Page 10 of 20
EN4.43 | Stridor — SDL Guide
Learning Objectives
- Define stridor and distinguish it from related sounds (stertor, wheeze); use the phase of stridor to localise the level of airway obstruction
- Describe the common causes of stridor by age group including laryngomalacia, croup, epiglottitis, bilateral vocal cord palsy, and subglottic stenosis
- Choose appropriate investigations for a patient presenting with stridor, including immediate severity assessment
- Describe the principles of emergency and definitive management of the major causes of stridor
INSTRUCTIONS
Stridor is not a diagnosis — it is a sign. It tells you that the airway is partially obstructed, and your job is to determine where, why, and how urgently. A child who develops stridor overnight after a runny nose needs dexamethasone and monitoring. A neonate with stridor on every feed may have laryngomalacia that will self-resolve. An adult who develops stridor after thyroid surgery needs immediate assessment for bilateral recurrent laryngeal nerve palsy. Each scenario demands a different response at a different speed. This SDL builds the framework for thinking systematically about stridor — from the sound itself, through the anatomy of obstruction, to cause-specific management.
References
- Dhingra PL, Dhingra S — Diseases of Ear, Nose and Throat and Head and Neck Surgery, 8th ed., Ch. 62-63, 76 (textbook)
- Hazarika P, Nayak DR — Textbook of ENT and Head and Neck Surgery, 3rd ed., Ch. 36-38, 53 (textbook)
- Gleeson M et al — Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Paediatric ENT and Laryngology chapters (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients present to your casualty on the same night. The first is a 6-week-old infant whose mother says the baby makes a high-pitched noise every time it feeds; it is otherwise thriving and not distressed between feeds. The second is a 2-year-old child with a 48-hour history of a barking cough; she is now breathing noisily at rest with mild subcostal recessions. The third is a 55-year-old man who underwent total thyroidectomy 12 hours ago; he is now increasingly short of breath and making a harsh noise on every breath, with an SpO2 of 91%. All three patients have stridor — but the cause, urgency, and management of each are completely different. How do you triage them? Which patient do you see first? And what is the single most dangerous mistake you can make when approaching the third patient?
WHY THIS MATTERS
Stridor is a clinical emergency sign until proven otherwise. It indicates that the airway has narrowed to the point where airflow is turbulent and audible — and the anatomy of the airway means that a modest degree of further narrowing (mucosal oedema, inspissated secretions, a small mass) can convert partial obstruction into complete obstruction within minutes. Children are at higher risk than adults, not because they are more susceptible to the causes of stridor, but because their airways are proportionally much narrower — a 1 mm rim of oedema in the subglottis of an infant occupies a much higher percentage of the total airway cross-sectional area than the same oedema in an adult. This size-related vulnerability is why the same viral infection (parainfluenza) that produces a mild 'barky cough' in a toddler would be virtually asymptomatic in a teenager. The EN4.43 competency reflects the centrality of stridor in emergency ENT — every MBBS graduate must be able to assess the severity of stridor, identify its likely cause based on age and clinical context, and initiate appropriate emergency management.
RECALL
Recall from the EN4.40 and EN4.41 SDLs two foundational concepts. First, the posterior cricoarytenoid (PCA) muscle is the sole abductor of the vocal cords; bilateral recurrent laryngeal nerve palsy (for example after bilateral thyroid surgery) paralyses both PCA muscles, leaving the cords adducted in the paramedian position. The adducted cords produce a narrow glottic opening through which each breath must pass — generating inspiratory stridor and expiratory noise, with relatively preserved voice quality (because the cords, though fixed, are close to the midline and still vibrate). Second, the subglottis — the region between the undersurface of the cords and the lower border of the cricoid cartilage — is the narrowest fixed part of the upper airway in a child. The cricoid is the only complete cartilaginous ring of the airway: unlike the trachea (which has C-shaped rings with a posterior membranous wall that can expand), the cricoid is a rigid ring that cannot dilate. Oedema within this rigid ring causes the hallmark 'steeple sign' narrowing seen in croup and explains why subglottic pathology causes biphasic stridor — both inspiratory and expiratory noise — because the fixed, symmetric narrowing affects both phases of breathing.
