Page 11 of 21
EN4.33 | Tumours of Nose, Nasopharynx and Paranasal Sinuses — SDL Guide
Learning Objectives
- Describe the clinical features of benign and malignant tumours of the nose, paranasal sinuses, and nasopharynx
- Choose appropriate investigations including nasal endoscopy, CT, MRI, and biopsy, and justify when biopsy should be deferred
- Outline the staging of maxillary sinus carcinoma and nasopharyngeal carcinoma
- Describe the principles of management of sinonasal malignancy and nasopharyngeal carcinoma
INSTRUCTIONS
Tumours of the nose, paranasal sinuses, and nasopharynx are rare but carry a heavy diagnostic burden because they present late — often after months of symptoms attributed to 'sinusitis' or 'nasal congestion.' The student who knows the warning features of sinonasal malignancy (unilateral symptoms, blood-stained discharge, bone erosion on imaging, cranial nerve involvement) and the distinctive epidemiological signature of nasopharyngeal carcinoma (EBV, Asian/African ethnicity, cervical lymphadenopathy as first presentation) will save patients from diagnostic delay. This module also reinforces the critical distinction between benign nasopharyngeal tumours (JNA — do not biopsy) and malignant ones (NPC — biopsy essential).
References
- Dhingra PL — Diseases of Ear, Nose & Throat, 7th ed., Ch 36-38 (textbook)
- Hazarika P — Textbook of ENT and Head & Neck Surgery, 3rd ed., Ch 29-31 (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed., Vol 2, Rhinology and Head and Neck (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old male farmer presents with a 4-month history of left-sided nasal blockage and blood-stained nasal discharge. He saw a doctor two months ago who prescribed antibiotics for 'sinusitis,' with no improvement. Now he has developed left facial swelling below the eye, paraesthesia over the left cheek, and his upper left molar teeth feel 'loose.' On examination there is a firm, non-tender swelling of the left cheek. Anterior rhinoscopy reveals a fleshy, irregular mass in the left nasal cavity that bleeds on touch. What is the most likely diagnosis, and what features in this history should have prompted earlier investigation for malignancy?
WHY THIS MATTERS
Sinonasal malignancies are uncommon (1–2% of all head and neck cancers, <0.5% of all malignancies) but are characterised by late diagnosis because the paranasal sinuses are a 'silent' anatomical region — symptoms appear only after the tumour has expanded beyond its sinus of origin and invaded adjacent structures. For practical purposes, the clinician must maintain a high index of suspicion for malignancy in any patient with: unilateral nasal symptoms, blood-stained nasal discharge, facial swelling, tooth loosening (maxillary sinus floor invasion), cranial nerve symptoms, or 'sinusitis' that does not respond to standard medical treatment. Nasopharyngeal carcinoma (NPC) has a distinct epidemiological profile — strongly associated with EBV, endemic in East and Southeast Asia and parts of North Africa, and classically presenting with painless cervical lymphadenopathy as the first sign, often in a young adult. Missing NPC costs years of cure-rate benefit, as early-stage NPC is eminently curable with concurrent chemoradiotherapy. The competency EN4.33 (KH level, K domain) requires knowledge of clinical features, investigations, and management principles across this range of tumours.
RECALL
Recall from your anatomy that the maxillary sinus (the largest of the paranasal sinuses) is a pyramid-shaped cavity within the maxillary bone. Its walls are: the anterolateral wall (facial surface — palpable on cheek), the posterior wall (separating it from the infratemporal/pterygomaxillary fossa), the medial wall (lateral nasal wall, contains the natural ostium draining to the middle meatus), the roof (orbital floor — contains the infraorbital nerve in the infraorbital canal), and the floor (alveolar process — in contact with the upper molar and premolar roots). This anatomy explains the spread patterns of maxillary sinus malignancy: upward invasion → orbital floor (proptosis, infraorbital nerve paraesthesia); backward invasion → pterygopalatine fossa and infratemporal fossa; medial invasion → nasal cavity; downward invasion → hard palate and upper teeth (dental loosening); anterior invasion → cheek. Recall from pathology that squamous cell carcinoma (SCC) is the most common histological type in the upper aerodigestive tract and that Epstein-Barr virus (EBV) is the key oncogenic driver of nasopharyngeal carcinoma.
