, including the role and findings of indirect laryngoscopy
- Describe the principles of management of the major causes of hoarseness
INSTRUCTIONS
Hoarseness is one of the most common laryngeal complaints encountered in ENT practice and general outpatient settings in India. Most causes are benign and easily managed, but persistent hoarseness carries the critical risk of underlying laryngeal malignancy — a risk that increases steeply with tobacco use, alcohol intake and duration beyond three weeks. This SDL builds from clinical presentation through anatomy, examination, diagnosis and management, equipping you with the systematic approach needed to distinguish a self-limiting laryngitis from a life-threatening carcinoma.
References
- Dhingra PL, Dhingra S — Diseases of Ear, Nose and Throat and Head and Neck Surgery, 8th ed., Ch. 64-68 (textbook)
- Hazarika P, Nayak DR — Textbook of ENT and Head and Neck Surgery, 3rd ed., Ch. 40-44 (textbook)
- Gleeson M et al — Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol 2, Larynx chapters (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 52-year-old male schoolteacher presents to the ENT OPD with a three-month history of progressively worsening hoarseness. He initially attributed it to overuse of his voice during examinations, but the hoarseness has persisted through the vacation period. He is a 30-pack-year smoker. On indirect laryngoscopy, you see an irregular thickening along the free edge of the left vocal cord with impaired mobility. The cord is not completely fixed, but the mucosa looks irregular. What is your working diagnosis, and what is the single most important investigation you will order? And if a student tells you this patient simply has 'chronic laryngitis' from smoking — what would you say to them?
WHY THIS MATTERS
Hoarseness of voice — a change in the quality, pitch or volume of the voice caused by abnormal vibration of the vocal folds — is among the ten most common presenting complaints in ENT practice in India. The vast majority of cases are benign: acute viral laryngitis that resolves with voice rest, or benign vocal cord lesions in professional voice users. However, hoarseness is also the earliest and most treatable symptom of glottic carcinoma, which constitutes roughly 60% of laryngeal cancers. The cruel epidemiology is this: a patient with early glottic carcinoma may have only hoarseness, no pain, no dysphagia, no neck mass — and yet T1 glottic carcinoma has a five-year survival of over 90% with radiotherapy. Delayed diagnosis, even by a few months, can convert a T1 to a T3 lesion and reduce survival to 60%. Every clinician who sees a patient with persistent hoarseness carries the responsibility for this gate-keeping. The EN4.40 competency operationalises that responsibility: you must be able to elicit the history, perform the examination, and choose the right investigations so that no laryngeal carcinoma is missed.
RECALL
Before approaching hoarseness clinically, recall three foundational concepts from your pre-clinical years. First, from anatomy: the larynx is formed by the thyroid cartilage (largest, V-shaped shield anteriorly), the cricoid cartilage (signet-ring shaped, only complete cartilaginous ring of the airway), and the paired arytenoid cartilages (which rotate to open and close the glottis). The intrinsic laryngeal muscles are all innervated by the recurrent laryngeal nerve (RLN) except the cricothyroid (external branch of superior laryngeal nerve). Critically, the posterior cricoarytenoid muscle is the sole abductor of the vocal cords — bilateral RLN palsy paralyses this muscle, causing the cords to lie in the paramedian position and producing life-threatening stridor. Second, from physiology: voicing requires the vocal folds to be adducted (brought together) so that exhaled air sets them into oscillation via the Bernoulli effect — as air flows through the narrowed glottis, subglottic pressure drops and pulls the cords together; elastic recoil separates them, creating a vibrating mucosal wave. Any lesion disrupting this wave — a mass, oedema, scar, paralysis — changes the vibratory pattern and produces hoarseness. Third, from pathology: the laryngeal mucosa overlying the vocal fold body is loosely attached to the deeper ligament by Reinke's space, a potential space filled with sparse connective tissue — a space that is significant both in disease (Reinke's oedema from smoking) and in surgery (microlaryngoscopy exploits this plane).
Clinical Presentation and Significance of Hoarseness
A complete and structured history of hoarseness is the foundation of the clinical assessment. Voice change can arise from any structural or neurological disruption of the vocal folds, and the history alone narrows the differential substantially before any instrument is introduced.
