Page 7 of 20
EN4.42 | Malignancy of Larynx Hypopharynx — SDL Guide
Learning Objectives
- Describe the clinical features of laryngeal carcinoma by anatomical subsite (glottic, supraglottic, subglottic) and explain how subsite determines prognosis
- Describe the clinical features, investigations and staging of hypopharyngeal carcinoma including the association with Plummer-Vinson syndrome
- Choose appropriate investigations and describe staging classification for laryngeal and hypopharyngeal malignancy
- Describe the principles of management including organ-preservation and surgical approaches for different stages
INSTRUCTIONS
Laryngeal carcinoma is one of the most common head and neck cancers in India, strongly associated with tobacco use and alcohol. The prognosis varies dramatically by subsite — a T1 glottic carcinoma caught early because of early hoarseness has a cure rate exceeding 90%, whereas a supraglottic carcinoma presenting late with bilateral cervical nodes may have a five-year survival below 40%. Understanding the anatomy of the larynx — particularly the lymphatic supply of each subsite — is the key to understanding why the same histological tumour (squamous cell carcinoma) behaves so differently depending on where it arises.
References
- Dhingra PL, Dhingra S — Diseases of Ear, Nose and Throat and Head and Neck Surgery, 8th ed., Ch. 71-75 (textbook)
- Hazarika P, Nayak DR — Textbook of ENT and Head and Neck Surgery, 3rd ed., Ch. 47-52 (textbook)
- Gleeson M et al — Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol 2, Laryngeal and hypopharyngeal cancer chapters (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two men are referred to the ENT OPD on the same day. The first, a 55-year-old teacher and smoker, has had hoarseness for five weeks; he is otherwise well and has no neck mass. On indirect laryngoscopy, you see an irregular, slightly thickened area on his left true vocal cord. The second, a 60-year-old farmer, has had progressive difficulty swallowing solids for three months, with unintentional weight loss and bilateral firm cervical lymphadenopathy. His voice is only mildly hoarse. Both have laryngeal carcinoma — but the staging, the treatment, and the prognosis could not be more different. Why does the first man have excellent prospects while the second's are guarded, even though both are at a similar 'stage' of symptom duration? The answer lies in the lymphatic anatomy of the larynx.
WHY THIS MATTERS
Laryngeal carcinoma is the most common malignancy of the head and neck in India after oral cavity cancers. It constitutes approximately 5% of all cancers in Indian men, with tobacco smoking and gutka/betel-nut use being the dominant risk factors. Hypopharyngeal carcinoma is rarer but carries an even worse prognosis. Together these cancers claim thousands of lives annually in India — most of them preventable, and many diagnosed too late because the early symptom of hoarseness is dismissed by the patient or misattributed to 'throat infection' at the primary-care level. The public-health importance of the >3 weeks hoarseness rule, which you learned in the EN4.40 SDL, is directly tied to these cancers — glottic carcinoma at T1 is essentially curable, but the same tumour at T3 (cord fixation) halves the survival. As a final-year MBBS student, you will be the first clinician many of these patients see. Recognising the red flags, choosing the right investigation, and making the correct referral is a life-saving skill.
