Page 22 of 29
EN4.29 | Obstructive Sleep Apnea — SDL Guide
Learning Objectives
- Describe the clinical features of obstructive sleep apnea including snoring, witnessed apnoeas, excessive daytime somnolence, and morning headaches
- Describe the pathophysiology of upper airway collapse in OSA and the risk factors for it
- Choose appropriate investigations including polysomnography and pulse oximetry, and describe the apnoea-hypopnoea index (AHI)
- Describe the principles of management including weight loss, positional therapy, CPAP, mandibular advancement devices, and surgical options
- Identify the systemic complications of untreated OSA — hypertension, cardiovascular disease, metabolic syndrome
INSTRUCTIONS
Obstructive sleep apnea (OSA) is among the most common and underdiagnosed chronic conditions in adults, affecting 3–7% of men and 2–5% of women globally. It carries major systemic consequences if untreated. EN4.29 requires you to describe clinical features, choose investigations, and describe principles of management. This module also covers OSA in children — where adenotonsillar hypertrophy is the dominant cause — and the overlap with rhinitis and nasal obstruction encountered throughout this cluster.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery. 8th ed. Chapter on Sleep-Disordered Breathing and Obstructive Sleep Apnea (textbook)
- Hazarika P, Nayak DR, Balakrishnan R. Textbook of Ear, Nose and Throat — Head and Neck Surgery. Chapter on Snoring and OSA (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery. 8th ed. Vol 2: Sleep-Disordered Breathing (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 48-year-old male bus driver with a BMI of 34 kg/m² is brought to the ENT OPD by his wife, who is 'at her wits' end' because of his snoring. She reports he stops breathing for 20–30 seconds at a time, multiple times each night, and then gasps and restarts. He is unaware of these episodes. He wakes unrefreshed, has a headache every morning, and has fallen asleep at traffic lights on two occasions. His blood pressure is 158/96 mmHg despite being on two antihypertensive agents. His Epworth Sleepiness Scale score is 17/24. His general practitioner said 'it's just snoring.' Is the GP right? What systemic condition makes his untreated OSA potentially dangerous? And what is the most important investigation to order?
WHY THIS MATTERS
Obstructive sleep apnea is a chronic medical condition of major public health importance in India. It is grossly underdiagnosed because many patients normalise snoring and daytime sleepiness as features of ageing or a busy lifestyle. Yet untreated OSA carries a 2–3 times increased risk of hypertension, coronary artery disease, stroke, atrial fibrillation, metabolic syndrome, and type 2 diabetes. It is also a major cause of road traffic accidents — excessive daytime somnolence from fragmented sleep impairs driving performance as much as alcohol intoxication. OSA in a bus driver, lorry driver, or aviation professional has serious public safety implications. As a final-year MBBS student, you will encounter OSA in medicine, cardiology, endocrinology, and ENT — knowing to ask about snoring, witnessed apnoeas, and daytime sleepiness is the first step toward preventing serious systemic disease.
RECALL
Recall the anatomy of the upper airway from your anatomy sessions. The pharynx is divided into the nasopharynx (above the soft palate), the oropharynx (between the soft palate and the tip of the epiglottis), and the hypopharynx (below the epiglottis to the larynx). The oropharyngeal segment is the most collapsible — it lacks rigid bony or cartilaginous support and relies on active muscle tone from the pharyngeal dilator muscles (primarily genioglossus, tensor palatini, and palatoglossus) to remain patent during sleep. The genioglossus (the main tongue protruder muscle, innervated by the hypoglossal nerve, CN XII) is the most important pharyngeal dilator — its tone normally increases reflexively with any rise in upper airway resistance during sleep, pulling the tongue base forward and preventing collapse. In OSA, this reflex is insufficient or overwhelmed, and the airway collapses repeatedly during sleep.
Clinical Features of Obstructive Sleep Apnea
The clinical presentation of OSA spans both nocturnal (night-time) and diurnal (daytime) symptoms reflecting the two physiological consequences of repeated upper airway obstruction during sleep: arousal from sleep (fragmenting sleep architecture) and episodic hypoxaemia (intermittent oxygen desaturation during each apnoeic event). The combination of these two mechanisms produces the characteristic symptom cluster that must be actively sought in the history. The cardinal insight about OSA symptomatology is that most patients are completely unaware of the apnoeic episodes — the witnesses are the bed-partner and the morning symptoms. This means the patient's chief complaint may be 'I'm tired all the time' or 'I can't concentrate at work' rather than 'I stop breathing in my sleep' — and the doctor who does not think to ask about snoring and witnessed apnoeas will miss the diagnosis entirely. A targeted sleep history, including asking the partner, is the only way to reliably elicit the diagnosis at the bedside.
