Page 8 of 21
EN4.31 | Nasopharyngeal Angiofibroma — SDL Guide
Learning Objectives
- Describe the clinical features of juvenile nasopharyngeal angiofibroma (JNA), including the classic triad and demographic profile
- Explain why biopsy is absolutely contraindicated and describe the correct diagnostic approach using contrast CT, MRI, and angiography
- Outline the principles of management including pre-operative embolisation and surgical excision
- Distinguish JNA from other causes of unilateral nasal obstruction in adolescent males
INSTRUCTIONS
Juvenile nasopharyngeal angiofibroma is a rare but intensely high-yield topic for ENT examinations and clinical practice because its management involves one absolute rule that must never be violated: do not perform a biopsy. A student who correctly identifies the clinical presentation, orders the right investigations, and withholds biopsy has demonstrated the essence of this competency. The module also illustrates how a thorough understanding of anatomy — specifically the sphenopalatine foramen and the pterygomaxillary fossa — explains both the origin and the surgical management of this tumour.
References
- Dhingra PL — Diseases of Ear, Nose & Throat, 7th ed., Ch 35 (textbook)
- Hazarika P — Textbook of ENT and Head & Neck Surgery, 3rd ed., Ch 28 (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed., Vol 2, Rhinology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 15-year-old boy is brought to the ENT outpatient clinic by his mother with a 6-month history of progressive right-sided nasal blockage and three episodes of severe, spontaneous right-sided nosebleeds, the last of which required emergency nasal packing at a peripheral hospital. He has no fever, no weight loss, and the nasal blockage has progressively worsened over the past 3 months. On anterior rhinoscopy you see a fleshy, pinkish-red mass in the right nasal cavity. It fills most of the right nostril. The patient is apyrexial and otherwise well. A junior colleague prepares to take a biopsy forceps to sample the mass. What do you say, and why?
WHY THIS MATTERS
Juvenile nasopharyngeal angiofibroma, despite its rarity (approximately 1 per 150,000 ENT consultations), is one of the most important conditions to know in ENT for three reasons. First, the demographic and clinical profile is so distinctive — adolescent male, recurrent severe epistaxis, progressive nasal obstruction — that the diagnosis should be made clinically before any investigation is ordered. Second, the rule against biopsy is absolute and consequential: a biopsy performed in a clinic or outpatient setting can trigger haemorrhage that fills the nasopharynx and cannot be controlled without surgical intervention, causing preventable catastrophe. Third, JNA illustrates a general principle of vascular tumour surgery: pre-operative devascularisation by embolisation is what makes excision of a tumour fed by the internal maxillary artery both feasible and safe. For the final-year student, this module delivers the knowledge content required by competency EN4.31 (KH level, K domain) and reinforces the broader diagnostic principle that a unilateral, vascular nasal mass in a young male is JNA until proven otherwise.
RECALL
Recall from your anatomy teaching that the pterygopalatine fossa (also called the pterygomaxillary fossa) is a small pyramidal space behind the maxillary sinus, bounded by the posterior wall of the maxillary sinus anteriorly, the pterygoid plates posteriorly, and the palatine bone medially. It is a key anatomical crossroads: the sphenopalatine foramen opens medially from the pterygopalatine fossa into the posterior nasal cavity, transmitting the sphenopalatine artery (the terminal branch of the internal maxillary artery and the dominant blood supply to the posterior nasal cavity) and the nasopalatine nerve. The pterygopalatine fossa also communicates with the infratemporal fossa laterally (via the pterygomaxillary fissure), the orbit superiorly (via the inferior orbital fissure), the oral cavity inferiorly (via the greater and lesser palatine canals), and the middle cranial fossa superiorly (via the foramen rotundum and vidian canal). This explains why JNA, which arises near the sphenopalatine foramen, has multiple routes of spread and why complete surgical excision requires approaching through multiple planes.
