Page 20 of 29
EN4.28 | Epistaxis — SDL Guide (Part 2)
Causes of Epistaxis
The causes of epistaxis are broadly classified as local (within the nose) and systemic (general factors predisposing to bleeding). Most clinical epistaxis has a local trigger acting on a systemic background — for example, digital trauma (local) in a child on aspirin for Kawasaki disease (systemic), or a septal spur (local) in an elderly hypertensive on warfarin (systemic). Both dimensions must be assessed. A systematic approach to aetiology prevents common errors such as treating a single episode of epistaxis as idiopathic without checking the blood pressure or medications, or missing hereditary haemorrhagic telangiectasia in a patient with recurrent epistaxis and a positive family history. The most important red-flag cause to exclude in a young male with recurrent epistaxis and nasal obstruction is juvenile nasopharyngeal angiofibroma (JNA) — a vascular tumour that must never be biopsied; always image with contrast CT first.
Provided image
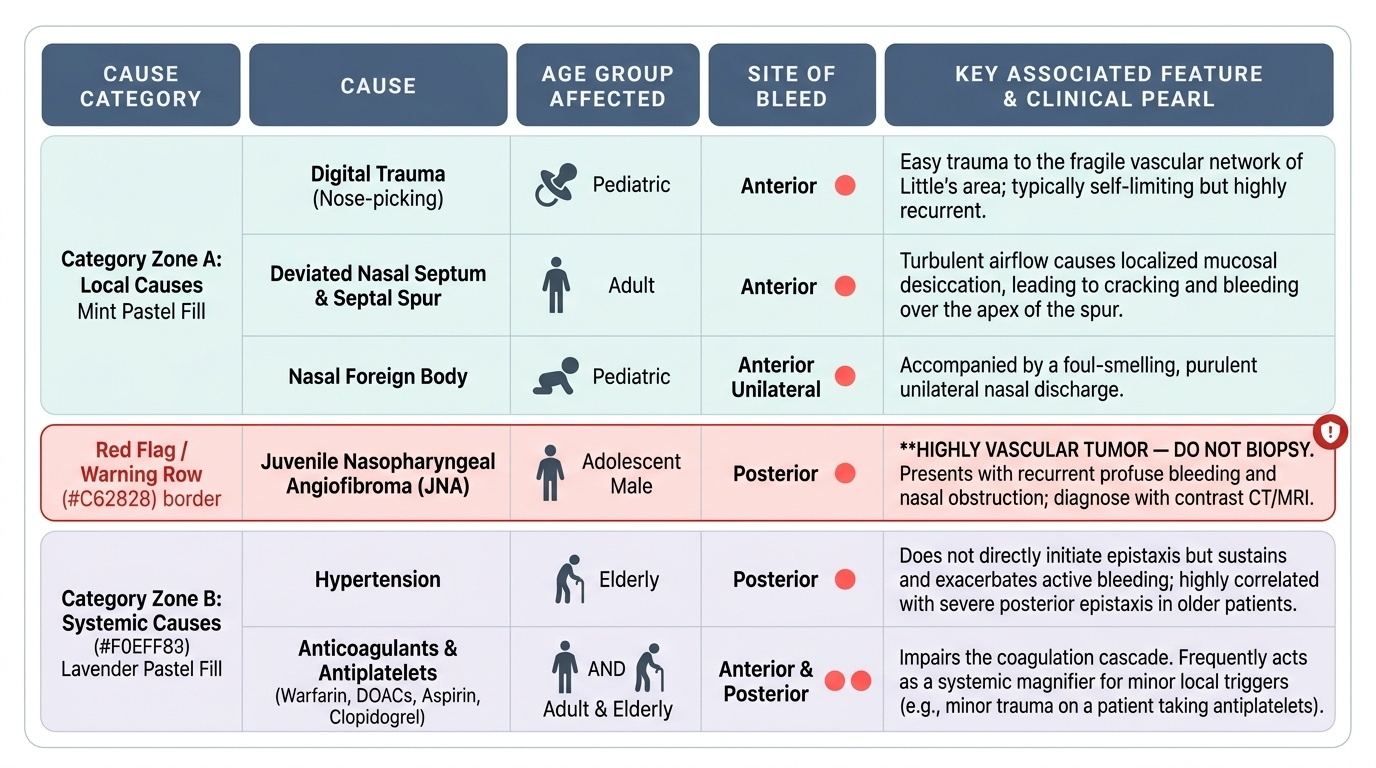
Local causes:
- Digital trauma (nose-picking): commonest cause in children; the vascular Little's area is easily traumatised by fingers.