Nocturnal symptoms:
- Snoring: the cardinal symptom; loud, habitual, and often reported by the bed-partner before the patient is aware of it. Not all snorers have OSA, but virtually all patients with significant OSA snore.
- Witnessed apnoeas: episodes of cessation of breathing during sleep observed by the bed-partner, typically lasting 20–30 seconds, ending with a loud gasp or snort as the patient partially arouses. This is the most specific symptom of OSA.
- Gasping or choking episodes: the patient partially wakes choking or gasping for breath, often unaware of the apnoeic episode.
- Restless sleep and frequent arousal: multiple partial arousals per hour fragment sleep architecture; the patient moves frequently, may fall out of bed.
- Nocturia: frequent waking at night may be misinterpreted as urinary urgency — in fact, the arousal triggers voiding, not a urinary problem.
- Nocturnal sweating and reflux/heartburn (raised intrathoracic negative pressure during obstructed breathing episodes can provoke reflux).
Diurnal (daytime) symptoms:
- Excessive daytime somnolence (EDS): the most clinically significant daytime symptom; the patient falls asleep in passive situations (reading, watching TV), active situations (driving, conversations, meetings), or even during meals. Assessed by the Epworth Sleepiness Scale (ESS) — a score ≥10 indicates clinically significant EDS.
- Unrefreshing sleep: the patient wakes feeling as tired as when they went to bed, despite sleeping for 7–8 hours.
- Morning headache: from nocturnal CO2 retention (hypercapnia) from repeated apnoeic hypoventilation; typically bifrontal, resolves within an hour of waking.
- Cognitive impairment: poor concentration, memory lapses, and reduced work performance — often the feature that first prompts medical consultation in high-functioning patients.
- Mood changes: irritability, depression — from chronic sleep deprivation.
- Erectile dysfunction in men — from autonomic dysfunction and hypoxaemia.
Risk factors for OSA:
- Male sex (2–3× higher prevalence than women, though post-menopausal risk approaches male risk).
- Obesity — BMI >30 kg/m² is the single most important modifiable risk factor; adipose tissue deposition in the neck and pharyngeal walls reduces pharyngeal airway calibre.
- Neck circumference: >43 cm in men and >41 cm in women is a risk factor (fat deposition compresses the pharyngeal lumen).
- Age: peak prevalence in 40–65 years.
- Craniofacial anatomy: retrognathia, micrognathia, high-arched narrow palate, low soft palate.
- Nasal obstruction: DNS, allergic rhinitis, adenoids — nasal obstruction increases upper airway resistance and mouth breathing, both of which predispose to pharyngeal collapse.
- Alcohol and sedatives: relax pharyngeal dilator muscle tone.
- Family history: heritable craniofacial structure and airway tone.
Pathophysiology of Upper Airway Collapse
The fundamental pathophysiology of OSA is the repeated collapse of the pharyngeal airway during sleep when the normal protective mechanisms of pharyngeal dilator muscle tone are insufficient to maintain patency against the negative intraluminal pressure generated during inspiration. Understanding this mechanism explains both why certain anatomical and functional factors predispose to OSA and why specific treatments work.
During wakefulness, the pharynx is held open by active tone in the dilator muscles — principally the genioglossus (tongue protruder), the tensor palatini (stiffens the soft palate), and the other pharyngeal constrictors acting in coordinated balance. This tone compensates for any anatomical narrowing from obesity, adenotonsillar hypertrophy, or craniofacial structure. During the transition to sleep, there is a physiological reduction in skeletal muscle tone, including the pharyngeal dilators. In most people, this is compensated for and the airway remains patent. In patients with OSA, one or more of the following factors cause the compensation to fail:
- Anatomical loading (reduced airway calibre): obesity-related fat deposition in the parapharyngeal fat pads and neck narrows the resting airway lumen; a tongue that is disproportionately large relative to the mandible (retrognathia or macroglossia) encroaches posteriorly on the oropharyngeal space; a long, flaccid soft palate and large uvula collapse posteriorly; adenotonsillar hypertrophy (in children) mechanically obstructs the airway.