Clinical Presentation and Recognition of Stridor
Understanding stridor begins with distinguishing it from other noisy breathing sounds and using the character of the stridor to localise the obstruction before any investigation is performed. This acoustic localisation saves both time and, in emergencies, the patient's life.
Stridor is a high-pitched, musical or harsh sound produced by turbulent airflow through a partially obstructed airway. It is predominantly heard on inspiration from supraglottic or glottic obstruction, on both inspiration and expiration (biphasic) from subglottic or tracheal obstruction, or predominantly on expiration from lower intrathoracic airway obstruction. It is typically louder with increased respiratory effort — more airflow through a fixed obstruction generates more turbulence.
Stertor (from the Latin stertere — to snore) is a lower-pitched, snoring sound produced by vibration of soft tissue in the nasopharynx or oropharynx. It is caused by adenotonsillar hypertrophy, macroglossia, obesity (obstructive sleep apnoea), or any cause of nasopharyngeal or oropharyngeal narrowing. Unlike stridor, stertor is predominantly heard during sleep; it does not indicate the same degree of fixed, rigid airway compromise.
Wheeze is a musical, predominantly expiratory sound produced by bronchospasm or lower airway narrowing within the chest — asthma, bronchiolitis, foreign body in the bronchus. It is fundamentally different from stridor because the site of obstruction is intrathoracic, distal to the larynx and trachea.
The phase of stridor provides immediate anatomical localisation:
- Inspiratory stridor: obstruction at the supraglottis or glottis (e.g., epiglottitis, laryngomalacia, bilateral VCP). The collapse of the supraglottic structures inward during inspiration narrows the glottis.
- Expiratory stridor: intrathoracic tracheal or bronchial obstruction — the increased intrathoracic pressure during expiration compresses the airway further.
- Biphasic stridor (inspiratory + expiratory): subglottic or upper tracheal obstruction (e.g., croup, subglottic stenosis, subglottic haemangioma). The rigid subglottic narrowing creates turbulence in both phases.
The age of the patient is the most powerful initial filter for the differential diagnosis of stridor, because different causes predominate at different ages. A 4-week-old infant with inspiratory stridor on feeding almost certainly has laryngomalacia; an adult with stridor of recent onset after thyroid surgery almost certainly has bilateral vocal cord palsy. This age-based reasoning should be applied immediately on clinical assessment.
Anatomy and Pathophysiology of Airway Obstruction
The severity of stridor and its clinical consequences are determined not just by the size of the obstructing lesion but by the proportional reduction in airway cross-sectional area — and this is why children experience proportionally greater obstruction from the same degree of mucosal swelling as adults.
The subglottic diameter of a newborn is approximately 4-5 mm. The adult subglottis measures approximately 15-20 mm. A 1 mm rim of circumferential oedema (as in croup or post-extubation subglottic oedema) reduces the newborn's subglottic cross-sectional area by approximately 44%; in the adult the same oedema reduces the area by only approximately 12%. Because airway resistance is inversely proportional to the FOURTH POWER of the radius (Poiseuille's law), a halving of the radius increases resistance by 16-fold. This geometric relationship explains why viral laryngotracheitis that causes mild symptoms in a 5-year-old can produce severe respiratory distress in a 6-month-old — the absolute degree of inflammation may be identical, but the proportional consequence is vastly different.