Clinical Presentation of Nasal and Nasopharyngeal Tumours
The clinical presentation of sinonasal and nasopharyngeal tumours depends on the site of origin and the extent of spread at the time of diagnosis. Because most of these tumours arise in enclosed spaces with no early symptoms, patients typically present at a late stage. Recognising the warning features that distinguish tumours from inflammatory disease is the clinician's primary obligation. The maxillary sinus is particularly notorious for 'silent' disease — it can accommodate a large tumour before any symptom is produced, and by the time symptoms appear, the tumour has usually grown beyond the sinus walls to invade the orbit, pterygomaxillary fossa, or hard palate. In contrast, nasal cavity tumours present somewhat earlier because nasal obstruction and epistaxis are noticed more readily. Nasopharyngeal carcinoma has an entirely different and deceptive presentation — the first clinically apparent sign is often a cervical lymph node, and the primary tumour in the nasopharynx may be subclinical for months. The student's task in the history is to identify the combination of site-specific symptoms and red-flag features that mandate immediate endoscopic and imaging investigation rather than empirical antibiotic treatment.
Presentations of nasal and paranasal sinus tumours:
- Unilateral nasal obstruction that is progressive and does not respond to standard treatment for rhinitis or sinusitis. Bilateral disease is uncommon until very advanced. Unilateral symptoms in middle-aged or elderly adults should always raise the possibility of a structural pathology.
- Blood-stained nasal discharge or epistaxis: a key red flag. Inflammatory nasal disease (polyps, sinusitis) rarely produces persistent blood-stained discharge. Epistaxis associated with a unilateral mass, particularly in older adults, mandates endoscopy and imaging.
- Facial pain or swelling: involvement of the maxillary sinus anterolateral wall produces cheek swelling; involvement of the orbital floor produces infraorbital nerve paraesthesia (cheek numbness — a sign of advanced disease).
- Loosening of upper teeth or palatal swelling: invasion through the floor of the maxillary sinus into the alveolar process; a molar root that abuts the sinus floor can loosen.
- Orbital symptoms: proptosis, diplopia, reduced vision from floor-of-orbit or periorbital invasion.
- Trismus (restriction of mouth opening): pterygoid muscle involvement from posterior maxillary or infratemporal fossa extension.
- Cranial nerve deficits: infraorbital nerve (CN V2, cheek paraesthesia), vidian nerve (dry eye, dry mouth from secretomotor disruption), or advanced skull base involvement.
Presentations of nasopharyngeal carcinoma (NPC):
NPC has a distinctive and often deceptive clinical presentation because the nasopharynx is not directly visible without posterior rhinoscopy or nasopharyngoscopy. The classic presentation follows three patterns:
- Cervical lymphadenopathy (most common first presentation, 50–60% of patients): painless, firm, and often bilateral upper cervical lymph nodes, particularly in the posterior triangle. A young adult with unexplained upper deep cervical lymphadenopathy — especially in an Asian or African patient — should be investigated for NPC with nasopharyngoscopy before any other head and neck cause is assumed.
- Nasal symptoms: unilateral nasal obstruction, epistaxis, and post-nasal discharge. These are often attributed to 'sinusitis' early in the disease.
- Aural symptoms: unilateral conductive hearing loss and tinnitus from obstruction of the Eustachian tube at its nasopharyngeal opening, producing a secretory otitis media (glue ear) on the affected side. Unilateral glue ear in an adult (particularly of Asian or African origin) must prompt nasopharyngoscopy to exclude NPC.
Trotter's triad (classic NPC presentation): (1) unilateral conductive deafness (Eustachian tube obstruction); (2) unilateral palatal paraesthesia or anaesthesia (CN V2/V3 involvement at the foramen lacerum or skull base); (3) immobility of the ipsilateral soft palate (CN X or direct palatal muscle invasion). Trotter's triad is a late presentation indicating extensive skull base involvement.
Cranial nerve palsies in advanced NPC: CN VI (abducens — diplopia from cavernous sinus involvement) is the most commonly affected cranial nerve in NPC. Other cranial nerves (CN III, IV, V, IX, X, XII) may be involved as the tumour grows along the skull base.