Duration is the single most important discriminator. Hoarseness lasting less than two to three weeks is almost always inflammatory — acute laryngitis following an upper respiratory infection, vocal overuse, or inhalation of irritants. Hoarseness persisting beyond three weeks is the threshold at which laryngoscopy becomes mandatory; this is the internationally recognised red-flag duration for laryngeal malignancy and must be memorised without qualification.
Character of voice change offers further clues. A rough, low-pitched, fatigable voice that worsens through the teaching day is consistent with vocal cord nodules or laryngitis. A breathy, weak, 'whispery' voice that fails to build volume suggests a gap at the glottis — either a paralysed cord or a large mass. A strained, effortful, high-pitched voice with pitch breaks may indicate muscle tension dysphonia or spasmodic dysphonia. Sudden onset dysphonia after shouting or vigorous singing may indicate a vocal cord haemorrhage (a haemorrhagic polyp).
Associated symptoms must be systematically enquired:
- Dysphagia (difficulty swallowing) — if present with hoarseness, raises concern for hypopharyngeal or oesophageal extension of laryngeal disease, or a pharyngeal mass.
- Dyspnoea (breathlessness) or stridor — indicates significant supraglottic or bilateral glottic involvement; bilateral cord palsy is an emergency.
- Odynophagia (painful swallowing) — uncommon in early glottic carcinoma; its presence suggests supraglottic involvement or acute infection.
- Neck mass — cervical lymphadenopathy alongside hoarseness in a smoker is highly suspicious for laryngeal malignancy with nodal spread (typically supraglottic).
- Unintentional weight loss, haemoptysis, otalgia (referred pain via the vagus to the ear) — these constitute the 'alarm symptoms' of laryngeal carcinoma.
Occupational voice use is essential context: teachers, singers, call-centre workers and public speakers subject the vocal folds to high-demand phonation and are at risk of benign vocal fold lesions (nodules, contact ulcers) related to mechanical trauma.
Risk factors for malignancy must be documented explicitly: tobacco smoking (by far the most important risk factor; dose-dependent; synergistic with alcohol), alcohol use, exposure to industrial carcinogens (wood dust, nickel, asbestos), and prior radiation to the neck.
Gastro-oesophageal and laryngopharyngeal reflux is an underappreciated cause of chronic hoarseness in non-smokers; patients may deny heartburn (silent reflux) but describe morning hoarseness, voice warming up through the day, excess throat-clearing, and a sensation of mucus in the throat.
A high-yield history summary: when a patient presents with hoarseness, the ENT resident must document — onset and duration, character of voice change, associated alarm symptoms (dysphagia, stridor, otalgia, weight loss, neck mass), voice demand and occupation, smoking and alcohol history, reflux symptoms, and prior ENT history or radiotherapy.
Anatomy and Pathophysiology of Voice Production
Understanding why a particular laryngeal lesion produces a characteristic voice quality requires a working knowledge of the multilayered structure of the vocal fold and the mechanics of phonation.
The vocal fold (or true vocal cord) is not a simple cord but a layered structure composed of five histological layers. From deep to surface: the vocalis muscle (thyroarytenoid muscle — forms the body), the deep layer of the lamina propria (dense collagen and elastin fibres — the 'vocal ligament'), the intermediate layer (predominantly elastin), the superficial layer of the lamina propria — known as Reinke's space (loose areolar tissue, minimal cellular elements), and finally the epithelium (stratified squamous). This body-cover structure is fundamental: the epithelium and Reinke's space (the 'cover') vibrate independently of the deeper muscle-ligament 'body' during phonation, generating the mucosal wave. Any disruption to this independent cover vibration — by scar tissue (loss of the compliant Reinke's space), by a mass resting on the vocal fold surface, by oedema flooding Reinke's space, or by neurological paralysis preventing cord adduction — produces hoarseness.
During phonation, the vocal folds are adducted by the lateral cricoarytenoid and interarytenoid muscles. Subglottic air pressure builds until it exceeds the medial compression of the folds, forces them apart, creates a jet of air — and the Bernoulli effect then pulls them back together. This oscillatory cycle at approximately 100–200 Hz (fundamental frequency) creates the mucosal wave — a propagating ripple of the cover that travels from the inferior surface to the superior surface of the vocal fold. It is the mucosal wave that produces the 'warmth' and resonance of the normal voice; its absence (as in a scarred post-surgical cord) produces a thin, rough sound.