RECALL
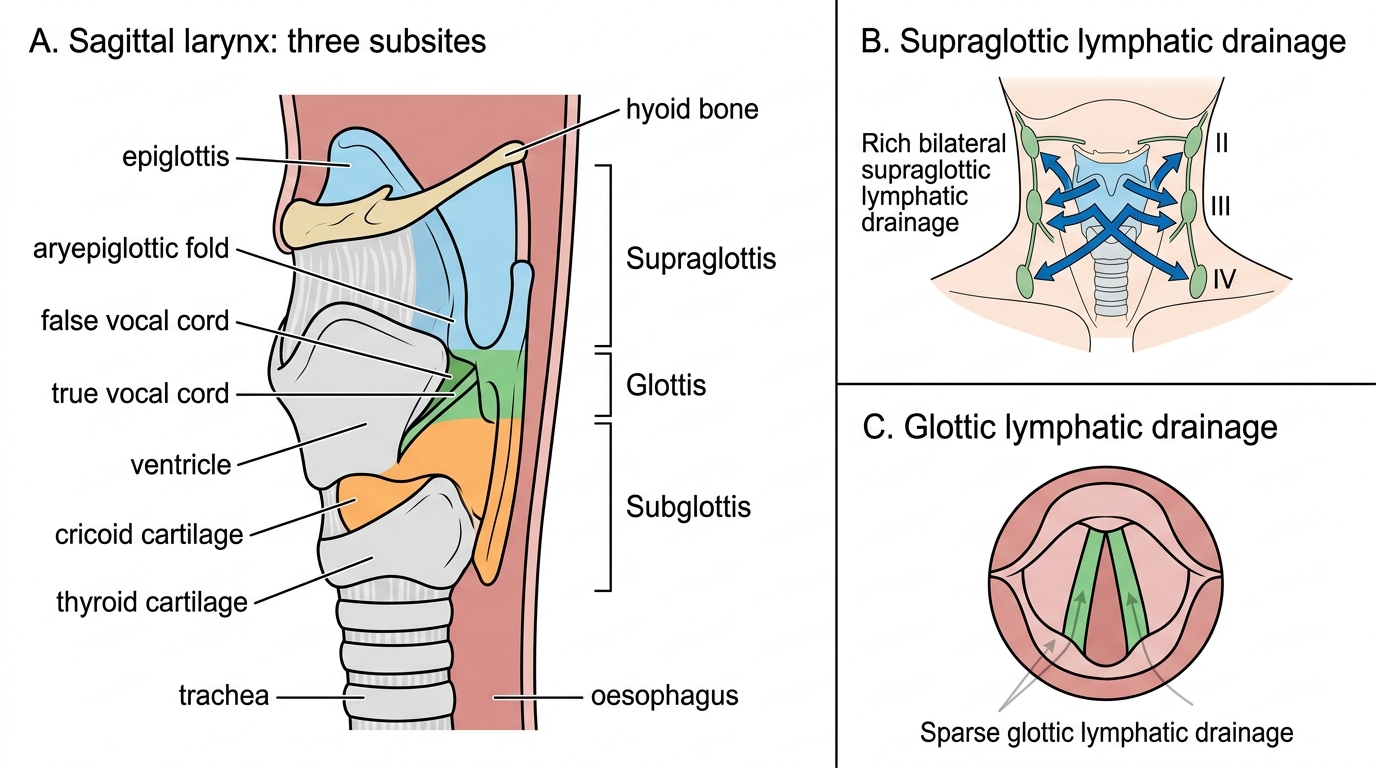
Recall from the EN4.40 SDL the three anatomical subsites of the larynx and their critical lymphatic differences. The glottis (true vocal cords, anterior and posterior commissures) is almost devoid of lymphatics — which is why glottic tumours spread locally along the cord and rarely produce early cervical node metastases, giving them an inherently better prognosis. The supraglottis (epiglottis, aryepiglottic folds, false cords, arytenoids) has a rich bilateral lymphatic supply draining to both sets of jugulodigastric and deep cervical lymph nodes — which is why supraglottic tumours spread early and bilaterally to cervical nodes. The subglottis (below the cords to the lower edge of the cricoid) is rare as a primary site but has lymphatics draining to the paratracheal and mediastinal nodes, and carries a poor prognosis. Recall also that cord fixation — the inability of a vocal cord to abduct on laryngoscopy — is a specific staging criterion (T3) indicating invasion of the cricoarytenoid joint or the thyroarytenoid muscle, significantly worsening the prognosis.
Clinical Presentation of Laryngeal and Hypopharyngeal Malignancy
The presenting symptoms of laryngeal and hypopharyngeal malignancy are determined by the subsite of origin. The single most important clinical principle is that different subsites have different 'sentinel symptoms' — the symptom that appears earliest — and these differ precisely because of the differing proximity of each subsite to the vocal cords and to the regional lymphatics.
Glottic carcinoma presents with hoarseness as the earliest symptom, typically of gradual onset over weeks to months. Because the true vocal cord vibrates with every voicing effort, even a small tumour disrupts the mucosal wave and changes the voice quality. This early symptom is clinically important because it allows detection at a time when the tumour is still confined and curable. Late symptoms in glottic carcinoma include dyspnoea and stridor (when the tumour is large enough to obstruct the glottis), dysphagia (when it has spread to the hypopharynx), and referred otalgia (via the vagal-auricular reflex — pain referred to the ear via the auricular branch of the vagus). Cervical lymphadenopathy is uncommon in early glottic carcinoma due to the sparse lymphatic supply.