- Reduced pharyngeal muscle tone during sleep: alcohol, sedatives (benzodiazepines, opioids), and sleep deprivation reduce genioglossus tone; ageing and obesity are associated with reduced neuromuscular reflex responsiveness.
- Increased upper airway resistance: nasal obstruction forces mouth breathing; mouth breathing in a supine position is associated with posterior tongue displacement and palatal collapse.
- Supine position: in the supine position, gravity acts on the tongue and soft palate, displacing them posteriorly against the pharyngeal wall; OSA is typically worse or exclusively present in the supine position in milder cases.
The resulting obstructive event cycle: airway narrows → inspiratory effort produces negative intraluminal pressure → pharyngeal walls are sucked together → complete occlusion → apnoea → oxygen saturation falls (SpO2 may drop to <80% in severe OSA) → rising CO2 and hypoxia trigger arousal → genioglossus tone restored → airway reopened → resumption of breathing with a gasp → brief sleep resumption → cycle repeats. In severe OSA, this cycle repeats >30 times per hour, producing profoundly fragmented, non-restorative sleep and repeated hypoxic episodes.
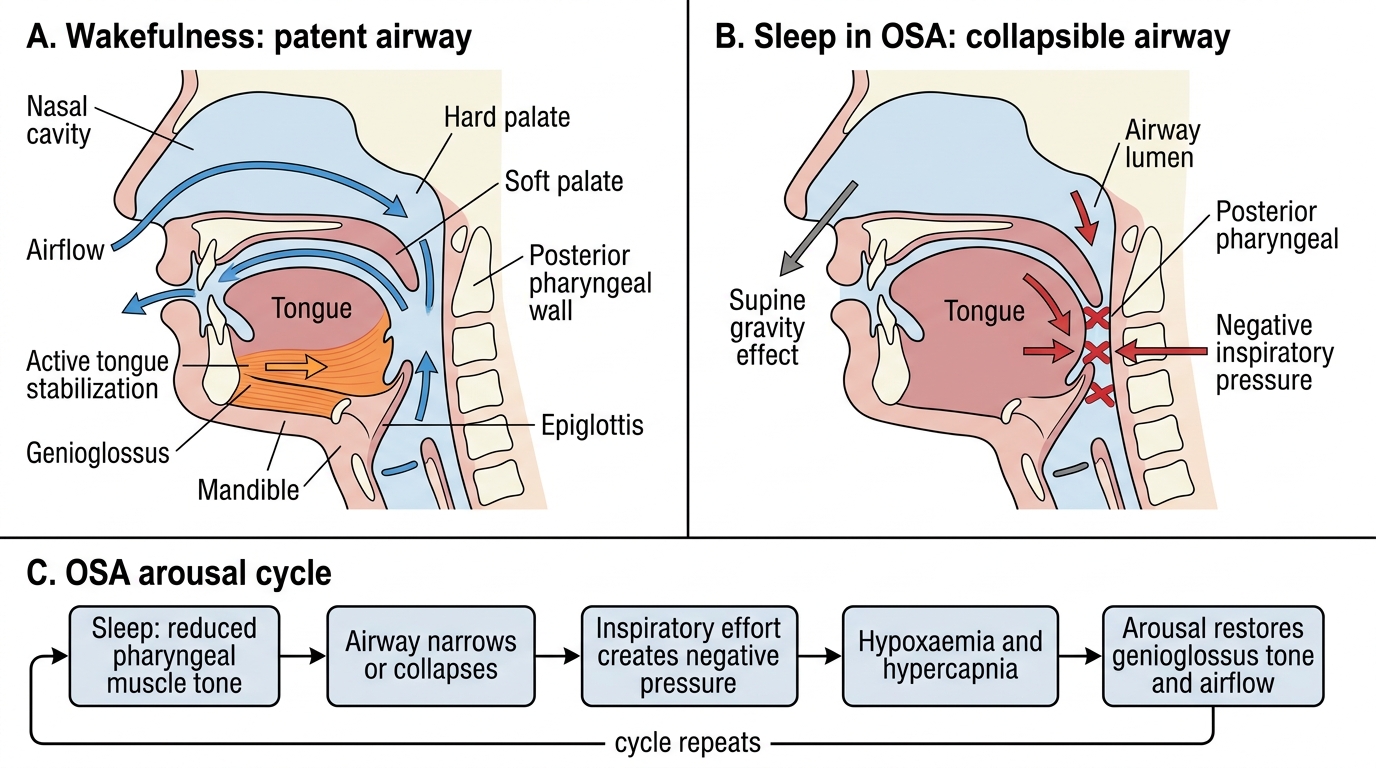
Upper Airway Collapse Mechanism in OSA
SELF-CHECK
A 52-year-old man with OSA reports that his symptoms are much worse when he sleeps on his back than on his side. His wife notes that he snores loudly and has apnoeic episodes only in the supine position. The most likely explanation is:
A. OSA is a Central nervous system disorder worse when brain perfusion is reduced in the supine position
B. Gravity displaces the tongue and soft palate posteriorly when supine, narrowing the oropharyngeal lumen and precipitating airway collapse
C. The diaphragm is compressed by abdominal contents in the supine position, reducing respiratory drive
D. Nasal obstruction is worse when supine because the inferior turbinates engorge in the horizontal position
Reveal Answer
Answer: B. Gravity displaces the tongue and soft palate posteriorly when supine, narrowing the oropharyngeal lumen and precipitating airway collapse
In the supine position, gravity acts on the tongue and soft palate, pulling them posteriorly toward the posterior pharyngeal wall. This reduces the already-narrowed oropharyngeal airway in OSA patients and makes collapse easier during the reduced muscle tone of sleep. Patients whose OSA occurs primarily or exclusively in the supine position ('positional OSA') may be treated effectively with positional therapy (sleeping on the side — lateral decubitus position) using a positional device or a pillow sewn to the back of a sleep-shirt. The inferior turbinate engorgement in the supine position is real (a component of the nasal cycle) but is not the dominant mechanism for positional OSA.
Examination and Investigations
