Page 5 of 29
EN4.22 | Deviated Nasal Septum — SDL Guide (Part 2)
Diagnosis and Differential Diagnosis of DNS
The diagnosis of DNS is largely clinical: a history of unilateral nasal obstruction (constant, not seasonal or episodic) combined with a visible septal deviation on anterior rhinoscopy is sufficient in most cases. However, confirming that the DNS is the genuine cause of the patient's symptoms — rather than an incidental finding in a patient whose actual problem is something else — requires clinical judgement. Many patients with DNS also have co-existing allergic rhinitis, and the rhinitis may be the dominant driver of their obstruction; operating on the DNS without addressing the rhinitis will give a poor outcome. This principle — that a positive finding does not automatically mean a relevant finding — is one of the most important lessons in ENT clinical reasoning and extends beyond DNS to any structural abnormality discovered during workup for a symptom.
The differential diagnosis of unilateral nasal obstruction includes other structural causes that may coexist with or mimic DNS. The key differentiators are:
- Antrochoanal polyp: single, translucent, pale grey mass in the posterior nasal cavity; not the nasal septum itself; visible on endoscopy; CT shows origin in the maxillary sinus.
- Nasal foreign body: in children; foul-smelling unilateral purulent discharge; may be visible anteriorly.
- Nasal tumour (JNA, malignancy): unilateral mass; vascularity (JNA bleeds profusely when touched); in JNA do NOT biopsy; in adults over 40 with bloody discharge, contrast CT mandatory.
- Septal abscess or haematoma: acute presentation after nasal trauma; septal swelling is fluctuant, bilateral (elevates both mucosal flaps), acutely tender — very different from the firm fixed bony/cartilaginous deviation of DNS.
Septal headache vs sinusitis headache: both can present as facial/periorbital pain. Distinguishing features — sinusitis headache is accompanied by purulent nasal discharge, hyposmia, fever, and thickening on CT PNS; septal contact headache is reproduced by probing the spur, relieved by topical anaesthetic, with no CT sinus changes.
SELF-CHECK
A 19-year-old woman presents for evaluation of DNS and recurrent right-sided headaches. She is very keen on surgery. On examination, she has a mild C-shaped deviation of the nasal septum to the right, but her nasal passages are reasonably patent bilaterally. Her headaches are throbbing, associated with nausea and photophobia, and last 12–24 hours. What is the most appropriate next step?
A. Refer for septoplasty — the DNS is the likely cause of her migrainous headaches
B. Manage the headaches as migraine; the DNS is mild and likely incidental
C. Order CT PNS to assess for sinusitis before considering septoplasty
D. Perform submucous resection of the deviated segment under local anaesthesia
Reveal Answer
Answer: B. Manage the headaches as migraine; the DNS is mild and likely incidental
The headache described — throbbing, associated with nausea and photophobia, lasting 12–24 hours — has the classic features of migraine, not septal contact headache (which is dull, non-pulsatile, not associated with nausea, and reproducible by probing the spur). The DNS here is mild and the nasal passages are reasonably patent — there is no clinical indication for septoplasty. Operating on an incidental mild DNS to 'cure' what is actually migraine will not help the patient and exposes her to surgical risk unnecessarily. Septal contact headache is dull, unilateral, reproduced by probing the spur, and relieved by topical nasal anaesthetic — it does not have migrainous features.
Management: Septoplasty and Adjunctive Procedures
The management of symptomatic DNS is primarily surgical — no medical treatment corrects an anatomical deviation. The decision to operate depends on the severity of symptoms, the degree of deviation, the patient's age, and the absence of contraindications. Patients with mild DNS and co-existing rhinitis should have the rhinitis treated medically first, as the rhinitis may be the dominant symptom driver and successful medical treatment may make surgery unnecessary. The surgical approach — septoplasty — is one of the most commonly performed ENT procedures in the world, and understanding its indications, steps, and complications is a core expectation at the KH level. The goal of septoplasty is functional: to restore a symmetrical, patent nasal airway, not to achieve a cosmetically straight septum visible only on CT. A patient who has a straight septum post-operatively but is still obstructed because of unaddressed turbinate hypertrophy has not had a successful outcome.
Provided image
Indications for septoplasty:
- Significant nasal obstruction due to DNS refractory to a trial of intranasal corticosteroids and nasal decongestants.
