Page 10 of 17
EN4.45 | Diseases of Oesophagus — SDL Guide
Learning Objectives
- Describe the cardinal clinical features of oesophageal disease including dysphagia, odynophagia, regurgitation, heartburn, and alarm symptoms
- Explain the pathophysiology of GORD, Barrett's oesophagus, oesophageal carcinoma, and oesophageal atresia
- Choose appropriate investigations — barium swallow, upper GI endoscopy, manometry, pH monitoring, and CT — for oesophageal conditions
- Distinguish squamous cell carcinoma from adenocarcinoma of the oesophagus by location, risk factors, and prognosis
- Describe the principles of management of key oesophageal diseases: GORD, Barrett's oesophagus, oesophageal carcinoma, oesophageal foreign body, and oesophageal atresia
INSTRUCTIONS
Diseases of the oesophagus are clinically important because their presentations — dysphagia, heartburn, and regurgitation — are among the most frequent upper gastrointestinal complaints encountered in general practice, and because failure to recognise alarm features (progressive dysphagia, weight loss, odynophagia) delays the diagnosis of oesophageal carcinoma, which carries a poor prognosis when detected late. As a final-year student you must be able to construct a systematic differential for dysphagia, choose the appropriate first investigation, and outline the management principles for GORD-to-Barrett's progression, oesophageal carcinoma, and the emergency ENT scenario of an oesophageal foreign body in a child.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th ed., Chapter on Oesophagus (textbook)
- Hazarika P — Textbook of Ear, Nose and Throat Diseases, Chapter on Oesophagology (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Oesophagus section (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old male retired teacher presents to the ENT outpatient with a three-month history of progressive difficulty in swallowing. He initially noticed food 'sticking' at the lower chest level, first with bread and meat, but over the past four weeks he struggles even with semi-solid food. He has lost 7 kg in weight. He smokes one pack daily and drinks alcohol socially. On inquiry he also reports occasional regurgitation of undigested food and a persistent dry cough at night. His voice is unchanged. Examination of the oral cavity and oropharynx is normal; indirect laryngoscopy shows normal vocal cord movement. Where does the pathology lie, and what investigation will you request first to confirm your clinical suspicion before urgent referral?
WHY THIS MATTERS
The oesophagus serves as a conduit between the pharynx and the stomach, and diseases affecting it produce a distinctive symptom complex — dysphagia, heartburn, regurgitation, and odynophagia — that overlaps with both ENT and gastroenterological presentations. Oesophageal carcinoma is among the most lethal gastrointestinal malignancies because the oesophagus has no serosa and its rich submucosal lymphatics allow early nodal spread; the five-year survival for oesophageal cancer in India is below 20% largely because the majority present at an advanced stage. At the other end of the spectrum, gastro-oesophageal reflux disease (GORD) is one of the most prevalent conditions in clinical practice, and the GORD → Barrett's oesophagus → adenocarcinoma sequence is a paradigm for premalignant surveillance that you will apply throughout your career. For the ENT surgeon, the oesophageal foreign body — especially a coin or a button battery in a child — represents a time-critical emergency because an impacted button battery can cause full-thickness oesophageal perforation within hours through electrolytic and thermal injury. Understanding this disease group at the KH (Knowledge and Helping) level is the EN4.45 standard.
RECALL
Before engaging with oesophageal disease, consolidate three anatomical and physiological facts from your Phase I studies. First, recall that the oesophagus is approximately 25 cm long in adults, extending from the cricopharyngeus muscle (at the level of C6, marking the pharyngo-oesophageal junction) to the gastro-oesophageal junction (GOJ) at T10-T11. It has three natural anatomical narrowings — at the cricopharyngeus, at the level of the aortic arch and left main bronchus (T4-T5), and at the diaphragmatic hiatus (T10) — and these are the sites where swallowed foreign bodies most commonly impact. Second, the lower oesophageal sphincter (LOS) is a physiological rather than anatomical sphincter maintained by the intrinsic smooth muscle of the distal oesophagus and the extrinsic sling of the crural diaphragm; LOS relaxation is co-ordinated by vagal parasympathetic fibres through the myenteric plexus, and its failure to relax (as in achalasia) or its inappropriate relaxation (as in GORD) underpins two major disease categories. Third, the mucosal lining of the oesophagus is stratified squamous epithelium throughout, transitioning to columnar gastric epithelium at the Z-line (squamo-columnar junction) at the GOJ; when chronic acid reflux bathes the distal oesophageal mucosa, squamous cells undergo metaplastic change to intestinal columnar epithelium — this is Barrett's oesophagus, the premalignant state you will study in this SDL.