- Nasal infections: acute rhinitis (inflamed, friable mucosa), chronic rhinosinusitis.
- Deviated nasal septum and septal spur: turbulent airflow and mucosal desiccation over the spur causes cracking and bleeding.
- Nasal foreign body: unilateral epistaxis + foul discharge in a child.
- Nasal polyps: occasionally bleed if traumatised.
- Trauma: nasal fracture, facial trauma.
- Tumours: Juvenile nasopharyngeal angiofibroma (JNA) — adolescent males, recurrent profuse epistaxis + nasal obstruction; DO NOT BIOPSY — diagnose on contrast CT/MRI. Nasopharyngeal carcinoma; maxillary sinus tumours. Any tumour in the nasal cavity or nasopharynx can present with epistaxis.
- Nasal surgery: post-septoplasty, post-adenoidectomy (primary or reactionary haemorrhage).
- Septal perforation: midline perforation; turbulent air flow over the perforation edge causes crusting and recurrent bleeding at the perforation rim.
- Dry climate and low humidity: mucosal desiccation — very common in winter and at high altitude.
Systemic causes:
- Hypertension: does not directly cause epistaxis but sustains a bleed once started; associated strongly with posterior epistaxis in the elderly.
- Anticoagulants and antiplatelet drugs: warfarin, DOACs, aspirin, clopidogrel — all reduce the ability to clot; common in the elderly population with atrial fibrillation, coronary artery disease.
- Coagulopathies: haemophilia A (factor VIII deficiency), haemophilia B (factor IX deficiency), von Willebrand disease.
- Thrombocytopaenia: immune thrombocytopaenic purpura (ITP), haematological malignancy, dengue fever (very common in India).
- Liver disease: reduced synthesis of clotting factors (II, VII, IX, X) + reduced thrombopoietin → low platelets.
- Hereditary haemorrhagic telangiectasia (HHT/Osler-Weber-Rendu disease): autosomal dominant; recurrent bilateral epistaxis from telangiectasias in the nasal mucosa; associated telangiectasias on the lips, tongue, fingertips, and gastrointestinal tract; pulmonary arteriovenous malformations.
- Infections: dengue haemorrhagic fever (thrombocytopaenia), leptospirosis, typhoid.
- Pregnancy: increased mucosal vascularity and hormonal changes.
SELF-CHECK
A 68-year-old woman on warfarin for atrial fibrillation presents with bilateral nosebleeds running down her throat, not stopped by self-applied anterior pressure for 30 minutes. Her INR is 4.8. Blood pressure is 190/105 mmHg. The bleeding is most likely arising from:
A. Little's area bilaterally — anterior epistaxis from anticoagulation
B. The sphenopalatine artery territory — posterior epistaxis in an elderly hypertensive on anticoagulation
C. Both ethmoidal arteries — requires internal carotid ligation
D. Woodruff's plexus anteriorly — controlled by anterior nasal packing
Reveal Answer
Answer: B. The sphenopalatine artery territory — posterior epistaxis in an elderly hypertensive on anticoagulation
The clinical picture — elderly, hypertensive, on anticoagulation (warfarin with supratherapeutic INR 4.8), bilateral bleeding running down the throat, not controlled by anterior pressure — is classic posterior epistaxis from the sphenopalatine artery territory. Posterior epistaxis in the elderly is strongly associated with hypertension (sustains the bleed by maintaining high arterial pressure) and anticoagulation (impairs haemostasis). The blood running posteriorly (rather than anteriorly from the nostril) and bilateral nature are the key clinical distinguishers from anterior Little's area bleeding. Woodruff's plexus is posterior, not anterior. The management requires posterior nasal packing or balloon tamponade and reversal of anticoagulation.