Supraglottic carcinoma presents with a different pattern — hoarseness is a LATE symptom, appearing only when the tumour has spread downward to involve the true cords. The early symptoms are dysphagia (difficulty swallowing, particularly solids), odynophagia (painful swallowing), a sensation of a foreign body in the throat, and — most importantly — a painless neck mass from metastatic cervical lymphadenopathy. This is why patients with supraglottic carcinoma so often present at an advanced stage with bilateral nodal disease despite appearing to have only mild voice change: the first symptom (neck lump or dysphagia) may be erroneously attributed to a benign cause.
Subglottic carcinoma is rare (~5% of laryngeal cancers) and may present with stridor as its first symptom when the tumour grows to obstruct the subglottic airway. Hoarseness appears only when the tumour extends upward to involve the cords. It carries the worst prognosis of the three subsites.
Hypopharyngeal carcinoma typically presents late. The three subsites — piriform sinus (the commonest, accounting for about 60-65% of hypopharyngeal carcinomas), posterior pharyngeal wall, and postcricoid region — all present with progressive dysphagia (initially for solids, then liquids), unintentional weight loss, and a neck mass. Hoarseness may be absent until the tumour extends to involve the larynx. Postcricoid carcinoma has an important association with Plummer-Vinson syndrome (also called Patterson-Kelly-Brown syndrome) — a triad of iron-deficiency anaemia, dysphagia from a post-cricoid web, and koilonychia, occurring predominantly in middle-aged women. The presence of this syndrome identifies a population at elevated risk of postcricoid carcinoma.
Risk factors common to all subtypes: tobacco smoking (the dominant risk factor, multiplicative with alcohol), alcohol use, occupational exposure to wood dust (nasopharynx and hypopharynx) and asbestos, laryngopharyngeal reflux (a chronic irritant and potential carcinogen), and prior head and neck irradiation. Iron-deficiency anaemia specifically relates to postcricoid risk.
| Subsite | First symptom | Lymphatics | Typical stage at presentation | Prognosis (5yr) |
|---|---|---|---|---|
| Glottic | Hoarseness (early) | Sparse | T1-T2 | Excellent (T1: >90%) |
| Supraglottic | Dysphagia, neck mass | Rich bilateral | T3-T4 with N+ | Moderate (50-60%) |
| Subglottic | Stridor (late) | Paratracheal | T3-T4 | Poor (<50%) |
| Piriform sinus | Dysphagia, neck mass | Rich | T3-T4 with N+ | Poor (30-40%) |
| Postcricoid | Dysphagia, weight loss | Rich | Advanced | Poor (<30%) |
Anatomy, Pathology and Spread of Laryngeal Carcinoma
Understanding the pathology and spread of laryngeal carcinoma requires integration of the anatomy of each subsite with the biology of squamous cell carcinoma. Laryngeal carcinoma is squamous cell carcinoma (SCC) in over 95% of cases — arising from the stratified squamous epithelium of the laryngeal mucosa, usually on a background of dysplastic change driven by years of tobacco and alcohol exposure.
Macroscopically, laryngeal carcinomas may be: exophytic (warty, cauliflower-like growths projecting into the laryngeal lumen — tend to be well-differentiated and less invasive), ulcerative (deeply ulcerated lesion with firm edges — suggests aggressive invasion), or infiltrative (diffuse thickening and fixation without a discrete lesion margin). The clinical significance is that exophytic tumours are often caught earlier and have a better prognosis, whereas infiltrative tumours may be understaged because the full extent of invasion is not apparent on endoscopy alone.
The pattern of spread is governed by anatomical barriers and lymphatics. Within the larynx, tumours spread along mucosal surfaces and via the Reinke's space plane; they can penetrate the paraglottic space (fatty space between the thyroid cartilage and the inner laryngeal mucosa), the pre-epiglottic space (between the epiglottis and the thyrohyoid membrane — a route by which supraglottic tumours can reach the base of tongue), and eventually erode cartilage (thyroid or cricoid cartilage invasion = T4a disease).
Lymph node spread follows the lymphatic drainage of each subsite. Glottic tumours, because of their sparse lymphatics, rarely produce cervical nodes at presentation — this is the fundamental reason for their excellent prognosis at T1. Supraglottic tumours drain bilaterally to the jugulodigastric (level II), internal jugular chain (levels III-IV), and suprahyoid nodes, producing bilateral cervical node metastases in 20-30% of even clinically N0 supraglottic tumours (occult nodal disease). This 'occult N+' rate is the reason prophylactic (elective) neck dissection is recommended even for N0 supraglottic disease.