- Recurrent or chronic sinusitis where DNS obstructs the OMC (combined septoplasty + FESS).
- Epistaxis from a septal spur not controlled by local measures.
- Septal spur headache (Sluder's neuralgia) confirmed by spur contact examination and topical lignocaine test.
- Obstructive sleep apnea contributed to by DNS.
- As part of rhinoplasty for cosmetic and functional nasal deformity.
Age restriction: Septoplasty should be deferred until the nasal septum has completed its growth — generally ≥16 years in females and ≥17–18 years in males. Operating on the septal cartilage before skeletal maturity risks disrupting the septal growth centre (the junction of the quadrilateral cartilage with the nasal bones), which can cause nasal growth arrest and secondary saddle-nose deformity in adolescents.
Septoplasty procedure (key steps per Dhingra):
1. Killian's incision: a vertical incision on the concave side of the deviation, placed just inside the vestibule at the mucocutaneous junction. This is the standard access incision.
2. Mucoperiosteal/mucoperichondrial flap elevation: the incision is deepened through the mucosa to expose the cartilage; a plane is developed between the mucosa/perichondrium and the underlying cartilage — the subperichondrial plane. The mucosal flap is elevated widely on one side (and if needed on both sides) to expose the full extent of the deviation without tearing the mucosa.
3. Resection or repositioning of the deviated segment: the deviated cartilage or bone is excised or repositioned. The cartilage is scored, morselised, or partially excised while preserving at least 1 cm of dorsal and caudal cartilage strut (the 'L-strut') to prevent loss of nasal support. Bony deviations (perpendicular plate, vomer, spurs) are removed with chisel and mallet or through-cutting forceps.
4. Closure: the mucosal flaps are repositioned and sutured or held with through-and-through septal sutures; a splint or pack may be placed for 48 hours.
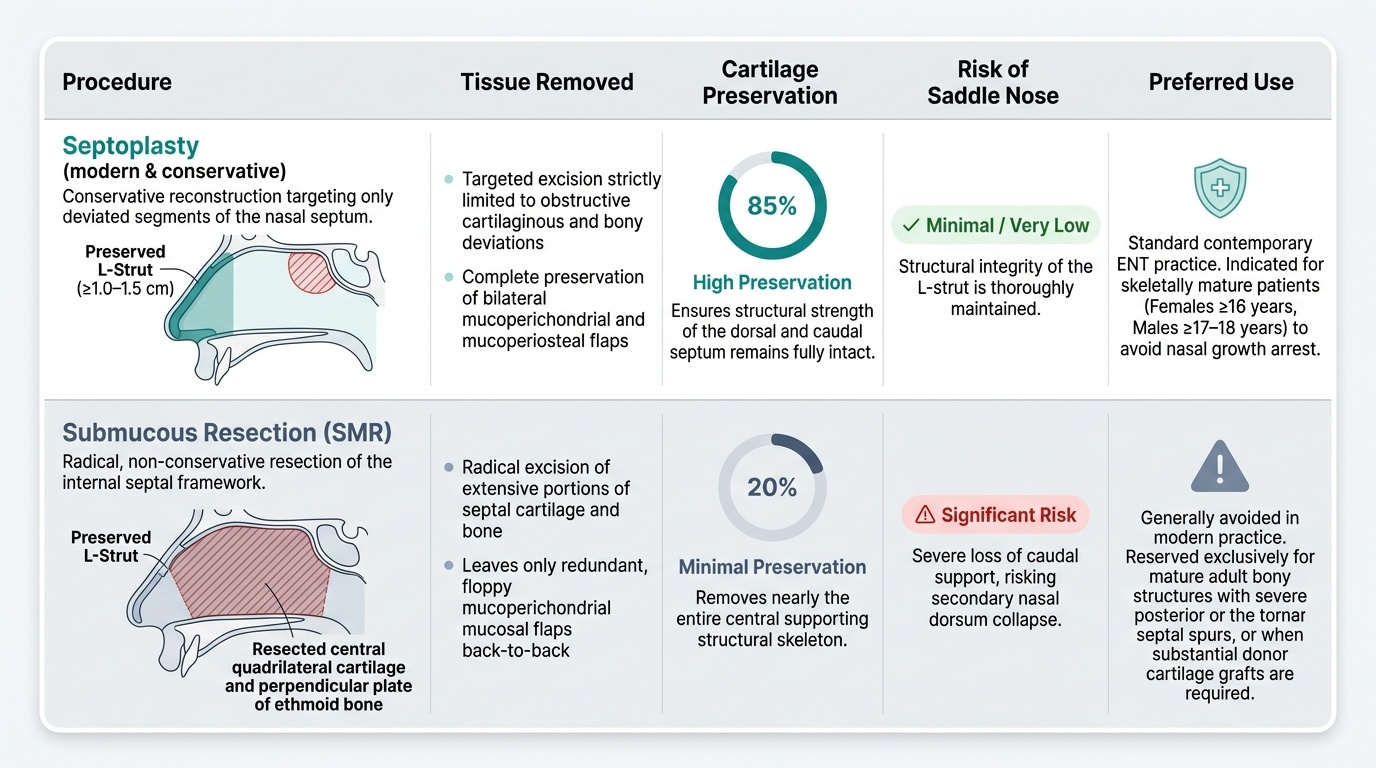
Septoplasty vs submucous resection (SMR):
SMR (Killian's procedure) is an older technique that removes the central portion of the quadrilateral cartilage. It is more extensive, leaving only a dorsal and caudal cartilage rim. The risk of saddle-nose deformity (loss of nasal bridge height from loss of dorsal cartilage support) is higher with SMR than with modern septoplasty. Septoplasty is now the preferred procedure because it is cartilage-conserving.
Turbinate reduction: Compensatory inferior turbinate hypertrophy on the contralateral side is frequently addressed during the same surgical session by inferior turbinoplasty or submucosal diathermy of the turbinate. Leaving a markedly hypertrophied compensatory turbinate unaddressed can result in persistent bilateral obstruction despite a technically correct septoplasty.