Principles of Management
The management of epistaxis follows a stepwise approach from simple first aid to advanced surgical intervention, escalating based on the site (anterior vs posterior), severity, and whether lower-level measures have controlled the bleed. Every step in the escalation ladder must be mastered, as the correct approach can save a life in a posterior bleed or prevent unnecessary hospitalisation in an anterior bleed. The key principle is that management of the bleed and management of the underlying cause are not sequential — they run in parallel. A hypertensive patient with posterior epistaxis needs simultaneous nasal packing AND antihypertensive therapy; an anticoagulated patient needs simultaneous haemostasis AND anticoagulation reversal. Treating only the nasal bleed without addressing a BP of 200/115 is incomplete management and the bleed will likely recur within hours.
Step 1 — First aid for anterior epistaxis (Trotter's method):
1. Sit the patient upright, leaning slightly forward (prevents blood running into the throat and airway).
2. Pinch the soft part of the nose (the cartilaginous portion, just below the nasal bones) firmly with the thumb and index finger.
3. Breathe through the mouth.
4. Maintain continuous pressure for 10–15 minutes without releasing.
5. Apply a cold compress to the forehead or nasal bridge.
6. Do NOT tilt the head back — this causes blood to run down the throat, may cause aspiration, and is a common incorrect first-aid manoeuvre.
7. If bleeding stops: do NOT blow the nose for 24 hours; avoid nose-picking; apply vaseline to the Little's area to prevent mucosal desiccation.
Step 2 — Identification and cauterisation of the bleeding point:
If Trotter's method controls the bleed and the patient is seen in ENT, the bleeding point in Little's area is identified on anterior rhinoscopy. Cauterisation is performed:
- Chemical cauterisation: application of a silver nitrate stick (75% silver nitrate) or trichloroacetic acid to the bleeding point; painless, outpatient procedure; effective for small, well-visualised anterior bleeds.
- Electrocauterisation: bipolar diathermy under direct vision; more controlled than silver nitrate; preferred for larger vessels.
- Important rule: NEVER cauterise both sides of the septum at the same level simultaneously — bilateral opposing cauterisation at the same site devascularises the intervening cartilage and can cause septal perforation.
Step 3 — Anterior nasal packing:
If cauterisation fails or the bleeding point cannot be identified, anterior nasal packing is applied:
- Bismuth iodoform paraffin paste (BIPP) ribbon gauze: classical pack; layered into the nasal cavity from below; left in place 24–48 hours.
- Non-adherent nasal packs (Merocel, RhinoRocket): expandable compressed sponge packs that expand on contact with blood/saline; easy to insert; preferred in most settings.
- After packing, the patient is admitted, given antibiotics (to prevent toxic shock syndrome and sinusitis), and the pack is removed at 24–48 hours.
Step 4 — Posterior nasal packing:
For confirmed posterior epistaxis not controlled by anterior packing:
- Brighton balloon / Foley catheter: a balloon catheter is inserted through the nasal cavity into the nasopharynx and inflated to tamponade the posterior nasal space; an anterior pack is added to provide bidirectional pressure.
- Bilateral posterior packing with gauze: classical method (Bellocq's method); technically demanding; superseded by balloon devices.
- Patients with posterior packs must be admitted to a monitored setting (risk of hypoxia, vasovagal syncope, airway compromise).
