Page 2 of 17
EN4.37 | Dysphagia — SDL Guide (Part 2)
Examination and Investigation of Dysphagia
The clinical examination of a patient with dysphagia is directed at three goals: identifying the anatomical site of the problem, characterising the nature of the lesion (structural vs motility, benign vs malignant), and detecting systemic signs of malignancy or nutritional compromise. A thorough examination often confirms or modifies the diagnostic impression formed from the history before a single investigation is ordered. In a busy outpatient setting, the combination of a structured history and a targeted clinical examination — taking no more than 10–15 minutes — should allow the clinician to order the correct first investigation with confidence rather than ordering a 'shotgun' panel. The examination sequence follows a logical anatomical hierarchy: general assessment, then neck, then oral cavity and oropharynx, then laryngoscopy, followed by a directed investigation plan based on the working diagnosis reached from the history.
Clinical examination:
- General: nutritional status (weight loss, temporal wasting, pallor from anaemia), dehydration, lymphadenopathy.
- Neck: hard fixed non-tender lymph nodes (malignancy); soft compressible swelling in the left posterior triangle with a gurgling sound (Boyce's sign — pharyngeal pouch); thyroid enlargement (retrosternal goitre); tracheal deviation.
- Oral cavity and oropharynx: lesions of the tongue, tonsil, soft palate, or posterior pharyngeal wall; palatal palsy (nasal speech, regurgitation); examine the cranial nerves IX, X, and XII.
- Laryngoscopy (indirect or fibreoptic): pooling of saliva in the pyriform fossae (obstruction or poor clearance), mucosal lesion in the hypopharynx or postcricoid region, vocal cord palsy (indicating recurrent laryngeal nerve involvement — a feature of hypopharyngeal or oesophageal malignancy or mediastinal disease).
Investigations — logical sequence:
- Blood tests: Full blood count (anaemia in malignancy or Plummer-Vinson), iron studies, serum albumin (nutritional status).
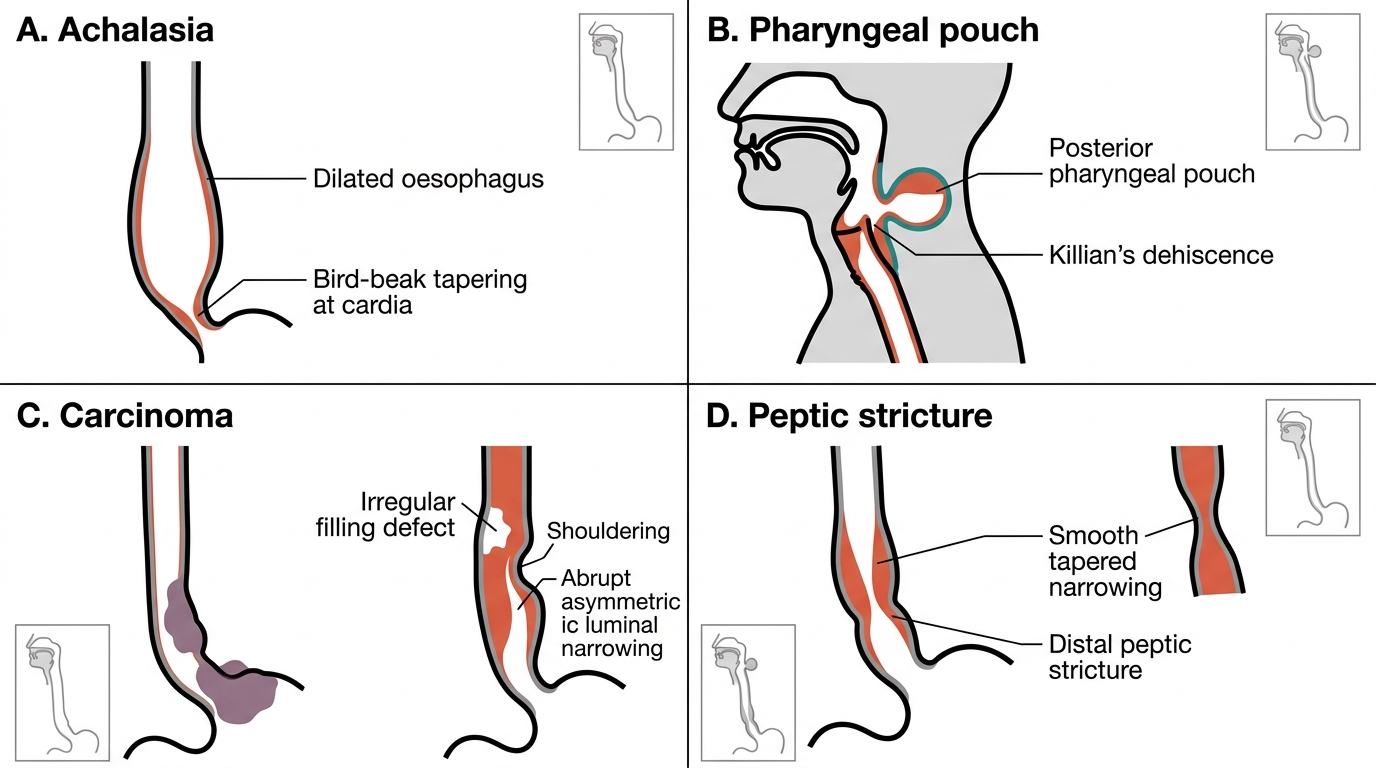
- Barium swallow (fluoroscopy): A dynamic study — the patient swallows barium contrast while fluoroscopic images are taken. It shows the site and nature of the obstruction, pouch morphology, and motility pattern. Safe, non-invasive, overview of the entire mechanism. Key findings: bird-beak tapering at the cardia (achalasia); corkscrew pattern (DES); irregular filling defect with shouldering (carcinoma); smooth tapered narrowing (peptic stricture); posterior outpouching at Killian's dehiscence (pharyngeal pouch); thin shelf-like defect on the anterior wall of the postcricoid region (web in Plummer-Vinson); dilated oesophagus with air-fluid level (longstanding achalasia).