Clinical Presentation of Oesophageal Diseases
The clinical presentations of oesophageal disease, though superficially diverse, resolve into a small set of cardinal symptoms whose character, progression, and associated features direct both the differential diagnosis and the urgency of investigation. Recognising these patterns at the bedside is the first clinical skill required by EN4.45.
Dysphagia is difficulty in swallowing and is the most important oesophageal symptom. Its clinical utility depends on precise characterisation. The distinction between dysphagia to solids only (suggesting mechanical obstruction — carcinoma, stricture, foreign body, extrinsic compression) and dysphagia to both solids and liquids from the outset (suggesting a motility disorder — achalasia, diffuse oesophageal spasm) is perhaps the single most discriminating feature in the history. Progressive dysphagia — starting with solids, then progressing to soft food, then liquids — is the classic temporal profile of a slowly enlarging obstructing lesion such as carcinoma. Dysphagia that is intermittent and related to cold beverages or emotional stress suggests diffuse oesophageal spasm. Dysphagia associated with regurgitation of undigested food (food retained in the oesophagus, not mixed with acid) is characteristic of achalasia or Zenker's diverticulum, where there is no gastric secretion mixing.
Odynophagia — painful swallowing — occurs with oesophagitis (reflux, candidal, herpetic), foreign body impaction, and oesophageal perforation. Its presence alongside dysphagia in an immunocompromised patient (HIV, post-transplant, steroid-treated) should immediately raise candidal or viral (HSV, CMV) oesophagitis.
Heartburn (pyrosis) — a burning retrosternal sensation radiating upward, often worse after meals, when supine, or on bending — is the cardinal symptom of GORD. It may be associated with acid regurgitation (effortless return of sour-tasting fluid into the mouth), waterbrash (reflex hypersalivation), and belching. Chronic GORD may also present with ENT manifestations: chronic laryngopharyngeal reflux (LPR) causing hoarseness, chronic cough, throat-clearing, and posterior laryngeal oedema.
Regurgitation of undigested food (not sour, not acid-tasting) distinguishes oesophageal from gastric regurgitation and points to achalasia or a pharyngeal pouch.
Alarm features that demand urgent investigation: progressive dysphagia, significant unintentional weight loss (>5% body weight), odynophagia, haematemesis or melaena, a palpable cervical lymph node, and new voice change. Any of these alongside dysphagia obliges urgent upper GI endoscopy to exclude malignancy.
In neonates, oesophageal disease presents quite differently: oesophageal atresia classically manifests at birth as excessive salivation and frothy secretions from the mouth, episodes of choking and cyanosis with the first feed, respiratory distress from overflow aspiration, and the inability to pass a nasogastric tube beyond 8–10 cm from the nostril.
Pathophysiology of Key Oesophageal Conditions
Understanding the pathophysiological mechanism of each major oesophageal condition provides the logical framework for selecting investigations and planning management. The diseases relevant to EN4.45 cluster around four pathophysiological axes: mucosal injury from acid reflux, premalignant mucosal metaplasia, neoplastic transformation, and structural or embryological anomalies.