Glottic closure is equally important: if the cords fail to meet at the midline (glottic gap), air escapes continuously during voicing, producing a breathy, weak voice. A unilateral cord paralysis typically leaves a gap because the paralysed cord sits in the paramedian or lateral position while the mobile contralateral cord attempts to cross the midline.
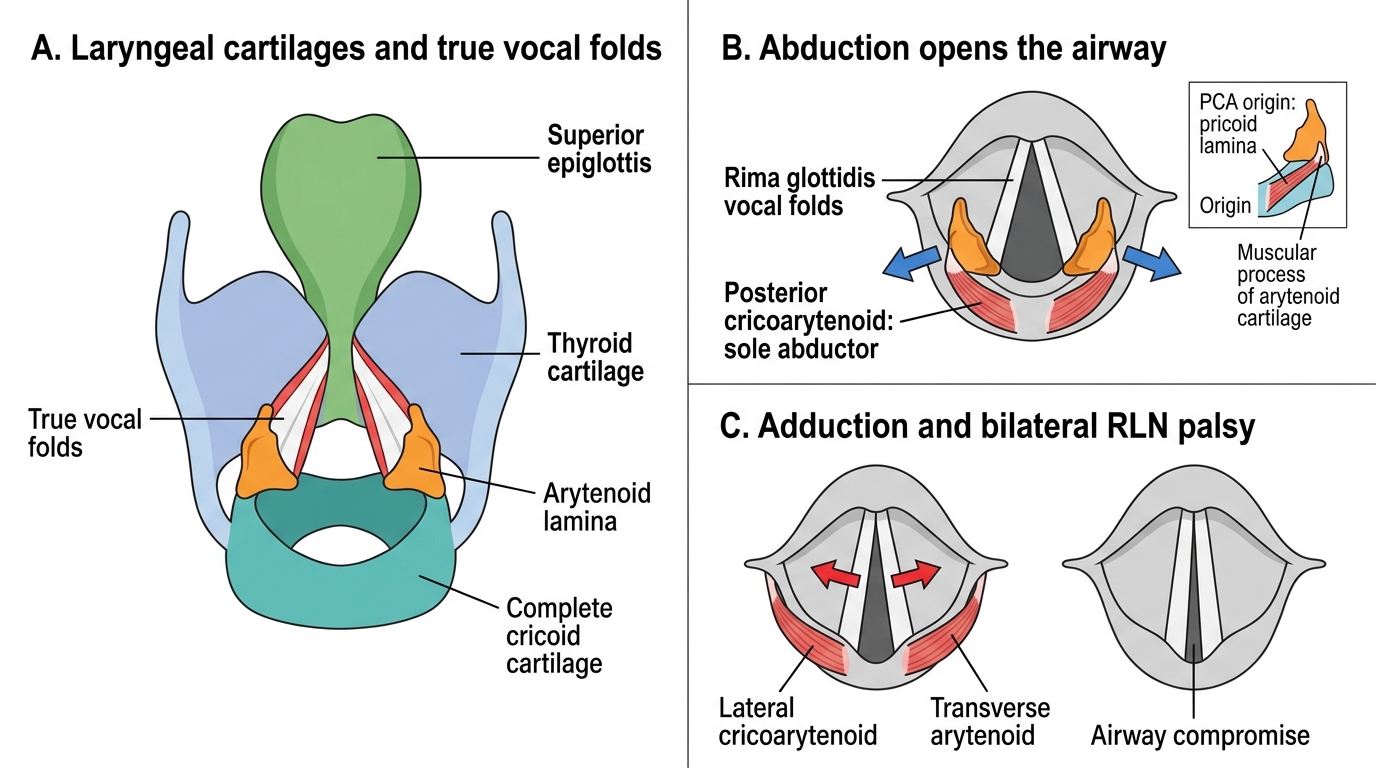
Larynx: Vocal Fold Movements and Posterior Cricoarytenoid
The posterior cricoarytenoid (PCA) muscle deserves special emphasis: it is the ONLY abductor of the vocal cords. It arises from the posterior surface of the cricoid lamina and inserts on the muscular process of the arytenoid, rotating the arytenoid laterally to pull the vocal processes apart and open the airway. In bilateral RLN palsy, the PCA on both sides is paralysed, and the cords lie adducted in the paramedian or median position — the adductor tone of the passive ligaments and cricothyroid (innervated by the external SLN, which is spared) is unopposed. This produces airway compromise requiring emergency intervention.
