Page 8 of 17
EN4.39 | Tonsillectomy and Adenoidectomy — SDL Guide (Part 2)
Interpretation of Post-operative Findings and Complications
The post-operative period after tonsillectomy carries several characteristic complications that the clinician must be able to recognise and respond to promptly. Among these, haemorrhage is the most feared and the most important to understand — both in terms of its timing and its immediate management. Every patient and parent must be counselled about the risk of secondary haemorrhage before discharge, because failure to return promptly when it occurs can be fatal in rare cases where blood loss is significant or where a blood clot obstructs the airway. Beyond haemorrhage, a small number of patients develop complications related to the adenoidectomy component (VPI, Grisel syndrome) or to the anaesthetic itself; a complete understanding of this spectrum is what makes the post-operative assessment and discharge counselling accurate and safe.
Provided image
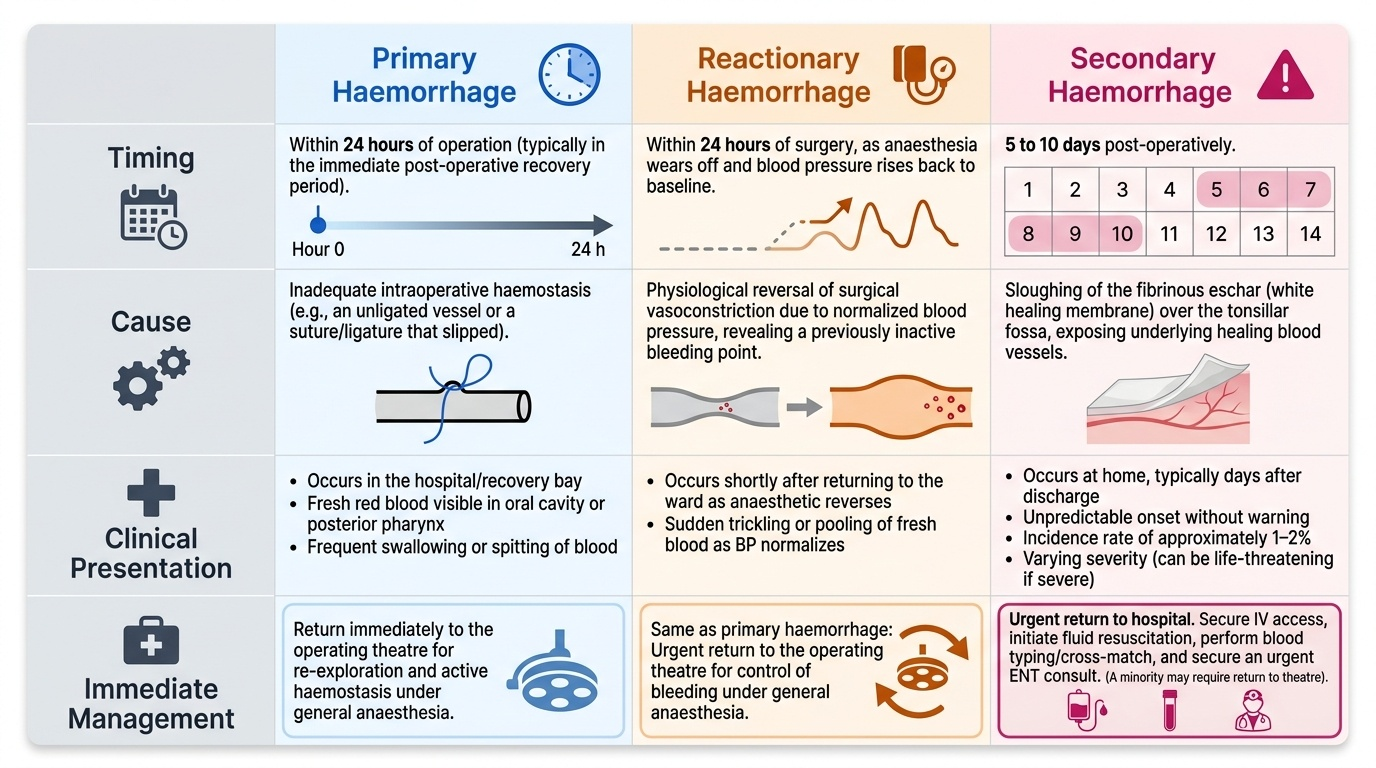
Post-operative haemorrhage — three types:
- Primary haemorrhage: bleeding that occurs within 24 hours of the operation, most often in the immediate post-operative recovery period. Cause: inadequate intraoperative haemostasis — a vessel that was not ligated, or a ligature that slipped. Management: return to theatre for re-exploration and haemostasis under general anaesthesia.
- Reactionary haemorrhage: bleeding within the first 24 hours, typically occurring when the patient's blood pressure rises toward normal as the vasoconstriction from anaesthesia reverses. Cause: physiological reversal of surgical vasoconstriction revealing a bleeding point that appeared controlled intraoperatively. Management: as for primary haemorrhage — return to theatre.
- Secondary haemorrhage: bleeding occurring 5–10 days after surgery, caused by sloughing of the fibrinous eschar (white membrane) that forms over the tonsillar fossa as part of normal healing. When this eschar separates, the healing blood vessels beneath may bleed. Secondary haemorrhage is the most clinically significant complication for patients discharged home — it is entirely unpredictable, can occur without warning, and the patient may be at home alone. Incidence: approximately 1–2%. Management: all secondary haemorrhage requires urgent return to hospital. Most episodes stop spontaneously, but some require return to theatre. IV access, fluid resuscitation, blood group and cross-match, and ENT review are mandatory. NEVER advise a patient to 'wait and see' with secondary haemorrhage.