GORD and Reflux Oesophagitis: Normal gastro-oesophageal competence depends on the LOS maintaining a resting pressure of approximately 10–30 mmHg above intragastric pressure, aided by the crural diaphragm sling, the angle of His (the acute angle between the oesophagus and gastric fundus), and the intra-abdominal segment of the oesophagus. GORD occurs when this anti-reflux barrier is overcome — most commonly through transient lower oesophageal sphincter relaxations (TLOSRs), less commonly through a fixed hiatus hernia that displaces the GOJ above the diaphragm. Repeated exposure of the stratified squamous oesophageal mucosa to acid, pepsin, and bile salts causes mucosal injury — microscopically, basal cell hyperplasia and elongation of papillae — progressing to macroscopic erosive oesophagitis, ulceration, fibrosis, and eventually peptic stricture at the GOJ.
Barrett's Oesophagus: With chronic GORD, the oesophageal squamous epithelium undergoes intestinal metaplasia — replacement by specialised columnar epithelium with goblet cells (histologically identical to small intestinal epithelium). This is Barrett's oesophagus, defined endoscopically as displacement of the squamo-columnar junction (Z-line) more than 3 cm proximal to the GOJ, confirmed histologically by intestinal metaplasia with goblet cells. Barrett's epithelium carries an approximately 0.5% per year risk of progression to adenocarcinoma through the stepwise sequence: non-dysplastic metaplasia → low-grade dysplasia (LGD) → high-grade dysplasia (HGD) → invasive adenocarcinoma. This sequence is the rationale for endoscopic surveillance.
Carcinoma of the Oesophagus — SCC vs Adenocarcinoma: Squamous cell carcinoma (SCC) arises from the oesophageal stratified squamous epithelium and is located in the upper and middle thirds of the oesophagus. Its principal risk factors are tobacco, alcohol, hot beverages (particularly tea in Central Asia and South Africa), nutritional deficiencies, and predisposing lesions (achalasia, Plummer-Vinson syndrome). Adenocarcinoma arises in Barrett's metaplastic epithelium and is therefore located in the lower third and the gastro-oesophageal junction (GOJ); it is strongly associated with GORD, obesity, and white male sex. Macroscopically, both types appear as proliferative, ulcerative, or infiltrative lesions; early disease causes intraluminal narrowing, and advanced disease causes complete obstruction with proximal dilatation.
Oesophageal Foreign Body: Foreign bodies most commonly impact at the three natural narrowings of the oesophagus. In children, the commonest objects are coins (which orient in the coronal plane — appearing as a disc on AP chest X-ray, unlike tracheal coins which appear end-on on AP view), button batteries, and safety pins. In adults, dentures, meat bolus, fish or chicken bones, and dental crowns are common. A button battery impacting in the oesophagus is a surgical emergency: it generates an electrical current and localised alkali through electrolysis, causing full-thickness liquefactive necrosis and perforation within as little as 2–4 hours.
Oesophageal Atresia: This is a congenital anomaly resulting from failure of complete separation of the foregut into the trachea and oesophagus during the fourth to fifth weeks of intrauterine development. The most common type (Gross type C, ~85% of cases) consists of a blind-ending proximal oesophageal pouch with a fistula between the lower oesophagus and the trachea or carina (tracheo-oesophageal fistula, TOF). The lower segment TOF allows gastric air to enter the lungs (explaining the gaseous distension of the GI tract on X-ray) and gastric acid to reflux into the trachea. The 'H-type' fistula (Gross type E) presents with recurrent chest infections without frank feeding difficulty because the oesophagus is patent.
