Page 6 of 15
EN3.2 | Diagnostic Nasal Endoscopy — SDL Guide (Part 2)
Procedure: Patient Positioning and Systematic Three-Pass Survey
The three-pass systematic survey is the procedural core of DNE. It ensures that every clinically relevant region of the nasal cavity is inspected in a logical, reproducible sequence. An unstructured examination risks missing the middle meatus (the most important diagnostic zone) because the surgeon becomes preoccupied with a finding in the nasal floor. Each pass is named by the primary region it surveys; within each pass, the surgeon notes specific landmarks and abnormalities.
Patient positioning:
The patient is seated in the ENT chair at a recline of approximately 45° (semi-recumbent), with the head slightly forward (neutral position). This position aligns the nasal floor approximately horizontally, facilitating scope passage along the floor for Pass 1. The surgeon sits or stands at the patient's side (on the ipsilateral side to the nasal cavity being examined), holding the endoscope in the dominant hand like a pencil.
Introducing the endoscope:
The 0° scope is introduced gently through the nostril with the tip directed toward the nasal floor. The light source is turned on before insertion. The endoscope moves inward along the floor of the nasal cavity, maintaining a gentle forward pressure without forcing. If significant resistance is met (polyp, septal deviation, prominent inferior turbinate), the scope is redirected or the preparation repeated with more decongestant.
Pass 1 — Nasal floor, inferior meatus, choana, and nasopharynx (0° scope):
The endoscope advances along the nasal floor, with the inferior turbinate visible superiorly. The space between the inferior turbinate and the nasal floor constitutes the inferior meatus — the opening of the nasolacrimal duct empties here, visible at the anterior end of the inferior turbinate (relevant if nasolacrimal duct obstruction is being assessed). Advancing further, the scope reaches the posterior choana — the posterior nasal aperture. Passing through the choana, the nasopharynx is reached: the surgeon inspects the adenoid (on the roof and posterior wall — prominent in children), the Eustachian tube orifice (visible on the lateral wall on each side, with the torus tubarius — the posterior lip of the ET opening), and the fossa of Rosenmüller (the recess posterior to the torus tubarius — an important site for nasopharyngeal carcinoma). Any mass, mucosal irregularity, or asymmetry is documented.
Pass 2 — Middle meatus and ostiomeatal complex (0° or 30° scope):
The scope is withdrawn slightly from the nasopharynx and redirected superiorly, passing between the inferior turbinate and the middle turbinate. The middle meatus comes into view. Key structures to identify:
- The middle turbinate (medially) and the lateral nasal wall (laterally)
- The uncinate process — a thin bony projection from the lateral wall, the anterior boundary of the hiatus semilunaris
- The hiatus semilunaris — the crescentic gap between the uncinate process and the bulla ethmoidalis; the drainage channel for the maxillary, anterior ethmoidal, and frontal sinuses
- The bulla ethmoidalis — the most anterior and largest anterior ethmoidal air cell, forming the posterior boundary of the hiatus
- The maxillary sinus ostium — visible at the posterior end of the infundibulum in the hiatus semilunaris
The 30° scope angle is used to look 'over' the middle turbinate into the hiatus and infundibulum when the 0° view is obstructed.
Pass 3 — Sphenoethmoid recess and superior meatus (0° scope):
The scope is now directed medially and superiorly, between the middle turbinate and the nasal septum, toward the superior turbinate. The sphenoethmoid recess — the narrow space between the superior turbinate and the septum — receives drainage from the sphenoid sinus (via the sphenoidal ostium visible on the anterior face of the sphenoid) and the posterior ethmoid air cells. Disease here explains recurrent sphenoid sinusitis and posterior ethmoid disease.