Clinical Presentation of Juvenile Nasopharyngeal Angiofibroma
The clinical presentation of JNA is so characteristic that in the correct demographic context — adolescent male, typically 10–25 years — the diagnosis should be strongly suspected from the history alone. The classic presenting triad is: progressive unilateral nasal obstruction, recurrent spontaneous epistaxis (often severe and difficult to control), and a visible or palpable nasopharyngeal mass. Each element has distinctive features that distinguish JNA from other causes of nasal obstruction.
Nasal obstruction is typically unilateral at first (because the tumour originates unilaterally, near the sphenopalatine foramen), progressive over months, and eventually may cause bilateral obstruction as the tumour enlarges into the nasopharynx. Unlike inflammatory nasal obstruction (which fluctuates and responds partially to decongestants), JNA-related obstruction is progressive and structural — it does not respond to medical treatment.
Epistaxis is the hallmark symptom and the feature that drives most patients to seek medical attention. It is characteristically spontaneous (not provoked by trauma), severe (often requiring packing or transfusion), and recurrent — patients may present after multiple pack-and-discharge episodes at primary care facilities without a definitive diagnosis. The massive bleeding reflects the histological architecture of JNA: it is composed of a fibrous stroma in which numerous thin-walled vascular channels lack a muscular media, meaning that when they are torn (as in minor mucosal trauma or attempted biopsy), the vessels cannot contract to achieve haemostasis. The result is uncontrolled haemorrhage.
Additional features in advanced disease include: anosmia (bilateral blockage extending to the olfactory cleft), rhinolalia clausa (hyponasal speech from nasopharyngeal obstruction), cheek swelling (involvement of the pterygomaxillary fossa or anterior extension into the maxillary sinus), proptosis (orbital extension through the inferior orbital fissure), and temporal fossa swelling (infratemporal fossa involvement). Intracranial extension may produce headache, cranial nerve deficits, or raised intracranial pressure, though this is fortunately rare at presentation.
Epidemiology and hormonal basis: JNA occurs almost exclusively in males between 10 and 25 years, with a peak incidence at 14–17 years. Reports of JNA in females are exceedingly rare (and many historical cases were probably not true JNA). Testosterone receptor expression within the tumour fibroblasts has been demonstrated histologically, and the growth of JNA parallels puberty, with spontaneous regression sometimes observed after puberty in small tumours. This hormonal basis historically motivated the use of oestrogen therapy to shrink tumours pre-operatively, though this approach has been largely abandoned in favour of embolisation.
Anatomy and Pathophysiology of JNA
Understanding the anatomy of JNA's origin and spread routes is the key to understanding both why it presents as it does and how it is approached surgically at different stages.
Site of origin: JNA arises from the fibrovascular stroma of the posterolateral wall of the nasal cavity near the sphenopalatine foramen, at the superior margin of the sphenopalatine foramen and the adjacent periosteum of the pterygoid base. The tumour is not truly a 'nasopharyngeal' tumour in origin (despite the traditional name) — it arises in the posterior nasal cavity and secondarily fills the nasopharynx as it grows posteriorly. The sphenopalatine foramen location explains the dominant blood supply: the internal maxillary artery (a branch of the external carotid artery) via the sphenopalatine artery is the primary feeder in early-stage disease. As the tumour grows and extends intracranially, internal carotid artery branches (via the vidian artery or cavernous ICA) may also contribute.
Histology: JNA has a characteristic biphasic histological pattern — a fibrous stroma (containing fibroblasts and myofibroblasts) interspersed with thin-walled, endothelium-lined vascular channels that lack a muscular media. The absence of smooth muscle in the vessel walls is the key pathological feature that explains the inability to achieve spontaneous haemostasis: when these vessels are torn, they cannot contract. The stroma contains cells expressing testosterone receptors, androgen receptors, and vascular endothelial growth factor (VEGF), supporting both the hormonal hypothesis and the tumour's aggressive angiogenic behaviour.