- Upper GI endoscopy (oesophagoscopy): The definitive investigation for any intraluminal oesophageal lesion. Allows direct visualisation, biopsy, and therapeutic intervention (dilatation, stent insertion, foreign body removal). Rigid oesophagoscopy (under general anaesthesia) is used for foreign body removal and in hypopharyngeal carcinoma; flexible UGI endoscopy is the standard outpatient diagnostic tool.
- Oesophageal manometry: The definitive test for motility disorders — measures resting and swallowing-induced pressures throughout the oesophagus and at the LES. Mandatory for diagnosis of achalasia (elevated LES resting pressure + absent LES relaxation + absent peristalsis) and DES.
- CT scan of neck, thorax, and abdomen: Used for staging of malignancy after histological confirmation — assesses local tumour extent, regional lymphadenopathy, and distant metastases. Also identifies extrinsic compressive causes.
- Video-fluoroscopic swallowing study (VFSS): A specialised dynamic study used to assess pharyngeal phase dysphagia and aspiration risk in neurological patients.
Barium Swallow Findings in Dysphagia
SELF-CHECK
A 35-year-old woman presents with a 2-year history of difficulty swallowing both solids and liquids, intermittent regurgitation of undigested food, and two episodes of aspiration pneumonia. Barium swallow shows a dilated oesophagus with smooth tapering at the cardia. The definitive diagnostic test to confirm the diagnosis is:
A. Upper GI endoscopy with biopsy
B. CT scan of the chest
C. Oesophageal manometry
D. 24-hour pH monitoring
Reveal Answer
Answer: C. Oesophageal manometry
The clinical picture — dysphagia to both solids AND liquids, regurgitation of undigested food, aspiration pneumonia, and a bird-beak deformity on barium swallow — is classic for achalasia. Oesophageal manometry is the definitive diagnostic test: it demonstrates elevated resting LES pressure, absent LES relaxation on swallowing, and absent oesophageal peristalsis. Endoscopy is performed to exclude pseudoachalasia (a malignancy at the cardia mimicking achalasia) but does not confirm motility. CT and pH monitoring are not diagnostic for achalasia.
Diagnosis and Differential Diagnosis of Dysphagia
Reaching a diagnostic impression in dysphagia relies on a clinical reasoning framework built on four history variables: (1) the solid vs liquid distinction, (2) the pattern of progression, (3) the patient's age and risk factors, and (4) associated features. Together, these four axes typically point to the correct diagnostic category before any investigation is requested. The ability to synthesise these axes into a working diagnosis — rather than ordering investigations in the dark — is the hallmark of competent clinical reasoning at the SH level. A student who can correctly apply this framework in an OSCE will not miss a malignancy or misclassify a motility disorder as a mechanical obstruction.
Axis 1 — Solid only vs solid + liquid from the outset:
Solid-only dysphagia = mechanical obstruction. Both-solid-and-liquid from onset = motility disorder. A patient who initially had solid dysphagia and then developed liquid dysphagia is most likely a mechanical lesion that is growing (e.g., carcinoma).
Axis 2 — Progression:
Rapidly progressive (weeks to a few months) = malignancy, rapidly expanding benign lesion (abscess), acute foreign body. Slowly progressive over months to years = achalasia, peptic stricture, pharyngeal pouch. Intermittent, episodic = Schatzki ring (complete obstruction of a large bolus followed by relief), diffuse oesophageal spasm (intermittent chest pain + dysphagia).