Step 5 — Surgical / interventional radiology:
For refractory bleeding not controlled by packing:
- Endoscopic sphenopalatine artery ligation (ESPAL): the sphenopalatine artery is identified endoscopically at the sphenopalatine foramen (posterior middle meatus) and clipped or cauterised; the gold standard surgical approach for posterior epistaxis.
- Anterior and posterior ethmoidal artery ligation: for anterior bleeds from the ethmoidal artery territory; performed through an external Lynch-Howarth incision at the medial canthus.
- Arterial embolisation (interventional radiology): selective catheterisation of the internal maxillary artery and embolisation of the sphenopalatine artery; preferred over open ligation in some centres, especially in high-risk surgical patients.
- External carotid artery ligation: historical; rarely performed now; less targeted than ESPAL.
Adjunctive measures:
- Blood pressure control: urgent antihypertensive therapy (IV labetalol, oral amlodipine) in hypertensive patients — reducing blood pressure reduces the driving pressure sustaining the bleed.
- Reversal of anticoagulation: warfarin — vitamin K (IV) ± fresh frozen plasma or prothrombin complex concentrate (PCC) for life-threatening bleed; DOACs — specific reversal agents (idarucizumab for dabigatran, andexanet alfa for factor Xa inhibitors) or PCC.
- Tranexamic acid (TXA): topical or systemic; antifibrinolytic — useful adjunct for mucosal bleeds.
- Blood transfusion: for haemodynamically significant haemorrhage.
CLINICAL PEARL
The most important first-aid instruction that is routinely given incorrectly is: 'tilt your head back' — this is wrong and dangerous. Tilting the head back directs blood posteriorly into the pharynx and trachea, causing nausea, vomiting of blood, airway soiling, and aspiration. The correct instruction is: sit upright, lean slightly forward, pinch the soft cartilaginous nose firmly for 10–15 minutes without releasing. This position allows the blood to drain forward into a tissue or bowl where it can be assessed for volume, rather than entering the gastrointestinal tract. Every medical student and doctor must actively correct this misconception whenever they encounter it — in patients, family members, and healthcare workers.
Self-Assessment
Apply the full clinical framework from this module to the following scenarios before the quiz:
Scenario A: A 9-year-old boy has a nosebleed from his right nostril that started 10 minutes ago. Blood is dripping forward. His mother is holding his head back. He is otherwise well, no medications, no family history of bleeding.
Scenario B: A 75-year-old man on warfarin and aspirin presents with bilateral bleeding running down his throat for 1 hour. BP 200/115. No visible anterior bleeding point.
For Scenario A: What is the first-aid correction you must make immediately? What is the likely bleeding site and cause? What is the next management step if first aid fails?
For Scenario B: Classify the bleed. What investigations are urgent? List management steps in order, including how to address the anticoagulation.
SELF-CHECK
During chemical cauterisation of Little's area for recurrent anterior epistaxis, the surgeon applies a silver nitrate stick to a bleeding point on the right anteroinferior nasal septum, then immediately cauterises the same level on the left side to prevent future bleeding. The most serious complication of this action is:
A. Toxic shock syndrome from bilateral silver nitrate application
B. Septal perforation due to bilateral opposing cauterisation devascularising the septal cartilage
C. Rhinitis medicamentosa from mucosal chemical irritation
D. Post-nasal drip from disruption of both mucosal surfaces simultaneously
Reveal Answer
Answer: B. Septal perforation due to bilateral opposing cauterisation devascularising the septal cartilage
Bilateral opposing septal cauterisation at the same level is a well-known cause of septal perforation. The septal cartilage is avascular and relies entirely on its perichondrial blood supply from the overlying mucosa. When both mucosal surfaces at the same septal level are cauterised simultaneously, the underlying cartilage is devascularised from both sides and undergoes avascular necrosis, leading to perforation. The rule is absolute: never cauterise both sides of the septum at the same level at the same sitting. If bilateral cauterisation is needed, it must be staged over several weeks to allow one side to heal before treating the other.