Distant spread occurs via haematogenous routes, most commonly to the lungs. Distant metastases are uncommon at presentation (unlike nasopharyngeal carcinoma) but become more likely with advanced N3 disease.
Laryngeal Subsites and Lymphatic Drainage
Hypopharyngeal Carcinoma
Hypopharyngeal carcinoma arises in the hypopharynx — the posterior wall of the pharynx between the oropharynx above and the oesophagus below, extending from the level of the hyoid bone to the lower border of the cricoid cartilage. It is divided into three anatomical subsites, each with distinct clinical associations and prognosis.
The piriform sinus (or fossa) is the bilateral pear-shaped recess on either side of the larynx, lateral to the aryepiglottic folds. It is the commonest site of hypopharyngeal carcinoma, accounting for approximately 60-65% of cases. Piriform sinus carcinoma typically presents with unilateral dysphagia, referred otalgia (ipsilateral), and a neck mass from cervical lymphadenopathy. Hoarseness occurs when the tumour extends medially to involve the larynx or directly invades the recurrent laryngeal nerve or cricoarytenoid joint. Because the piriform fossa is a silent area — tumours grow here without early symptoms — these cancers are often at T3 or T4 at the time of diagnosis.
The posterior pharyngeal wall is the rarest site; its carcinoma presents with dysphagia, odynophagia, and neck pain. It has a particularly poor prognosis because of the proximity of the prevertebral fascia (invasion of which makes resection impossible) and because bilateral cervical nodal metastases are common.
The postcricoid region is the area at the junction of the hypopharynx and the oesophagus, just behind the cricoid cartilage. This is the site where Plummer-Vinson syndrome (also called Patterson-Kelly syndrome) predisposes to carcinoma. The syndrome comprises: iron-deficiency anaemia (causing mucosal atrophy and the postcricoid web), dysphagia from the web, and brittle nails (koilonychia) — occurring predominantly in middle-aged women of Northern European and South Asian origin. The web itself is a thin mucosal shelf that partially obstructs the postcricoid lumen and represents a pre-malignant lesion when found in the context of chronic iron deficiency. Management of postcricoid carcinoma is surgical (pharyngolaryngectomy with reconstruction) but prognosis is poor.
All three hypopharyngeal subsites drain to the cervical lymph nodes, and approximately 70% of patients with hypopharyngeal carcinoma have palpable cervical nodal metastases at presentation. The overall five-year survival for hypopharyngeal carcinoma is approximately 25-35% — significantly worse than for laryngeal carcinoma — because of late presentation, rich lymphatics, and the propensity for early submucosal spread and skip metastases.
SELF-CHECK
A 62-year-old male smoker is referred with a two-month history of progressive dysphagia and a 3 cm firm left jugulodigastric lymph node. His voice is normal. On flexible fibre-optic nasolaryngoscopy, you see an irregular, friable lesion in the left piriform fossa. The most appropriate next step is:
A. Indirect laryngoscopy only and reassure if the cords are mobile
B. Panendoscopy (triple endoscopy) under general anaesthesia with biopsy of the piriform sinus lesion and staging CT of neck and chest
C. Fine needle aspiration cytology (FNAC) of the neck node and await results before further investigation
D. Empirical radiotherapy for presumed squamous cell carcinoma
Reveal Answer
Answer: B. Panendoscopy (triple endoscopy) under general anaesthesia with biopsy of the piriform sinus lesion and staging CT of neck and chest
This presentation — progressive dysphagia, cervical lymphadenopathy, and a visible lesion in the piriform sinus in a smoker — is hypopharyngeal carcinoma until proven otherwise. The next step is panendoscopy (laryngoscopy + oesophagoscopy + bronchoscopy) under general anaesthesia with biopsy to obtain histological confirmation, assess the full extent of the lesion, and detect synchronous primaries (second primary tumours in the oesophagus or bronchus occur in ~5-10% of head and neck cancer patients). Staging CT of the neck and chest should also be obtained to assess nodal disease, cartilage invasion, and pulmonary metastases. FNAC of the node alone provides cytology but not the primary histology; empirical radiotherapy without histological diagnosis is inappropriate. IDL alone is insufficient — panendoscopy provides complete assessment of the hypopharynx.