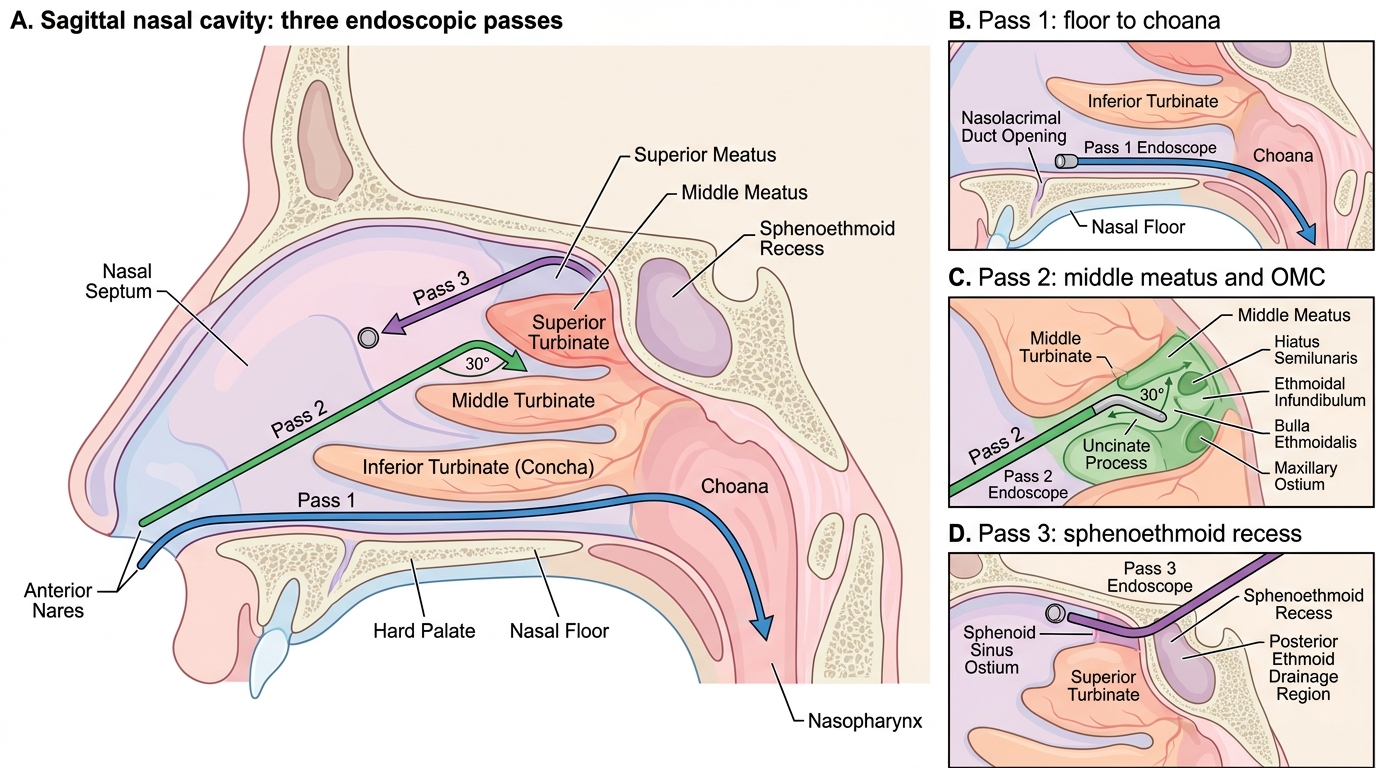
Diagnostic Nasal Endoscopy: Three Endoscopic Passes
SELF-CHECK
During Pass 2 of a diagnostic nasal endoscopy, the surgeon uses a 30° endoscope to look into the middle meatus. The key drainage complex for the maxillary, frontal, and anterior ethmoidal sinuses that is visible here is:
A. The sphenoethmoid recess, between the superior turbinate and the septum
B. The ostiomeatal complex, including the hiatus semilunaris and the maxillary ostium
C. The nasolacrimal duct opening in the anterior inferior meatus
D. The fossa of Rosenmüller posterior to the torus tubarius
Reveal Answer
Answer: B. The ostiomeatal complex, including the hiatus semilunaris and the maxillary ostium
The ostiomeatal complex (OMC) — comprising the maxillary ostium, infundibulum, hiatus semilunaris, bulla ethmoidalis, and middle meatus — is the functional drainage pathway for the maxillary, anterior ethmoidal, and frontal sinuses. It is located in the middle meatus and is the target of Pass 2. The 30° scope angle is used because the OMC lies 'around the corner' of the middle turbinate, hidden from a straight 0° view. The sphenoethmoid recess drains the sphenoid and posterior ethmoid (Pass 3). The nasolacrimal duct opens in the inferior meatus (Pass 1). The fossa of Rosenmüller is in the nasopharynx (Pass 1 — nasopharyngeal view).