Axis 3 — Age and risk profile:
Over 40 + progressive solid dysphagia + weight loss = malignancy until proven otherwise. Under 30 + both solid/liquid dysphagia + regurgitation of undigested food = achalasia. Middle-aged woman + anaemia + solid dysphagia = Plummer-Vinson syndrome. Elderly patient + regurgitation of undigested food + soft neck swelling = pharyngeal pouch.
Axis 4 — Associated features:
Hoarseness = recurrent laryngeal nerve involvement (hypopharyngeal or oesophageal malignancy). Referred otalgia = primary tumour in the hypopharynx (via Arnold's branch of X nerve). Nasal regurgitation of liquids = palatal paralysis (neurological). Chest pain accompanying dysphagia = diffuse oesophageal spasm. Iron-deficiency anaemia in a middle-aged woman = Plummer-Vinson syndrome.
Alarm features mandating urgent investigation (within 2 weeks):
- Progressive solid-food dysphagia in a patient over 40
- Dysphagia with significant unintentional weight loss
- New dysphagia with odynophagia (suggests carcinoma with mucosal invasion or ulceration)
- Dysphagia with haematemesis or malaena
- Hoarseness accompanying dysphagia (nerve invasion by malignancy)
| Discriminating feature | Mechanical obstruction | Motility disorder |
|---|---|---|
| Solid vs liquid | Solids first; liquids later | Both from onset |
| Progression | Usually progressive | Variable (achalasia = progressive; DES = intermittent) |
| Regurgitation type | Digested content (GORD) or recent meal | Undigested food (achalasia, pouch) |
| Weight loss | Common in malignancy | Moderate in achalasia |
| Pain | Odynophagia if ulcerated | Chest pain in DES/achalasia |
| Age/risk | >40, tobacco/alcohol for carcinoma | Any age; achalasia peaks 20–40 yr |
CLINICAL PEARL
The single most important clinical distinction in dysphagia is: solid-only dysphagia = mechanical obstruction; solid-AND-liquid dysphagia from the start = motility disorder. Committing this to memory prevents the most dangerous diagnostic error — missing a carcinoma by attributing progressive solid dysphagia to anxiety or oesophageal spasm. A patient over 40 years old with three months of worsening solid-food dysphagia and weight loss should be treated as having oesophageal malignancy until endoscopy and biopsy prove otherwise.
Principles of Management of Dysphagia
Management of dysphagia is diagnosis-specific, and no single treatment applies across the spectrum of causes. Before any definitive intervention is undertaken, the diagnosis must be established with histological or manometric confirmation, as the consequences of treating the wrong condition are serious — for example, attempting balloon dilatation for a suspected motility disorder that turns out to be a malignant stricture risks perforation of a friable tumour wall. The overarching management principles are: (1) establish the diagnosis before definitive treatment; (2) ensure adequate nutrition and airway safety throughout the diagnostic period; (3) treat the underlying cause with the least invasive effective modality; and (4) involve a multidisciplinary team (ENT, gastroenterology, surgery, speech-language therapy, dietetics, oncology as indicated). These principles apply whether the patient is seen at a primary health centre or a tertiary teaching hospital.
General supportive measures (apply across all causes):
- Nutritional support: modify food consistency (soft, pureed, thickened liquids) to maintain oral intake while investigations proceed. Nasogastric tube feeding or percutaneous endoscopic gastrostomy (PEG) if oral intake is inadequate or unsafe.
- Speech and language therapy: assess swallowing safety, prevent aspiration, advise on posture and texture modifications.
Specific management by condition:
1. Carcinoma of the hypopharynx or oesophagus:
- Early (localised) disease: total pharyngolaryngectomy ± partial oesophagectomy for hypopharyngeal carcinoma; oesophagectomy (Ivor-Lewis, transhiatal, or total oesophagectomy with gastric pull-up) for oesophageal carcinoma. Concurrent chemoradiotherapy is an organ-preservation alternative for some hypopharyngeal tumours.
- Palliative options: self-expanding metallic stent (SEMS) insertion to restore luminal patency for dysphagia palliation; endoscopic laser recanalisation; radiotherapy for symptom control; PEG for nutrition.
2. Achalasia:
- The aim is to reduce the LES pressure to allow food passage, since peristalsis cannot be restored.
- Endoscopic balloon dilatation (pneumatic dilatation): first-line treatment; a large-diameter balloon (3–4 cm) is inflated across the LES under fluoroscopic guidance. Effective in 60–85% of patients; risk of perforation ~1–3%.
- Heller's cardiomyotomy: surgical (laparoscopic or open) division of the LES circular muscle fibres, combined with a partial fundoplication (Dor or Toupet). Effective in ~85–90% of patients.