Recurrent Laryngeal Nerve Anatomy and Vocal Cord Palsy
Vocal cord palsy (VCP) is one of the most important causes of hoarseness in clinical practice, and understanding the anatomy of the recurrent laryngeal nerve is essential to identifying the underlying cause. The two recurrent laryngeal nerves share the same function but follow markedly different anatomical paths — a distinction that is not merely an anatomical curiosity but carries direct clinical consequences every time a clinician encounters a patient with an immobile vocal cord.
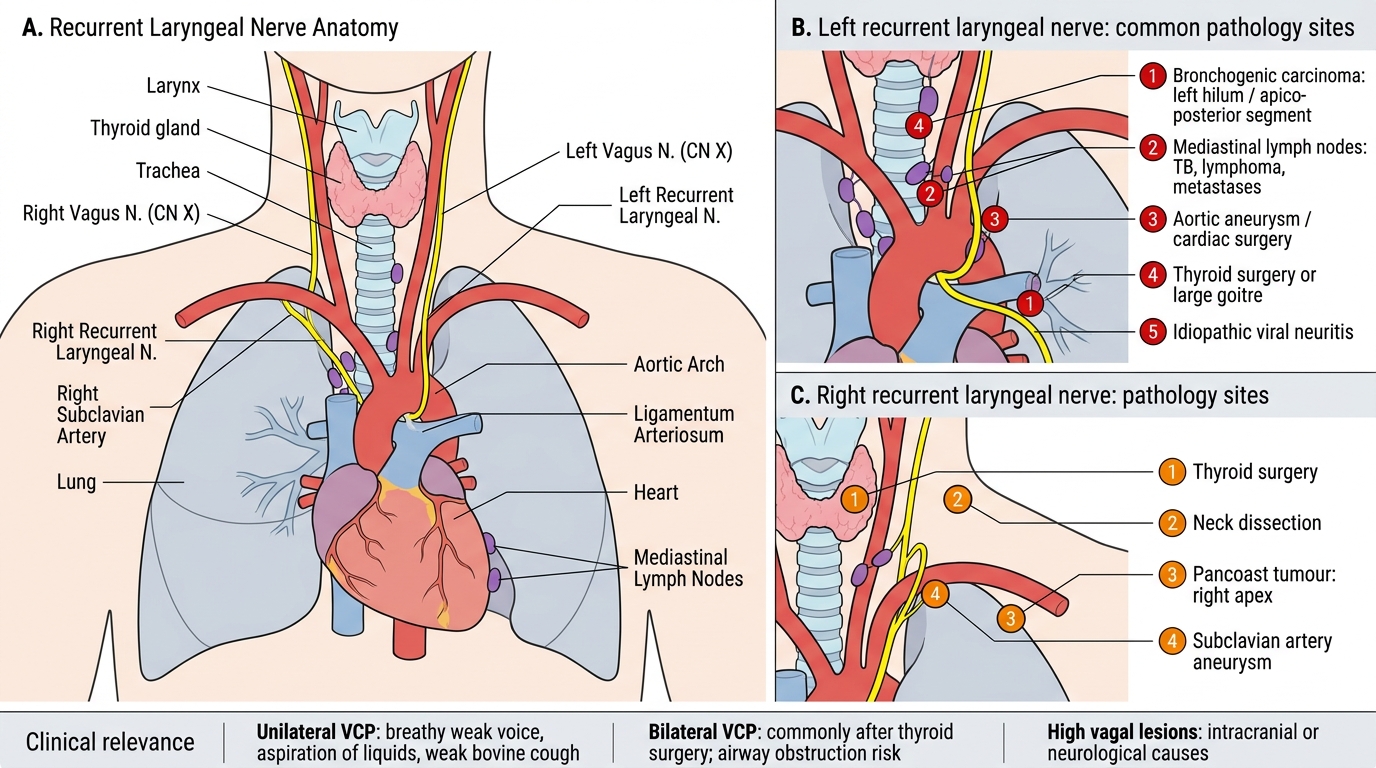
The vagus nerve (CN X) exits the skull through the jugular foramen and descends in the carotid sheath. In the thorax, it gives off the recurrent laryngeal nerve (RLN). The course of the two RLNs is anatomically asymmetric — a fact with major clinical implications. The right RLN loops under the right subclavian artery at the level of the thoracic inlet and then immediately ascends in the right tracheo-oesophageal groove to reach the larynx. Its intrathoracic course is therefore short. The left RLN, by contrast, must follow the vagus down into the posterior mediastinum before branching, looping posteriorly under the aortic arch at the level of the ligamentum arteriosum, and ascending in the left tracheo-oesophageal groove to the larynx. This extended intrathoracic arc means the left RLN travels close to the left hilar lymph nodes, the aortic arch, and the left main pulmonary artery before it reaches the larynx — making it vulnerable to any mass or lymphadenopathy in the superior mediastinum or left hilum. This anatomical asymmetry is why isolated left vocal cord palsy is far more common than right, and why its workup demands thoracic imaging as a priority.