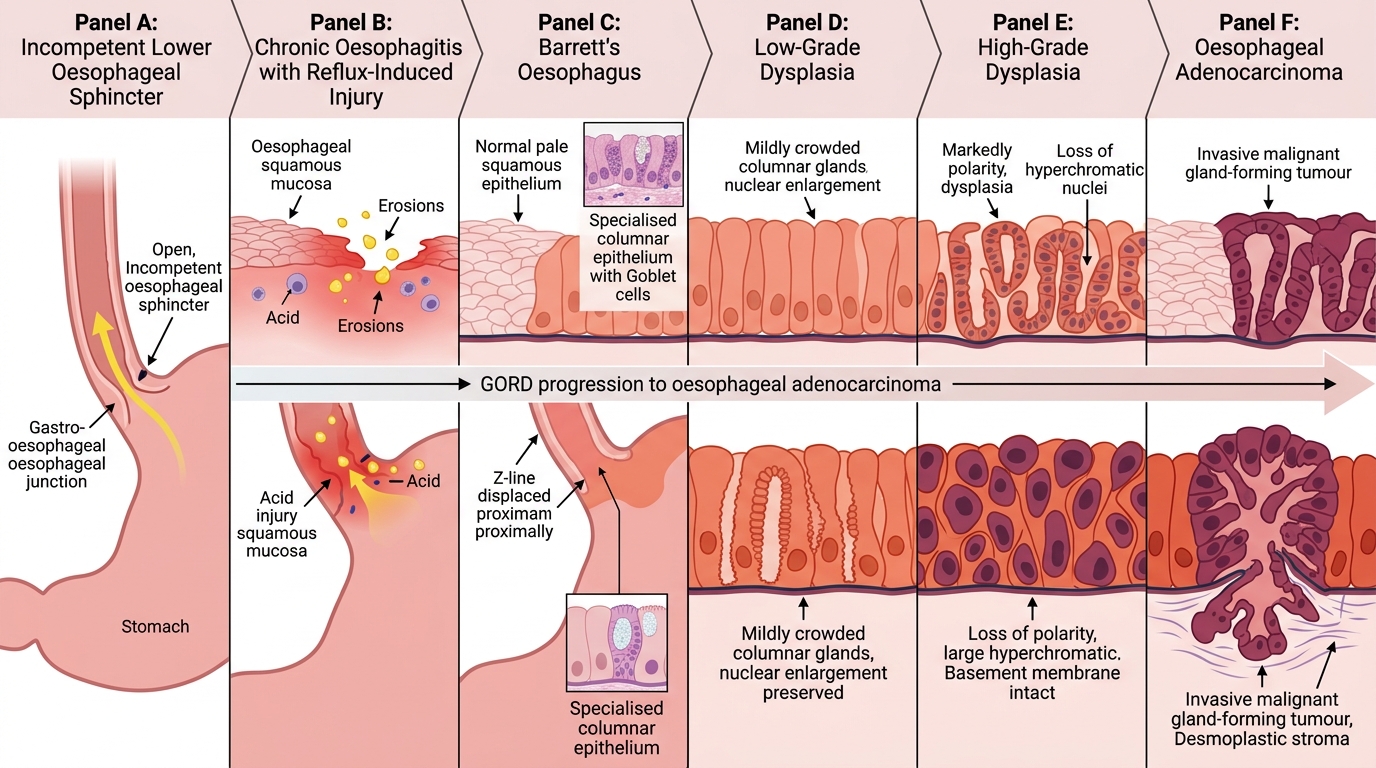
GORD to Barrett's Oesophagus to Adenocarcinoma
SELF-CHECK
A 48-year-old woman with a 10-year history of heartburn and acid regurgitation undergoes upper GI endoscopy, which shows displacement of the Z-line 4 cm above the GOJ. Biopsy confirms specialised columnar epithelium with goblet cells. This finding represents:
A. Reflux oesophagitis — manage with dose escalation of PPI
B. Barrett's oesophagus — enrol in endoscopic surveillance programme
C. Adenocarcinoma in situ — immediate oesophagectomy
D. Eosinophilic oesophagitis — dietary elimination therapy
Reveal Answer
Answer: B. Barrett's oesophagus — enrol in endoscopic surveillance programme
The combination of chronic GORD symptoms, Z-line displaced >3 cm proximal to GOJ, and histological confirmation of intestinal metaplasia (specialised columnar epithelium with goblet cells) defines Barrett's oesophagus. It is a premalignant condition, not carcinoma. The correct management is enrolment in an endoscopic surveillance programme (non-dysplastic Barrett's: surveillance endoscopy every 3–5 years; low-grade dysplasia: 6-monthly; high-grade dysplasia: endoscopic ablation/mucosal resection). Prescribing PPI alone without surveillance fails to address the malignant potential. Eosinophilic oesophagitis would show eosinophil infiltration on biopsy, not columnar metaplasia.