- Per-oral endoscopic myotomy (POEM): endoscopic division of the LES circular muscle via a submucosal tunnel; increasingly available in tertiary centres.
- Pharmacological (temporising only): sublingual nifedipine or botulinum toxin injection into the LES — temporary relief; reserved for patients unfit for dilatation or surgery.
3. Pharyngeal pouch (Zenker's diverticulum):
- Endoscopic stapling (modified Dohlman's procedure): the party wall between the pouch and oesophagus is divided using an endoscopic stapler or CO₂ laser — obliterates the pouch neck and divides the cricopharyngeus. Minimally invasive; preferred in elderly or unfit patients.
- External transcervical excision with cricopharyngeal myotomy: definitive treatment in fit patients with large pouches.
4. Peptic stricture:
- Endoscopic balloon dilatation combined with long-term PPI therapy to prevent recurrent stricture formation.
5. Plummer-Vinson syndrome:
- Iron supplementation (corrects anaemia; often causes web to regress spontaneously).
- If the web persists: endoscopic dilatation or disruption.
- Annual surveillance for postcricoid carcinoma (premalignant condition).
6. Schatzki ring:
- Endoscopic balloon dilatation or bougienage; often only one session required.
7. Oesophageal foreign body:
- Rigid oesophagoscopy under general anaesthesia — method of choice for sharp or impacted objects. Never attempt blind finger removal.
SELF-CHECK
A 55-year-old woman with Plummer-Vinson syndrome presents with persistent solid-food dysphagia despite six months of oral iron supplementation. Endoscopy reveals a persistent postcricoid web. She has no features of malignancy. The appropriate next step is:
A. Total pharyngolaryngectomy
B. Endoscopic dilatation or disruption of the web
C. Long-term PPI therapy alone
D. Achalasia balloon dilatation
Reveal Answer
Answer: B. Endoscopic dilatation or disruption of the web
In Plummer-Vinson syndrome, iron supplementation is the first-line treatment and often causes the postcricoid web to regress. When the web persists despite adequate iron replacement and continues to cause dysphagia, endoscopic dilatation or disruption (web rupture) is the appropriate next intervention. Total pharyngolaryngectomy would be appropriate for postcricoid carcinoma, not a benign web. PPI therapy targets GORD-related strictures. Balloon dilatation for achalasia targets the lower oesophageal sphincter in a motility disorder — not relevant here.
Self-Assessment: Dysphagia
Test your understanding of this module by working through the following questions before checking the answers. These questions reflect the competency level required at EN4.37 (SH) — you should be able to answer them from the history, examination, and investigation principles covered in this SDL. For each question, first commit to an answer and a brief justification, then read the explanation.
Question 1. A 48-year-old woman presents with a 4-month history of solid-food dysphagia and pallor. Haemoglobin is 7.4 g/dL with a hypochromic microcytic picture. Barium swallow in the lateral view shows a thin shelf-like filling defect on the anterior wall of the postcricoid region. What is the diagnosis, and what are the two essential components of management?
Answer: Plummer-Vinson syndrome (postcricoid web + iron-deficiency anaemia + dysphagia in a middle-aged woman). Management: (1) iron supplementation — corrects the anaemia and often causes the web to regress; (2) endoscopic dilatation or web disruption if the web persists despite iron replacement. Lifelong annual endoscopic surveillance for postcricoid carcinoma is mandatory because the web is premalignant.
Question 2. A 29-year-old man presents with a 3-year history of dysphagia to both solids and liquids, regurgitation of undigested food at night, and two episodes of aspiration pneumonia. Barium swallow shows a markedly dilated oesophagus with smooth, tapered narrowing at the gastro-oesophageal junction. What is the diagnosis, what investigation confirms it, and what is the first-line treatment?
Answer: Achalasia. The definitive investigation is oesophageal manometry (elevated resting LES pressure + absent LES relaxation on swallowing + absent peristalsis throughout the oesophageal body). First-line treatment is endoscopic pneumatic balloon dilatation (or Heller's cardiomyotomy in younger fit patients, given lower long-term recurrence rate). Upper GI endoscopy should also be performed to exclude pseudoachalasia from a cardia tumour.
Question 3. An elderly gentleman presents with progressive dysphagia, regurgitation of undigested food, halitosis, and a soft swelling in the left posterior triangle of the neck that makes a gurgling sound when palpated. What is the diagnosis? Which investigation is the best initial imaging test, and what is the ENT sign found on neck palpation?
Answer: Pharyngeal pouch (Zenker's diverticulum). The best initial imaging test is a barium swallow (shows posterior outpouching at Killian's dehiscence below the cricopharyngeus). The ENT sign is Boyce's sign — a soft, compressible, posterior triangle swelling that gurgles and reduces on gentle pressure (as the contents of the pouch empty).