- Right RLN: loops under the right subclavian artery at the thoracic inlet and ascends in the tracheo-oesophageal groove to enter the larynx.
- Left RLN: has a longer intrathoracic course — it descends into the chest, loops under the aortic arch (at the level of the ligamentum arteriosum/ductus arteriosus), and then ascends in the tracheo-oesophageal groove to the larynx. This longer course, looping around the aortic arch, makes the left RLN vulnerable to mediastinal pathology in a way the right RLN is not.
Recurrent Laryngeal Nerves and Vocal Cord Palsy
Causes of left VCP (in approximate order of frequency in India):
- Bronchogenic carcinoma (left hilum/apico-posterior segment) — commonest single cause of left VCP in adults; the left main bronchus and left hilar nodes lie close to the aortic arch where the nerve loops
- Mediastinal pathology — enlarged mediastinal lymph nodes (tuberculosis, lymphoma, metastases), aortic aneurysm, cardiac surgery
- Thyroid — thyroid surgery (most common iatrogenic cause), or large goitre
- Idiopathic — viral neuritis (herpes simplex, Epstein-Barr); approximately 20% remain unexplained after full workup
Causes of right VCP: thyroid surgery, neck dissection, apical lung tumour (Pancoast tumour at right apex), subclavian artery aneurysm.
Causes of bilateral VCP: thyroid surgery (the single most common cause globally), bilateral thyroid malignancy, neck irradiation, intracranial pathology (high vagal lesions), neurological disorders (Parkinson's disease, multiple system atrophy).
Clinical presentation of VCP:
- Unilateral VCP: breathy, weak dysphonia; aspiration of liquids (particularly water) because the glottis fails to close for swallowing; cough may be weak and ineffective ('bovine cough'). The patient can often compensate by increasing subglottic pressure, but the voice is effortful and fatigable.
- Bilateral VCP: presents with stridor (inspiratory > expiratory) due to bilateral adduction of the cords producing a small fixed glottic opening; voice may be surprisingly reasonable because the cords are adducted close to the midline. The cardinal danger is respiratory obstruction — particularly during sleep, upper respiratory infection, or exercise.
SELF-CHECK
A 58-year-old male smoker presents with four weeks of hoarseness and a weak 'bovine cough'. On indirect laryngoscopy, the left vocal cord is immobile and lies in the paramedian position; the right cord is mobile and crosses the midline during phonation. There is no neck mass. The most important next investigation is:
A. Direct laryngoscopy and biopsy of the left cord
B. Contrast-enhanced CT scan of the chest from thoracic inlet to the diaphragm
C. Thyroid function tests and ultrasound of the neck only
D. MRI of the brain to exclude intracranial vagal lesion
Reveal Answer
Answer: B. Contrast-enhanced CT scan of the chest from thoracic inlet to the diaphragm
Unilateral left vocal cord palsy in a smoker requires systematic imaging of the entire course of the left RLN — from the skull base through the neck, thoracic inlet, mediastinum and hilum, to the larynx. The left RLN loops under the aortic arch, making mediastinal and hilar causes (bronchogenic carcinoma, TB nodes, lymphoma) the most important to exclude. A contrast CT chest from thoracic inlet to diaphragm is the single most informative investigation. A neck ultrasound/TFT alone would miss a chest lesion; direct laryngoscopy confirms the palsy but does not find the cause; MRI brain is appropriate for bilateral or high-vagal lesions, not isolated left VCP.