Investigation of Oesophageal Diseases
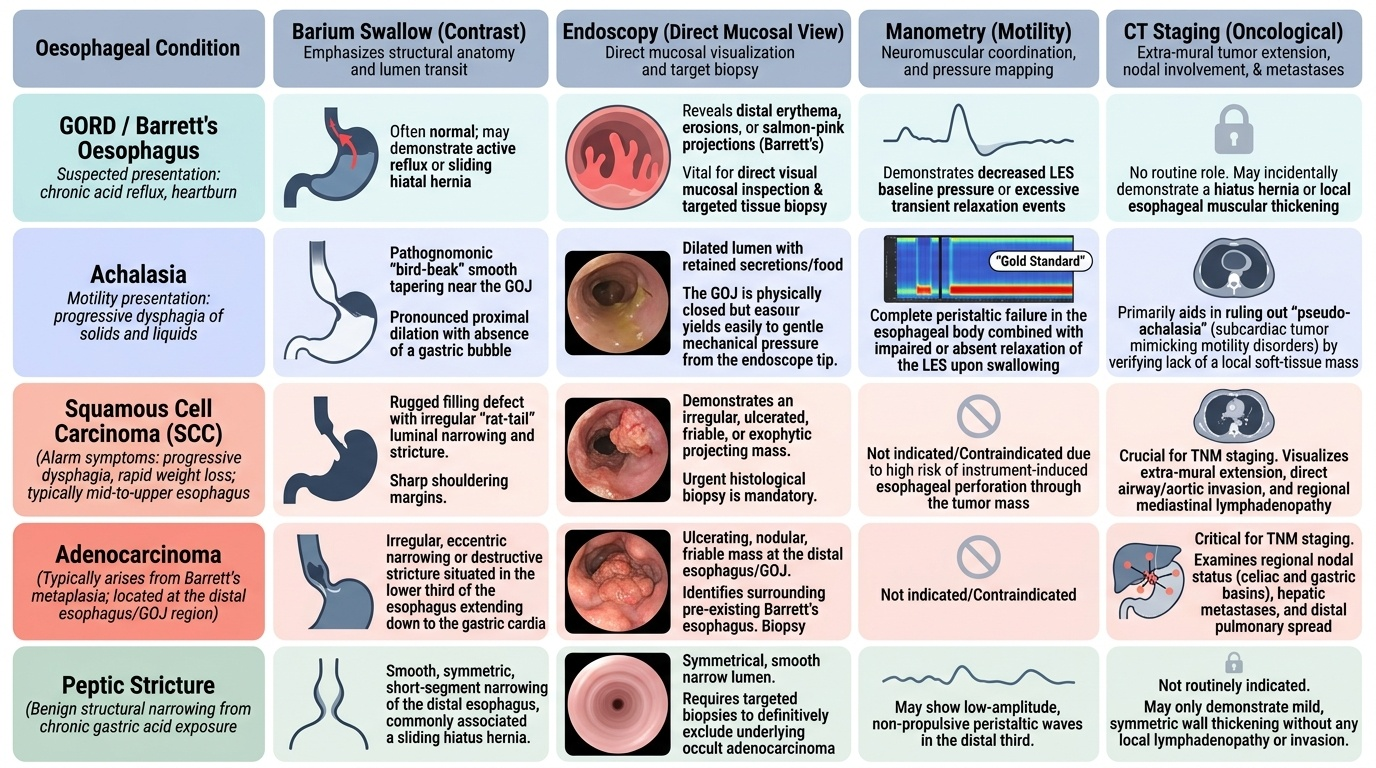
The choice of first investigation for an oesophageal complaint is determined by the clinical presentation, the urgency, and the specific information needed. No single investigation answers all questions — barium swallow defines anatomy, endoscopy provides direct mucosal visualisation and biopsy, manometry measures oesophageal function, and CT provides staging information. A practical principle guides the selection: start with the investigation most likely to establish the diagnosis at the least risk to the patient. In progressive dysphagia with alarm features, barium swallow (or direct upper GI endoscopy if the index of suspicion for carcinoma is high) is the first step; in suspected GORD, a therapeutic PPI trial and pH monitoring are more informative than anatomy-based investigations; in suspected motility disorders such as achalasia, manometry is the definitive test once structural obstruction has been excluded. Understanding the unique contribution of each modality — and its limitations — prevents the common error of relying on a single investigation to exclude or confirm a diagnosis that requires confirmation by a different test.