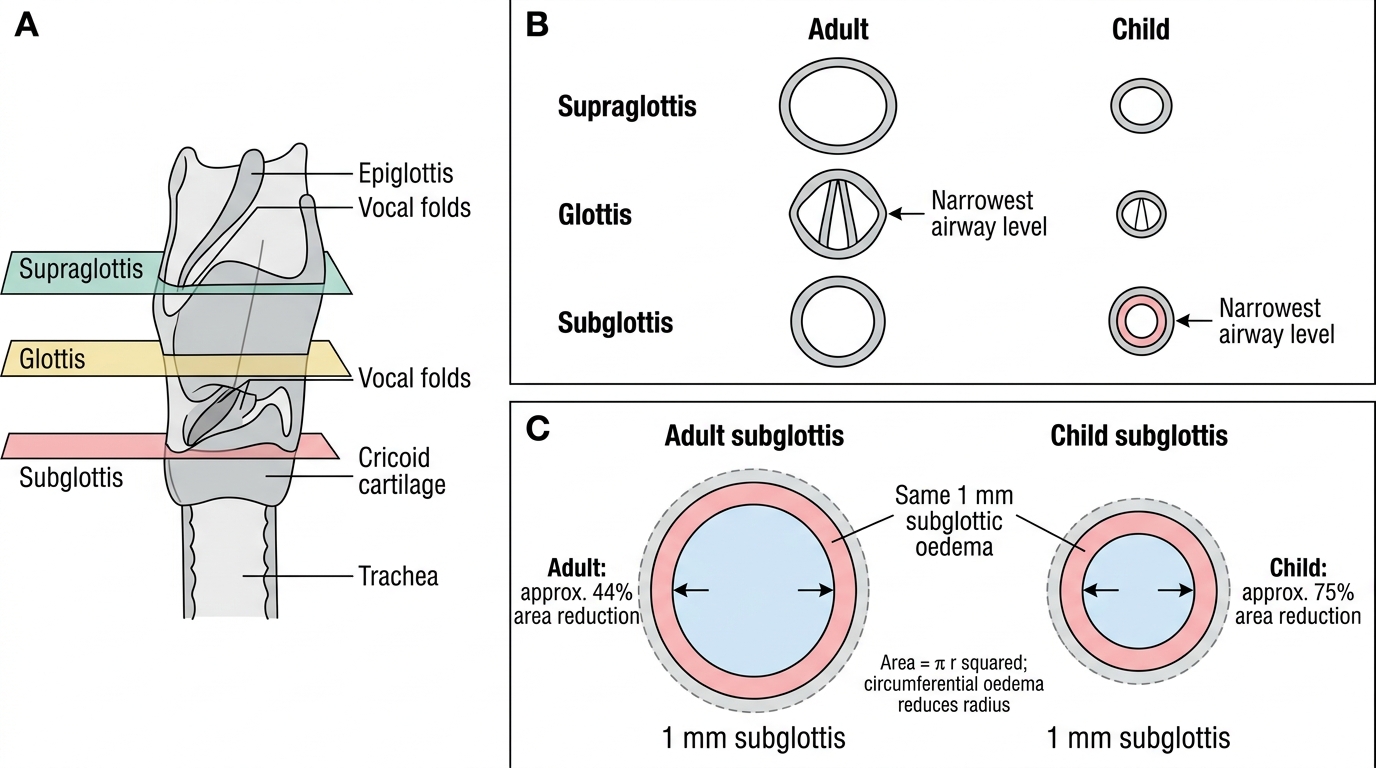
Subglottic Oedema and Airway Narrowing in Adult vs Child
The Bernoulli effect is additionally relevant in laryngomalacia — the commonest cause of stridor in infants. During inspiration, the infant generates negative intraluminal pressure to draw air into the lungs. If the supraglottic structures are floppy (an omega-shaped epiglottis that curls posteriorly, shortened aryepiglottic folds, and bulky redundant arytenoid mucosa), the Bernoulli effect causes these soft tissues to be sucked into the laryngeal inlet with each inspiration, dynamically narrowing it. The stridor therefore worsens with any condition that increases inspiratory effort — crying, feeding, upper respiratory infections, agitation — and improves when the infant is calm, prone, or neck-extended (which straightens the epiglottis). This dynamic nature — worse with effort, better at rest — is the hallmark of laryngomalacia and distinguishes it from the fixed obstruction of subglottic stenosis.
In bilateral vocal cord palsy, the mechanism is different: the posterior cricoarytenoid muscles are paralysed, and the cords lie adducted in the paramedian position due to the unopposed passive resting tone of the ligaments and the cricothyroid muscle (innervated by the superior laryngeal nerve, which is spared). Each breath must pass through this narrow fixed midline gap, generating biphasic stridor. The voice is paradoxically preserved (the adducted cords still vibrate) while the airway is compromised — an important clinical distinguishing feature.