Interpretation of Diagnostic Nasal Endoscopy Findings
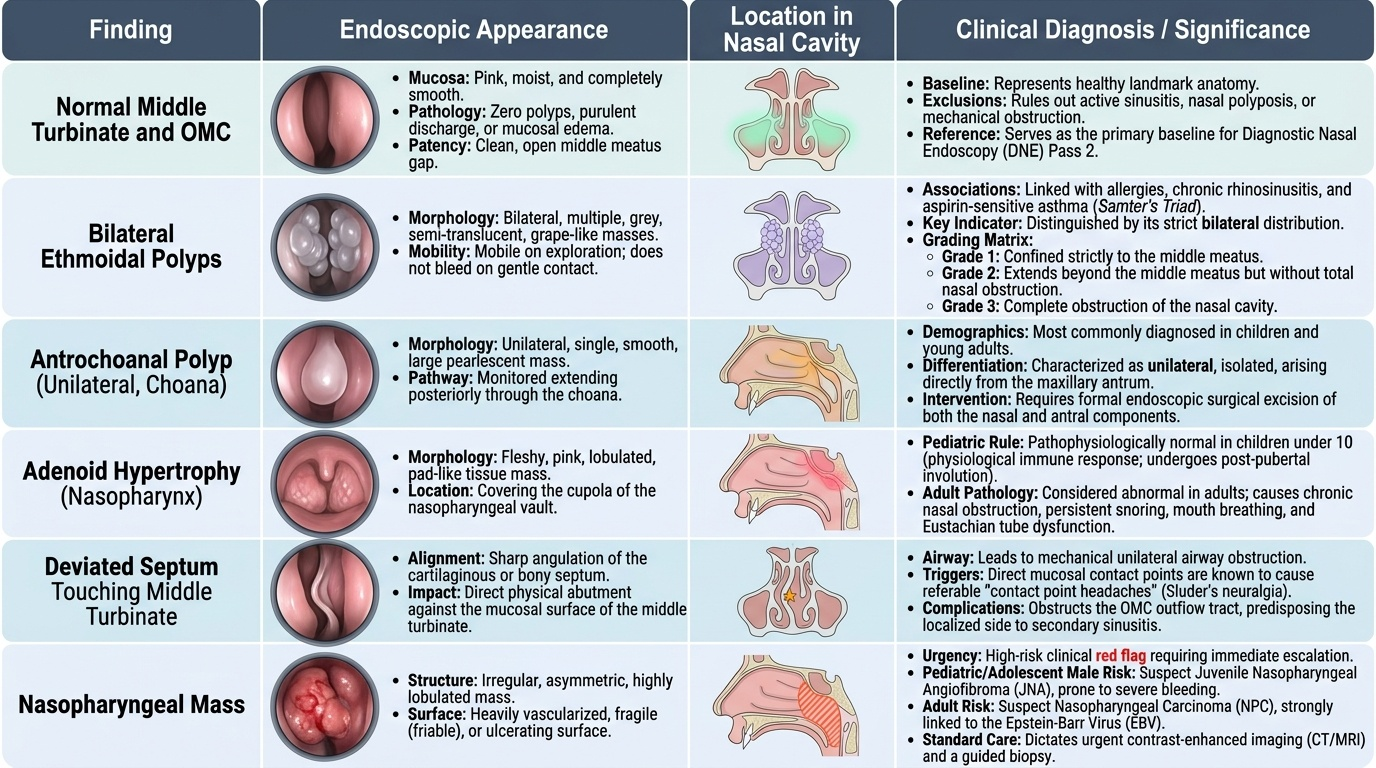
Interpreting DNE findings requires a systematic comparison of what is seen against the expected normal endoscopic anatomy. The most clinically important interpretive task is distinguishing bilateral from unilateral disease, because this distinction drives the diagnostic pathway and the urgency of referral.
Provided image
Normal endoscopic nasal anatomy:
Normal nasal mucosa appears pink, moist, and smooth. The middle turbinate is the dominant structure of Pass 2 — it should not be polypoid. The middle meatus is a visible gap between the middle turbinate and the lateral wall. The hiatus semilunaris and the uncinate process are visible as thin mucosal-covered bony structures. No polyps, no purulent discharge, no mucosal oedema occluding the hiatus. The nasopharynx in adults is clear of adenoid tissue (involuted after puberty); in children under 10, some adenoid tissue at the roof is normal.
Bilateral ethmoidal nasal polyps:
The endoscopic hallmark is bilateral, multiple, grey, semi-translucent, grape-like masses emerging from the middle meatus and spilling into the nasal cavity. They arise from the ethmoidal mucosa and are associated with allergy, chronic rhinosinusitis, and aspirin-sensitive asthma (Samter's triad). They are mobile (unlike tumours) and do not bleed spontaneously on gentle probing. Grading: Grade 1 = polyps confined to middle meatus; Grade 2 = polyps beyond middle meatus but not obstructing the nostril; Grade 3 = complete obstruction of the nostril. Bilateral distribution is the critical feature distinguishing ethmoidal polyps from the unilateral antrochoanal polyp.