Pathology and Aetiology of Sinonasal and Nasopharyngeal Tumours
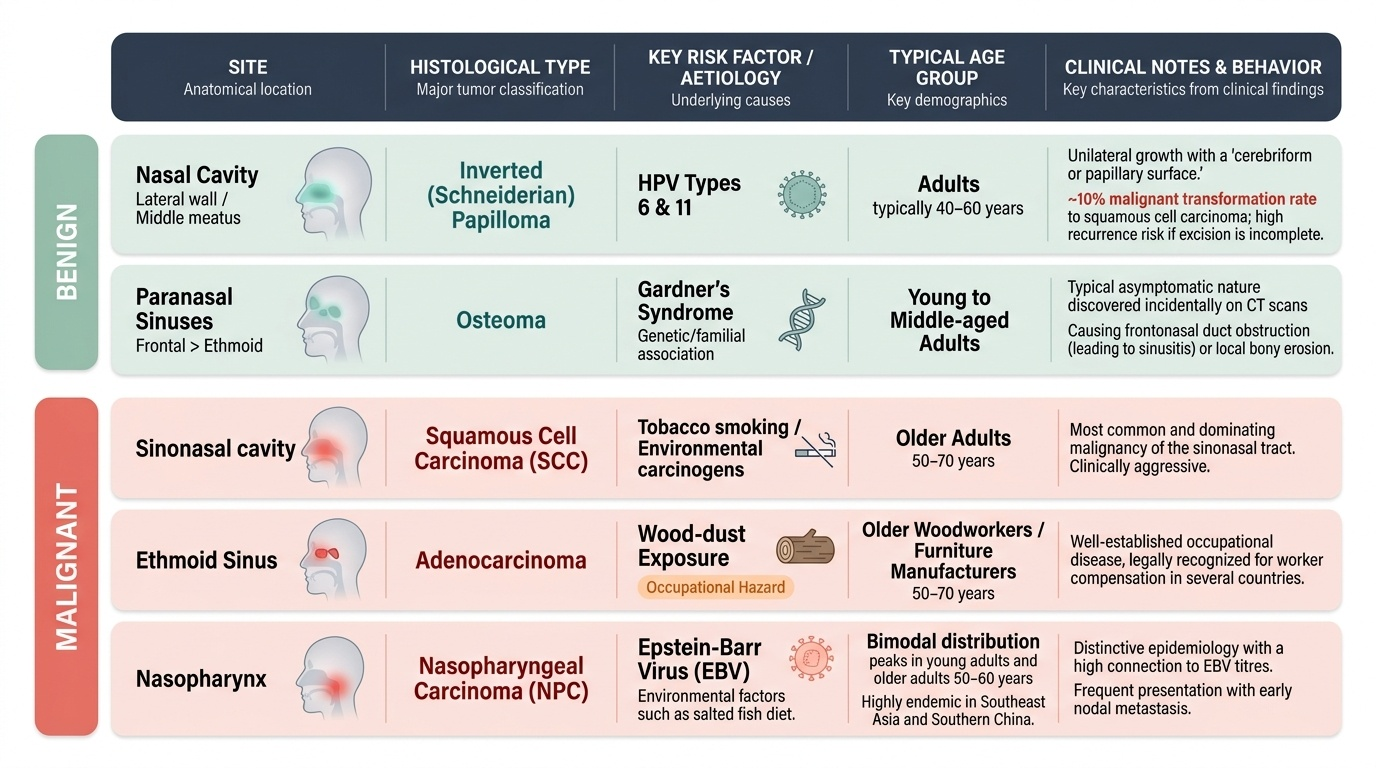
The histological diversity of sinonasal and nasopharyngeal tumours is broader than almost any other site in the body, reflecting the range of cell types present in the nasal mucosa, seromucinous glands, olfactory epithelium, bone, cartilage, and lymphoid tissue. Understanding the histological types and their specific risk factors guides both the diagnostic workup and the management strategy. For practical clinical purposes, the two most important categories are: (a) the benign tumours, of which inverted papilloma is the most significant because of its malignant transformation potential and high recurrence rate after incomplete excision; and (b) the malignant tumours, of which squamous cell carcinoma dominates the sinonasal group and nasopharyngeal carcinoma (with its distinctive EBV-associated and occupation-of-origin epidemiology) dominates the nasopharyngeal group. The occupational history is particularly important in sinonasal malignancy — ethmoid adenocarcinoma has a well-established causal link to wood-dust exposure that qualifies it as a prescribed occupational disease in several countries, meaning workers exposed to hardwood dust in furniture manufacturing may be entitled to compensation if they develop this tumour.