Provided image
Barium Swallow (Contrast Oesophagram): Barium swallow is a safe, widely available, and often the most informative first investigation for structural and motility oesophageal disease in a resource-limited setting. It outlines the oesophageal lumen, identifies filling defects (carcinoma, stricture), shows hold-ups of barium (foreign body, achalasia), and demonstrates the motility pattern. Characteristic appearances include:
- Carcinoma: irregular 'rat-tail' or 'apple-core' filling defect; shouldering of the margins at the obstruction; proximal dilatation.
- Achalasia: smooth tapering ('bird-beak' or 'rat-tail' appearance) at the GOJ with a greatly dilated proximal oesophagus; absence of the gastric air bubble on upright film.
- Pharyngeal pouch (Zenker's diverticulum): barium fills the posterior neck pouch behind the oesophagus; the pouch displaces the oesophagus anteriorly.
- Oesophageal web (Plummer-Vinson): thin shelf-like filling defect in the post-cricoid region.
Note: Barium swallow is contraindicated in suspected oesophageal perforation; use water-soluble contrast (Gastrografin) instead, as barium in the mediastinum causes severe granulomatous mediastinitis.
Upper GI Endoscopy (Oesophago-Gastro-Duodenoscopy, OGD): This is the definitive investigation for mucosal disease. It allows direct visualisation of the oesophageal mucosa, the Z-line, and the GOJ; permits biopsy of suspicious areas (essential for diagnosing Barrett's, carcinoma, and oesophagitis); and enables therapeutic intervention (dilatation of strictures, foreign body removal, haemostasis, stenting). Rigid oesophagoscopy (under general anaesthesia) is used primarily for foreign body removal and in some centres for post-cricoid lesions. Flexible endoscopy (conscious sedation) is the routine diagnostic and therapeutic modality.
Oesophageal Manometry: Manometry records intraluminal pressure patterns during swallowing using a catheter with multiple sensors. It is the gold standard for diagnosing motility disorders. In achalasia, manometry shows: absence of oesophageal peristalsis (aperistalsis); incomplete or absent LOS relaxation; elevated LOS resting pressure. In diffuse oesophageal spasm, it shows simultaneous non-propagated high-amplitude contractions in the distal oesophagus. Manometry is also used pre-operatively before fundoplication to assess oesophageal body function.
24-Hour Ambulatory pH Monitoring: This records the oesophageal pH continuously over 24 hours via a pH probe positioned 5 cm above the LOS. It quantifies the total acid exposure time and correlates symptoms with pH events. Pathological acid reflux is defined as pH <4 for >4% of the total monitoring period (DeMeester score). It is the gold standard for confirming GORD when the diagnosis is uncertain after empirical PPI therapy or when surgical treatment (fundoplication) is being considered.
CT Thorax/Abdomen: CT is used primarily for staging oesophageal carcinoma — assessing tumour length (T stage), regional lymphadenopathy (N stage), and distant metastases to liver, lungs, and peritoneum (M stage). Endoscopic ultrasound (EUS), where available, provides the most accurate T and N staging for surgical planning.
Plain Radiograph: A plain AP chest X-ray identifies radio-opaque foreign bodies (coins: appear as a disc on AP chest X-ray in the coronal plane in oesophagus, versus end-on in the trachea). An erect chest X-ray in suspected perforation may reveal pneumomediastinum or pleural effusion.