Antrochoanal polyp (Killian's polyp):
A unilateral, single, smooth polyp arising from the mucosa of the maxillary antrum (sinus), which passes through the accessory maxillary ostium or the widened natural ostium, fills the middle meatus, and extends posteriorly to protrude through the choana into the nasopharynx — visible on Pass 1 of the endoscopy as a polypoid mass hanging through the choana. The antrochoanal polyp is most common in children and young adults. Its key distinguishing features from ethmoidal polyps: it is unilateral, single, arises from the maxillary antrum, and extends to the choana/nasopharynx. Management is surgical excision (endoscopic removal of both the nasal portion and the antral component).
KEY EN KNOWN-TRAP: Bilateral polyps = ethmoidal/allergic; unilateral polyp = suspect antrochoanal or neoplasm. Never swap laterality.
Deviated nasal septum and its effect on the OMC:
A deviated nasal septum (DNS) may compress the middle turbinate against the lateral wall, narrowing or obliterating the middle meatus and impairing OMC drainage. Endoscopy demonstrates the contact point and its effect on the hiatus semilunaris. DNS contributing to OMC blockage is an indication for septoplasty combined with FESS.
Adenoid hypertrophy:
In children, endoscopic Pass 1 through the choana to the nasopharynx shows hypertrophied adenoid tissue filling the nasopharynx and partially or completely obstructing the choanae. In severe cases the Eustachian tube orifice is obstructed, contributing to OME. Endoscopy replaces plain lateral X-ray of the nasopharynx (which was the older investigation for adenoid assessment) as the gold standard.
Nasopharyngeal mass — JNA and malignancy:
Any mass in the nasopharynx visible on endoscopy must be assessed systematically. In an adolescent male with recurrent epistaxis and nasal obstruction, a vascular, pulsatile mass in the nasopharynx suggests juvenile nasopharyngeal angiofibroma (JNA). This is an extremely vascular benign tumour. DO NOT BIOPSY at outpatient endoscopy — catastrophic haemorrhage can result. Diagnosis is made by contrast CT or MRI and angiography. In an older adult, a firm, irregular, ulcerated mass in the fossa of Rosenmüller suggests nasopharyngeal carcinoma — this requires biopsy under general anaesthesia.
CLINICAL PEARL
The single most important interpretive rule in diagnostic nasal endoscopy is the laterality of nasal polyps: bilateral polyps = ethmoidal origin (allergic, CRS) = medical management first (topical steroids, allergen control, FESS if refractory); unilateral polyp = always investigate further — an antrochoanal polyp needs surgery, but a unilateral nasal mass in an adolescent male must first have contrast CT to exclude JNA before any attempt at biopsy or manipulation. Forgetting the laterality rule leads to either over-investigating a patient with straightforward bilateral allergic polyps, or — far more dangerously — biopsying a JNA in clinic and triggering a catastrophic haemorrhage. This laterality rule is non-negotiable.
Applied Practice: Case Scenarios
These three cases reinforce the key interpretive decisions from DNE. For each, form your diagnosis and management plan before reading the discussion.
Case 1 — The patient with chronic bilateral nasal obstruction and anosmia:
A 38-year-old man with a 5-year history of bilateral nasal obstruction, anosmia, recurrent maxillary sinusitis, and a diagnosis of intrinsic asthma presents for ENT assessment. Anterior rhinoscopy shows no visible pathology. DNE after decongestion: bilateral grey semi-translucent grape-like masses filling both middle meatuses and extending anteriorly to partially obstruct the nasal cavity. No mucosal ulceration or bleeding on probing. CT sinuses: bilateral opacification of the ethmoid sinuses with soft-tissue density extending into the nasal cavity.
Interpretation: Bilateral ethmoidal nasal polyps, Grade 2 (beyond middle meatus, not fully obstructing the nostril). The association of nasal polyps + asthma raises the possibility of Samter's triad (aspirin-sensitive asthma + nasal polyps + chronic rhinosinusitis).
Management: Medical treatment first: high-dose intranasal corticosteroids + short course of oral steroids. If no response: FESS for bilateral ethmoidectomy and polypectomy. Allergy assessment. Enquire about aspirin sensitivity.
Case 2 — The child with unilateral nasal obstruction:
A 14-year-old boy presents with progressive right-sided nasal obstruction for 8 months, no fever, mild right-sided nasal discharge, no epistaxis. DNE: a smooth, pale, single polypoid mass visible in the right middle meatus, extending posteriorly; on Pass 1, a polypoid mass is seen prolapsing through the right choana into the nasopharynx. The left nasal cavity is normal.