Routes of spread (by stage):
- Stage I: Tumour confined to the nasal cavity and/or nasopharynx. Minimal bony involvement.
- Stage II: Extension into the pterygomaxillary fossa, paranasal sinuses (maxillary, ethmoidal, sphenoidal), or infratemporal fossa.
- Stage III: Extension into the orbit (via inferior orbital fissure) or parasellar region (into the cavernous sinus area, lateral to the sella).
- Stage IV: Intracranial extension with or without cavernous sinus involvement.
The Fisch staging and the Andrews-Ward modifications are the most widely used systems; staging determines the surgical approach.
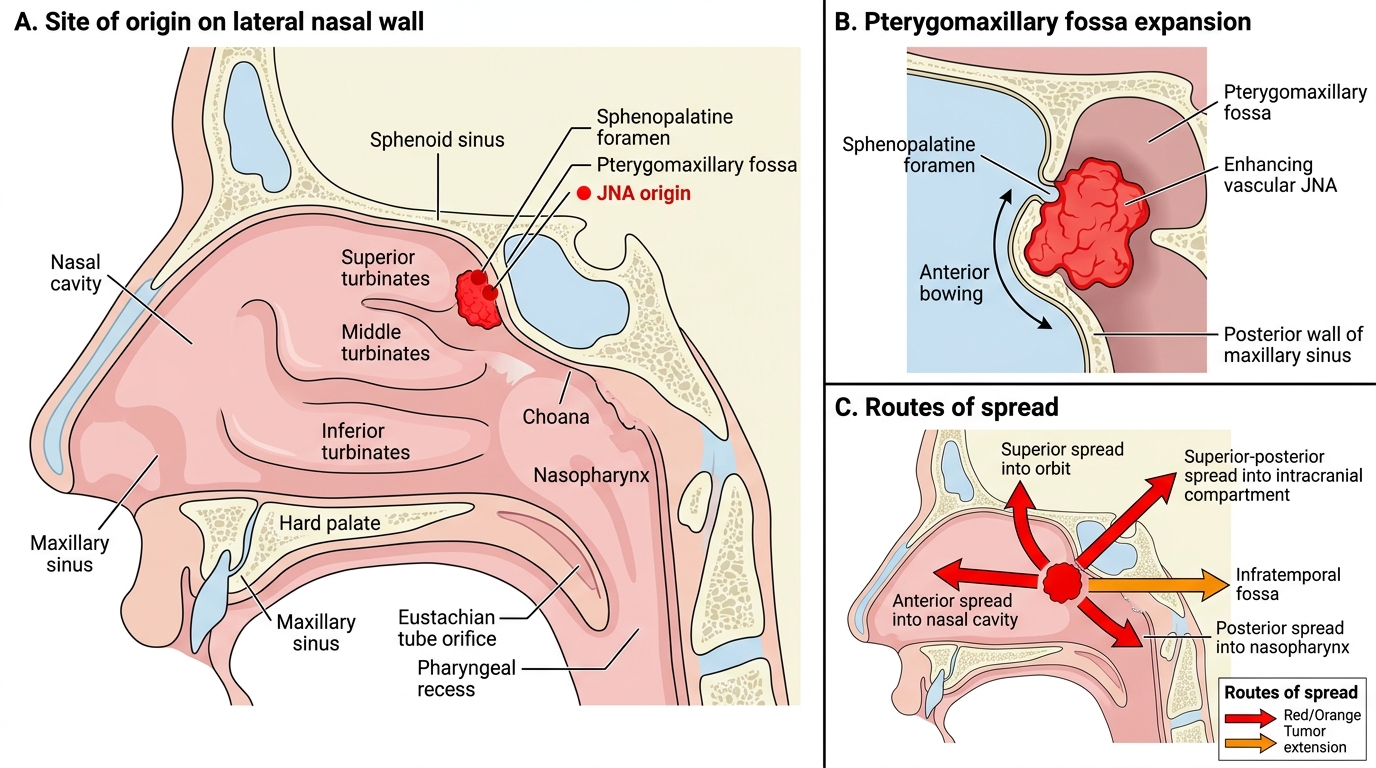
Juvenile Nasopharyngeal Angiofibroma: Site of Origin and Routes of Spread
SELF-CHECK
A 16-year-old boy presents with recurrent severe epistaxis and progressive right nasal obstruction. Anterior rhinoscopy reveals a pinkish-red vascular mass filling the right nasal cavity. Which single investigation is MOST appropriate as the first imaging step?