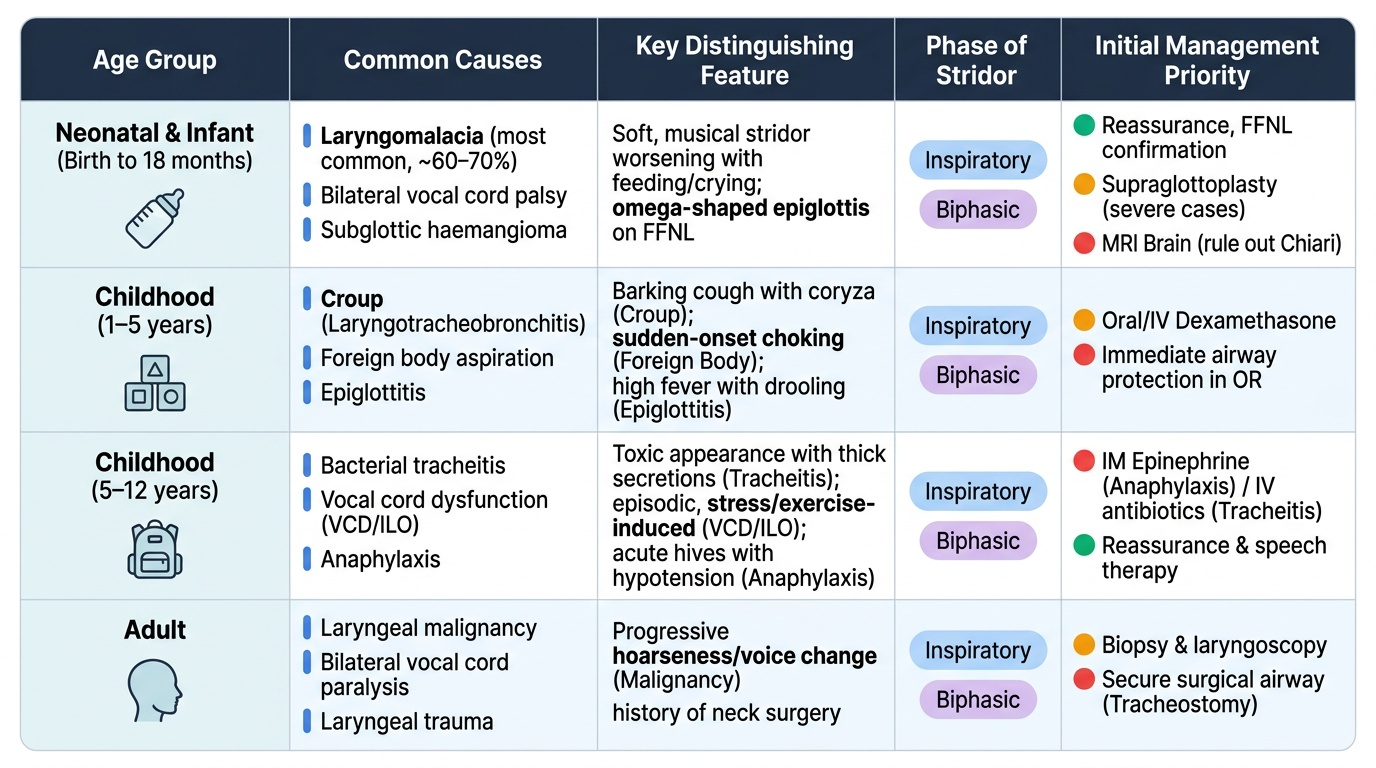
Causes of Stridor by Age Group
Organising the causes of stridor by age group converts an overwhelming list into a clinically navigable differential. Within each age group, one or two causes dominate and the others are distinguishable by key clinical features.
Provided image
Neonatal and infant stridor (birth to 18 months):
Laryngomalacia accounts for approximately 60-70% of all neonatal and infant stridor. The stridor is inspiratory, soft, and musical; it appears within the first few weeks of life and characteristically worsens with feeding, crying, and upper respiratory infections. The infant is typically otherwise well and thriving. The diagnosis is confirmed by flexible nasolaryngoscopy (FFNL), which shows the characteristic omega-shaped epiglottis curling posteriorly into the airway and/or the shortened aryepiglottic folds drawing the arytenoids inward on inspiration. More than 90% of cases resolve spontaneously by 18-24 months as the laryngeal cartilages stiffen with growth. Surgical treatment (supraglottoplasty — division of the short aryepiglottic folds and trimming of the redundant arytenoid mucosa) is reserved for the minority with failure to thrive, aspiration, or obstructive sleep apnoea.