Interpretation: Right antrochoanal polyp (Killian's polyp). The key diagnostic features: unilateral, single, smooth mass in the middle meatus extending to the choana and visible on both Pass 2 and Pass 1. The left side is completely normal — ruling out bilateral ethmoidal disease.
Management: CT sinuses to confirm origin from the right maxillary antrum and plan surgery. Endoscopic excision of both the nasal portion and the antral component through the middle meatus (not just snaring the nasal portion, which leaves the antral component and leads to recurrence).
Case 3 — The adolescent male with epistaxis and nasopharyngeal mass:
A 16-year-old boy presents with recurrent right-sided epistaxis (three episodes over 4 months, requiring nasal packing on two occasions) and progressive right nasal obstruction. DNE: on Pass 1 advancing to the nasopharynx, a firm, smooth, pinkish-red pulsatile mass is seen occupying the right nasopharynx and posterior choana. The mass appears vascular on the mucosal surface.
Interpretation: Juvenile nasopharyngeal angiofibroma (JNA) must be excluded. This is a 16-year-old male with recurrent severe epistaxis and a pulsatile, vascular-appearing nasopharyngeal mass — the classic presentation.
Management: DO NOT BIOPSY in the outpatient clinic — catastrophic haemorrhage risk. Arrange contrast CT and MRI of the nasopharynx and skull base urgently. Angiography may be required to assess vascular supply before planned surgery. Refer urgently to a tertiary ENT centre with skull base surgical capability.
SELF-CHECK
A 15-year-old boy presents with recurrent profuse right-sided nosebleeds and right nasal obstruction. On diagnostic nasal endoscopy, a smooth, pulsatile, pinkish mass is seen in the right nasopharynx extending to the right choana. The most appropriate next step is:
A. Perform a biopsy of the mass under local anaesthesia in the outpatient clinic
B. Request contrast CT and MRI of the nasopharynx — do not biopsy; refer urgently to tertiary ENT
C. Prescribe a topical nasal steroid spray for 6 weeks and reassess
D. Perform anterior nasal packing and discharge with oral iron supplementation
Reveal Answer
Answer: B. Request contrast CT and MRI of the nasopharynx — do not biopsy; refer urgently to tertiary ENT
A pulsatile vascular nasopharyngeal mass in an adolescent male with recurrent severe epistaxis is juvenile nasopharyngeal angiofibroma (JNA) until proven otherwise. JNA is an extremely vascular benign tumour — outpatient biopsy carries a risk of catastrophic, potentially fatal haemorrhage. Diagnosis is established by contrast CT/MRI (which shows characteristic enhancement and bony erosion patterns) and angiography. Management is surgical excision, often preceded by embolisation. This is the classic 'do NOT biopsy' ENT scenario. Topical steroids treat inflammatory polyps, not vascular tumours. Packing manages the acute bleed but does not address the underlying lesion.
Self-Assessment
Before your ENT clinical posting, use these questions to confirm your readiness to observe and contribute to a diagnostic nasal endoscopy session. Each question maps to a specific arc step of the EN-skills framework. A student who can describe the indications and three-pass technique but cannot correctly interpret the key finding — specifically the bilateral versus unilateral polyp distinction and the JNA do-not-biopsy rule — has not yet met the competency standard. These are not abstract facts; they are the clinical decisions that prevent harm and ensure the right referral is made promptly. The three-pass technique described in this SDL is the same one used in every ENT outpatient department in India and internationally — your ability to describe it accurately in an OSCE or clinical examination reflects your readiness for the ENT posting and, later, for primary-care practice where you will need to know which nasal symptoms require urgent ENT referral versus which can be managed with a topical steroid. Work through each question before looking at the answers, then re-read the relevant section for any question you find difficult.
- Name three clinical indications for DNE that cannot be adequately assessed by anterior rhinoscopy alone.
- What is the Hopkins rod lens system? Why does it produce a brighter and higher-quality image than a conventional telescope?
- Name the three standard endoscope angles and state which region of the nasal cavity each is used to inspect.
- Describe the three passes of the systematic nasal endoscopic survey. Name the two most important structures inspected on each pass.
- A patient has bilateral grey grape-like masses in both middle meatuses. A second patient has a single smooth mass in the right middle meatus extending to the right choana. State the diagnosis for each patient and the key distinguishing feature.
- During endoscopy, a pulsatile vascular mass is seen in the nasopharynx of a 17-year-old male. What is the critical management rule, and why?
If you cannot answer question 6, revisit the JNA section — the 'do not biopsy' rule is non-negotiable and potentially life-saving.