A. Plain X-ray of the paranasal sinuses (Waters' view) to screen for sinus opacification
B. Contrast CT scan of the nose and paranasal sinuses to characterise the mass and define its extent
C. Nasal endoscopy with biopsy under local anaesthesia to obtain tissue diagnosis
D. Ultrasound of the neck to assess for lymph node involvement
Reveal Answer
Answer: B. Contrast CT scan of the nose and paranasal sinuses to characterise the mass and define its extent
Contrast CT of the nose and paranasal sinuses is the first imaging investigation of choice for a suspected JNA. It demonstrates the characteristic features — a brightly enhancing vascular mass in the posterior nasal cavity and nasopharynx, with the pathognomonic 'Holman-Miller sign' (anterior bowing of the posterior wall of the maxillary sinus from expansion of the pterygomaxillary fossa), and defines tumour extent for staging. Plain X-ray is inadequate for soft-tissue characterisation. Biopsy is absolutely contraindicated — it can provoke catastrophic, uncontrollable haemorrhage in the clinic or outpatient setting. Ultrasound provides no useful information about a nasopharyngeal vascular mass.
Investigations: Why Biopsy Is Contraindicated and How to Diagnose JNA
The investigation of JNA is defined by one categorical rule and a sequence of imaging that collectively confirm the diagnosis, define the extent of disease, and map the vascular supply for surgical planning. The categorical rule — do not biopsy — is the most examined and most important point in this entire module.
Why biopsy is contraindicated: JNA is composed of thin-walled vascular channels without a muscular media. When these channels are disrupted by biopsy forceps, they cannot undergo physiological vasospasm. Massive arterial-pressure haemorrhage from the internal maxillary artery distribution pours into the nasopharynx. In an outpatient or clinic setting, without anaesthetic support, suction, or surgical access, this haemorrhage cannot be controlled. Patients have exsanguinated from attempted office biopsies of JNA. The clinical and imaging profile is so characteristic that histological confirmation is not required before surgical planning. If the clinical presentation matches JNA in an adolescent male, the correct response is imaging — not biopsy.
Contrast CT of the paranasal sinuses: This is the first-line investigation. Key CT findings include:
- A brightly enhancing mass in the posterior nasal cavity and nasopharynx (reflecting the high vascularity);
- Holman-Miller sign: anterior bowing of the posterior wall of the maxillary sinus — caused by the tumour filling and expanding the pterygomaxillary fossa, pushing the posterior maxillary wall forward; this sign, when present, is pathognomonic for JNA;
- Widening of the sphenopalatine foramen;
- Extension into the pterygomaxillary fossa, infratemporal fossa, sinuses, or orbit if advanced.
MRI of the nasopharynx and skull base: MRI provides superior soft-tissue delineation, particularly for detecting intracranial extension (parasellar involvement, cavernous sinus) and for delineating the tumour margins from adjacent soft tissues. On T1-weighted MRI, JNA shows flow voids (reflecting high vascularity) within the tumour mass. MRI is complementary to CT and is used in all patients being considered for surgery to define the intracranial extent.