Bilateral vocal cord palsy in neonates produces biphasic stridor from birth; it may be idiopathic (the commonest type in neonates, often resolves spontaneously), associated with birth trauma, or a feature of Arnold-Chiari malformation (hindbrain herniation compressing the vagal nuclei — consider MRI brain in any neonate with unexplained bilateral VCP).
Subglottic haemangioma presents between 6 weeks and 6 months of age as progressive biphasic stridor. It is a vascular tumour of the subglottic region that grows during the 'proliferative phase' of infantile haemangiomas (0-12 months) and then involutes. It is associated with facial cutaneous haemangiomas in 50% of cases. Diagnosis: microlaryngoscopy and bronchoscopy. Treatment: propranolol (oral, the drug of choice for infantile haemangiomas); CO2 laser in refractory cases.
Laryngeal web and subglottic stenosis (congenital) are rare structural anomalies causing stridor from birth; they require surgical correction.
Childhood stridor (1-12 years):
Croup (acute laryngotracheobronchitis) — parainfluenza virus, subglottic narrowing, barking cough, steeple sign on AP X-ray — is the commonest cause of childhood stridor (covered in EN4.41).
Acute epiglottitis — Haemophilus influenzae b, supraglottic cellulitis, drooling, thumb sign on lateral X-ray, DO NOT examine throat — is covered in EN4.41.
Foreign body aspiration presents with sudden onset choking, coughing, and stridor, followed by a 'quiet interval' (the foreign body lodges and the acute response settles). A radiopaque foreign body is seen on X-ray; a radiolucent foreign body may cause air trapping (hyperinflation on the affected side on expiratory X-ray). Urgent rigid bronchoscopy for retrieval.
Diphtheria — grey pseudomembrane, unvaccinated child — covered in EN4.41.
Adult stridor:
Bilateral vocal cord palsy — most commonly post-thyroidectomy (bilateral RLN injury); also bilateral thyroid malignancy, neck irradiation, neurological disorders. The voice is preserved but the airway is compromised; stridor is biphasic.
Post-intubation subglottic stenosis — fibrosis at the cricoid level following prolonged or traumatic endotracheal intubation; presents with progressive exertional dyspnoea months after extubation, then stridor at rest. Graded by Cotton-Myer classification (Grade I: <50% obstruction; Grade II: 51-70%; Grade III: 71-99%; Grade IV: complete). Managed by endoscopic dilatation (balloon or rigid) for early-grade stenosis; laryngotracheal reconstruction (open surgery) for severe stenosis.
Laryngeal carcinoma — progressive hoarseness preceding stridor; cord fixation on laryngoscopy; CT staging required.
SELF-CHECK
A 6-week-old infant is brought to the clinic because of a high-pitched squeaky noise during feeding that has been present since 3 weeks of age. The infant is thriving on breastfeeding (weight at the 50th percentile) and has no episodes of choking, apnoea, or cyanosis. Between feeds, the infant is quiet and comfortable. Flexible nasolaryngoscopy shows an omega-shaped epiglottis that folds posteriorly during inspiration. The most appropriate management is:
A. Urgent microlaryngoscopy and bronchoscopy under general anaesthesia
B. Parental reassurance and explanation; follow-up in 3 months; reassess if feeding deteriorates or weight falters
C. Tracheostomy to secure the airway
D. Commence oral propranolol immediately for presumed subglottic haemangioma
Reveal Answer
Answer: B. Parental reassurance and explanation; follow-up in 3 months; reassess if feeding deteriorates or weight falters
The clinical features — inspiratory stridor beginning at 3 weeks of life, worsening with feeding, an omega-shaped epiglottis on FFNL, and a thriving infant without apnoea or cyanosis — are diagnostic of laryngomalacia, the commonest cause of infant stridor. In a thriving infant without failure to thrive, aspiration pneumonia, obstructive apnoea, or cor pulmonale, management is conservative: parental reassurance, explanation of the condition and its expected natural history (resolution by 18-24 months in >90%), prone-positioning advice, and follow-up. Urgent MLB/DLB and tracheostomy are not indicated for mild laryngomalacia. Propranolol is the treatment for subglottic haemangioma, not laryngomalacia — haemangioma would present later (6 weeks-6 months) with progressive biphasic stridor and often with a cutaneous facial haemangioma.