Complications of septoplasty: haematoma (most important early complication — prevented by quilting sutures and a tight pack), septal perforation (mucosal tear on both sides at the same level), saddle-nose deformity (if L-strut is inadequately preserved), infection, cerebrospinal fluid leak (rare — if cribriform plate is damaged during posterior bony work).
CLINICAL PEARL
The most important anatomical concept in septoplasty is preservation of the L-strut — the 1 cm-wide strip of cartilage at the dorsal and caudal margin of the quadrilateral cartilage. The dorsal strut provides the height of the nasal bridge; the caudal strut supports the nasal tip. If either strut is removed or weakened, the nose collapses — the dorsal strut loss causes a saddle-nose deformity (flattening of the nasal bridge, the hallmark complication of over-aggressive SMR), and caudal strut loss causes tip ptosis. Every septoplasty decision — how much cartilage to excise versus score versus morselise — is made with one eye on preserving the L-strut.
Self-Assessment and Consolidation
Test your understanding with the scenario below before attempting the quiz:
A 17-year-old boy is referred for a 2-year history of progressive left-sided nasal obstruction after a sports injury to his nose at age 15. Anterior rhinoscopy reveals the caudal end of the nasal septum dislocated to the left out of the maxillary crest groove, with the anterior free edge of the septum visible in the left vestibule. There is also a bony spur at the septal floor contacting the left inferior turbinate.
Consider: (a) Is he old enough for septoplasty? (b) What is the specific anatomical type of deviation? (c) What operation would you plan, and would turbinate surgery be included? (d) What is the most important intraoperative complication to prevent, and how?
SELF-CHECK
After septoplasty, a patient develops a circular perforation in the middle of the nasal septum. The most likely cause is:
A. Infection of the maxillary sinus communicating with the septum
B. Mucosal tears on both sides of the septum at the same level, with loss of the intervening cartilage
C. Excessive preservation of the L-strut leading to cartilage necrosis
D. Injury to the perpendicular plate of the ethmoid causing cribriform plate damage
Reveal Answer
Answer: B. Mucosal tears on both sides of the septum at the same level, with loss of the intervening cartilage
Septal perforation after septoplasty occurs when mucosal tears (flap tears) occur on both sides of the septum at exactly the same level during flap elevation. The devascularised segment of cartilage between the two opposing mucosal tears has no blood supply and undergoes necrosis, leaving a permanent hole. Prevention is by careful flap elevation in the subperichondrial plane, avoiding direct cartilage handling until the flap is elevated, and if tears do occur on one side, ensuring the contralateral side is intact at that level. Bilateral opposing tears at the same level are the critical danger configuration.