Provided image
Benign tumours of the nasal cavity:
- Inverted (Schneiderian) papilloma: the most clinically important benign nasal tumour. Arises from the lateral nasal wall (most commonly from the middle meatus), is unilateral, and has a characteristic cerebriform or papillary surface on endoscopy. HPV types 6 and 11 are implicated in its pathogenesis. It is locally aggressive and has a malignant transformation rate of approximately 10% (to squamous cell carcinoma). Complete surgical excision with an adequate margin is mandatory; incomplete excision causes near-certain recurrence. Endoscopic excision has largely replaced the older lateral rhinotomy approach in experienced hands.
- Osteoma: benign bony tumour arising most commonly in the frontal sinus (less commonly ethmoid); typically asymptomatic, found incidentally on CT. Large osteomas may obstruct the frontonasal duct, causing sinusitis, or erode into the orbit or cranial fossa. Gardner's syndrome should be excluded when multiple osteomas are found (Gardner's syndrome = familial adenomatous polyposis + multiple osteomas + epidermoid cysts).
- Haemangioma: vascular tumour of the nasal septum or lateral nasal wall; presents with episodic epistaxis; appears as a reddish, lobulated sessile mass on rhinoscopy. Can be excised endoscopically.
Malignant tumours of the nasal cavity and paranasal sinuses:
- Squamous cell carcinoma (SCC): the commonest malignant tumour of the nasal cavity and paranasal sinuses (~80% of sinonasal malignancies). Most commonly arises in the maxillary sinus. Risk factors include tobacco smoking, nickel refining, woodworking, leather-tanning, and textile dust exposure. Presents late, often with cheek swelling, tooth loosening, or orbital invasion.
- Adenocarcinoma: arises most commonly in the ethmoid sinuses, and has a well-established occupational aetiology — wood dust exposure (hardwoods: oak, beech, teak; furniture and cabinet-making industries). IARC classifies wood dust as a Group 1 (definite) human carcinogen for sino-nasal adenocarcinoma. This is one of the few occupationally-caused head and neck cancers, and an occupational history must be taken in any patient with ethmoid adenocarcinoma.
- Olfactory neuroblastoma (esthesioneuroblastoma): a rare neuroectodermal tumour arising from the olfactory epithelium in the roof of the nasal cavity (cribriform plate area). Presents with anosmia, nasal obstruction, and epistaxis. Can extend intracranially through the cribriform plate. Bimodal age distribution (11–20 and 50–60 years). Treated with surgery + radiotherapy.
- Sinonasal undifferentiated carcinoma (SNUC): highly aggressive, rapidly growing undifferentiated carcinoma; poor prognosis; treated with combined modality therapy.
- Mucosal melanoma: rare; arises from melanocytes in the nasal mucosa; characteristically dark-pigmented mass; high rate of local recurrence and metastasis.
Malignant tumours of the nasopharynx — NPC WHO classification:
Nasopharyngeal carcinoma is classified by the WHO into three types based on histology:
- Type I — Keratinising squamous cell carcinoma: similar to conventional SCC elsewhere in the head and neck; less strongly EBV-associated; less radiosensitive; seen more in Western populations.
- Type II — Non-keratinising carcinoma: moderately radiosensitive; intermediate EBV association.
- Type III — Undifferentiated carcinoma (lymphoepithelioma): the most common type in endemic areas (Southeast Asia, Southern China, North Africa, India). Strongly EBV-associated; EBV viral capsid antigen IgA (VCA-IgA) is elevated in serum and is used as a screening and diagnostic marker. Highly radiosensitive — this is why NPC (Types II and III) is primarily treated with radiotherapy (and concurrent chemotherapy in Stage II and above) rather than surgery.