The examination of a patient with suspected OSA is a systematic assessment of the upper airway anatomy and the systemic consequences of OSA. No single examination finding confirms OSA — the diagnosis requires objective sleep study — but examination identifies the anatomical contributors that will guide both selection of treatment modality and surgical planning. A patient with a crowded oropharynx, large tonsils, and a long flaccid soft palate is a candidate for UPPP; a patient with retrognathia is a candidate for a mandibular advancement device or maxillomandibular advancement surgery; a patient whose only abnormality is DNS should have nasal surgery but should not expect it to cure significant OSA alone. Knowing what to look for and how to interpret it is the bridge between the sleep study result and the management plan.
General examination:
- BMI calculation and measurement of neck circumference (>43 cm in men, >41 cm in women = increased risk).
- Blood pressure measurement — hypertension is highly prevalent in OSA and may be a consequence of it.
- Mallampati classification of the oropharyngeal airway (classes I–IV, with III–IV indicating a crowded oropharynx).
Upper airway examination:
- Nasal cavity: anterior rhinoscopy for DNS, turbinate hypertrophy, polyps — nasal obstruction contributes to OSA.
- Oral cavity and oropharynx: tongue size, tonsillar size (graded 1–4 on Friedman/Brodsky scale), length and redundancy of the soft palate and uvula, position of the mandible (retrognathia).
- Neck: assess for retrognathia on lateral profile.
Investigations:
Epworth Sleepiness Scale (ESS): a validated 8-item questionnaire assessing the likelihood of dozing in common situations; score 0–24; score ≥10 indicates clinically significant EDS; score ≥16 indicates severe EDS. Simple, quick screening tool.
STOP-BANG questionnaire: widely used screening tool: Snoring, Tired, Observed apnoeas, blood Pressure, BMI, Age, Neck circumference, Gender — score ≥3 indicates high risk for moderate-severe OSA.
Polysomnography (PSG, full sleep study): the gold standard investigation for diagnosing OSA. Conducted in a sleep laboratory overnight; measures: airflow, respiratory effort, oxygen saturation, EEG (sleep stages), EMG, ECG, body position, and video recording. Generates the Apnoea-Hypopnoea Index (AHI) — the number of apnoeic + hypopnoeic events per hour of sleep.
AHI severity grading:
- AHI <5: normal
- AHI 5–15: mild OSA
- AHI 15–30: moderate OSA
- AHI >30: severe OSA
Home sleep apnea testing (HSAT / level 3 sleep study): portable oximetry + nasal airflow measurement; less comprehensive than full PSG but sufficient to diagnose moderate-severe OSA in high-pre-test-probability patients; available in the community.
Pulse oximetry (overnight): simple, non-invasive; detects repeated oxygen desaturation events; a useful screening tool when PSG is not immediately available; oxygen desaturation index (ODI ≥4% desaturations per hour of ≥5 = significant).