Angiography and pre-operative embolisation: Digital subtraction angiography (DSA) identifies the feeding vessels (most commonly branches of the internal maxillary artery, less commonly the accessory meningeal artery or internal carotid artery branches in advanced disease). Pre-operative selective angiographic embolisation is performed 24–48 hours before surgical excision, blocking the dominant blood supply to dramatically reduce intraoperative haemorrhage. Without embolisation, blood loss during JNA excision can be massive.
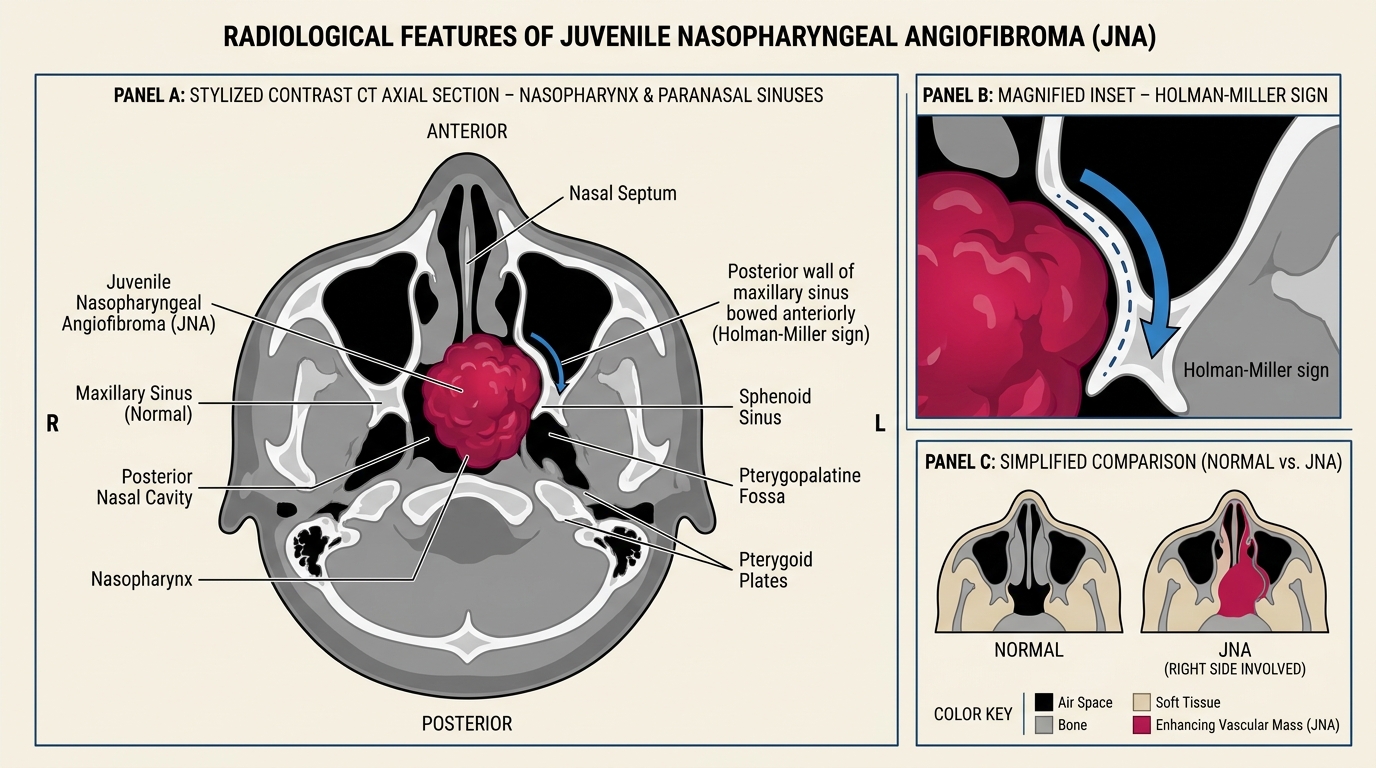
Axial Contrast CT Features of Juvenile Nasopharyngeal Angiofibroma