SELF-CHECK
A 45-year-old furniture factory worker presents with progressive left-sided nasal obstruction and blood-stained nasal discharge for 3 months. CT shows an opacified left ethmoid sinus with bony erosion. Nasal endoscopy reveals an irregular mass in the left ethmoid region. The histology is most likely to show:
A. Squamous cell carcinoma — the most common histological type of all sinonasal malignancies
B. Adenocarcinoma — strongly associated with wood-dust exposure, particularly in the ethmoid sinus
C. Olfactory neuroblastoma — arises from the olfactory epithelium in the cribriform plate region
D. Mucosal melanoma — the ethmoid sinus is the most common site for nasal melanoma
Reveal Answer
Answer: B. Adenocarcinoma — strongly associated with wood-dust exposure, particularly in the ethmoid sinus
Ethmoid sinus adenocarcinoma has a well-established occupational association with wood-dust exposure (hardwoods — oak, beech, teak; furniture and cabinet-making industries). IARC classifies wood dust as a Group 1 (definite) carcinogen for sinonasal adenocarcinoma. While SCC is the most common sinonasal malignancy overall (~80%), when the site is the ethmoid and there is occupational wood-dust exposure, adenocarcinoma is the correct specific answer. Olfactory neuroblastoma arises from the cribriform plate/nasal roof, not the ethmoid sinuses specifically. Mucosal melanoma is rare and not specifically occupationally associated.
Investigations for Nasal and Nasopharyngeal Tumours
The investigation of sinonasal and nasopharyngeal tumours serves three purposes: confirming the diagnosis, staging the extent of disease, and planning treatment. The choice and sequence of investigations must be guided by the clinical context — particularly the critical question of whether biopsy is safe or whether there is any possibility that the mass is a JNA (in which case biopsy is contraindicated until imaging confirms it is not).
Nasal endoscopy: Rigid nasal endoscopy (0° and 30°) provides direct visualisation of the nasal cavity, middle and superior meatus, sphenoethmoidal recess, and posterior choana. It identifies the site of origin of a mass, its surface characteristics (smooth vs irregular, pedunculated vs sessile), and its vascularity. For most nasal masses in adults, endoscopy-guided biopsy is performed to obtain a tissue diagnosis. The exception is a suspected JNA in an adolescent male — in that case, imaging must be performed first.
CT of the paranasal sinuses and skull base: Provides bone detail, identifies the site and extent of the primary tumour, demonstrates bone erosion or destruction (a malignant feature), and maps sinus opacification. Contrast CT is used for vascular masses and when orbital or intracranial extension is suspected. For maxillary sinus SCC, CT assesses invasion of the orbital floor, pterygoid plates, posterior wall, and hard palate — all of which determine staging and operability.
MRI of the paranasal sinuses and skull base: Superior to CT for soft-tissue characterisation, distinguishing inflammatory secretions from tumour (retained secretions have different T2 signal from infiltrating carcinoma), and detecting perineural spread, dural involvement, and intracranial extension. MRI is complementary to CT in all malignant nasal tumours and is the preferred modality for NPC (skull base and cranial nerve assessment).
Nasopharyngoscopy: Flexible or rigid endoscopic examination of the nasopharynx is the gold standard for diagnosing NPC. The tumour typically arises in the fossa of Rosenmüller (the lateral recess of the nasopharynx posterior to the Eustachian tube opening) as an irregular, fleshy mass. Biopsies of nasopharyngeal tumours are taken under direct vision during nasopharyngoscopy.
EBV serology for NPC: Serum EBV viral capsid antigen IgA (VCA-IgA) is elevated in NPC, particularly in Types II and III. It is used as a diagnostic and screening marker in endemic regions and for post-treatment surveillance (rising titres suggest recurrence).
Biopsy: Essential for histological diagnosis of all malignant nasal and nasopharyngeal tumours. For nasal cavity and sinus masses, endoscopy-guided biopsy under local or general anaesthesia. For NPC, nasopharyngoscopic biopsy. For cervical lymphadenopathy from suspected NPC: fine-needle aspiration cytology (FNAC) from the node if nasopharyngoscopic biopsy is non-diagnostic (but nasopharyngoscopy first — a positive nasopharyngeal biopsy avoids the need for neck node FNAC).
PET-CT: Used for staging of advanced sinonasal and nasopharyngeal malignancies — identifies distant metastases (lung, bone, liver), occult nodal disease, and is used for treatment response assessment after chemoradiotherapy.