Other complications:
- Velopharyngeal insufficiency (VPI): inadequate closure of the velopharyngeal sphincter after adenoidectomy, resulting in hypernasal speech and nasal regurgitation of liquids. Occurs when the adenoid was contributing to velopharyngeal closure in a patient with a short or cleft palate. This is why adenoidectomy is contraindicated in patients with cleft palate or submucous cleft.
- Grisel syndrome (atlantoaxial subluxation): rare but serious — subluxation of the atlantoaxial joint following adenoidectomy, attributed to laxity of the atlantoaxial ligaments secondary to adjacent inflammation and hyperaemia. Presents with painful torticollis in the post-operative period. Requires urgent imaging and orthopaedic/neurosurgical consultation.
- Post-operative pain: significant, particularly on day 3–5 as the eschar forms; managed with regular paracetamol ± ibuprofen. Swallowing is painful but the patient must be encouraged to maintain oral intake and hydration, as dehydration increases the risk of secondary haemorrhage.
- Throat infection: secondary infection of the tonsillar fossa is not uncommon; treated with antibiotics if systemic features develop.
Applied Practice — Tonsillectomy and Adenoidectomy Decision-Making
The applied practice dimension of EN4.39 focuses on the pre-operative counselling, consent, and post-operative management that are the direct interface between the ENT team and the patient and family. At the KH level, you are expected to understand and communicate these elements clearly — this is the clinical skill most frequently tested in final-year assessments and most practically relevant in your role as a junior doctor on the ENT ward. The ability to explain a procedure clearly, obtain valid informed consent, and provide precise post-discharge instructions is a core professional competency that bridges the gap between a technically successful operation and a safe patient outcome in the community.
Pre-operative counselling for tonsillectomy:
The patient (and parent if the patient is a child) must be counselled on:
- The indication for surgery and why conservative management has been exhausted or is inappropriate.
- The procedure itself: general anaesthesia, oral route, approximately 30–45 minutes, 1–2 day hospital stay.
- Complications to be discussed at consent (standard of care — must be mentioned):
- Pain (significant, lasting 10–14 days; worst on days 3–5).
- Secondary haemorrhage (1–2%) — occurs 5–10 days after surgery; patient must return immediately if any bleeding from the mouth occurs.
- Primary haemorrhage (rare, <1%).
- Risk of anaesthesia (general).
- Rare: taste change, velopharyngeal insufficiency.
- Post-operative diet: soft foods and adequate fluid intake; avoid hard, rough, or spicy foods for 2 weeks.
- Activity: avoid strenuous activity and contact sports for 2 weeks.
- School/work: typically 2 weeks off.
Post-discharge instructions — secondary haemorrhage warning (non-negotiable):
Every patient discharged after tonsillectomy must receive explicit verbal and written instructions: 'If you see any blood in your mouth, or spit out any blood, at any time in the first two weeks after the operation — come to the emergency department immediately, do not wait at home.' This instruction must be given to the patient AND to the responsible adult (parent, carer). Secondary haemorrhage is unpredictable and can escalate rapidly.
Combined tonsillectomy and adenoidectomy (T&A) vs tonsillectomy alone:
In children with both recurrent tonsillitis and adenoid hypertrophy contributing to obstruction or recurrent otitis media, T&A (combined procedure) is performed. In adults, adenoid tissue has usually involuted by the third decade, and adenoidectomy alone is rarely indicated except for nasopharyngeal pathology. The decision to combine or separate the procedures depends on the child's age, dominant indication, and presence of contraindications (submucous cleft).
Assessment of combined indications:
- Child with recurrent tonsillitis (meeting Paradise criteria) AND significant adenoid hypertrophy with mouth breathing → T&A.
- Child with persistent glue ear requiring repeat grommets AND adenoid hypertrophy → adenoidectomy ± grommets, not tonsillectomy (unless tonsillitis also meets criteria).
- Adult with suspected tonsillar malignancy → unilateral tonsillectomy for histology — adenoidectomy not indicated.
SELF-CHECK
Eight days after tonsillectomy, a 7-year-old child's parents call the emergency department to say the child has had two episodes of fresh blood in the mouth. The child is awake and talking. The parents ask if they should 'just monitor at home as the bleeding has stopped.' The correct advice is:
A. Monitor at home with ice chips to the throat, and come in if bleeding resumes
B. Come immediately to the emergency department — all secondary haemorrhage after tonsillectomy requires immediate hospital assessment
C. Call the GP in the morning for an antibiotic prescription as this is likely infection
D. Return to the ward only if there is more than 100 mL of blood loss
Reveal Answer
Answer: B. Come immediately to the emergency department — all secondary haemorrhage after tonsillectomy requires immediate hospital assessment
Secondary haemorrhage after tonsillectomy (occurring 5–10 days post-operatively) requires immediate return to hospital regardless of whether the bleeding appears to have stopped at the time of the call. The bleeding can restart suddenly and escalate rapidly, potentially compromising the airway with a clot. There is no safe threshold at home — any blood from the mouth after tonsillectomy warrants immediate emergency assessment, IV access, blood group and save, and ENT review. The 'wait and see' approach has been associated with preventable deaths. A GP antibiotic is not the appropriate first response.
Self-Assessment: Tonsillectomy and Adenoidectomy
Work through the following questions to consolidate your understanding of the indications, technique, and complications covered in this module. These reflect the expected knowledge level at EN4.39 (KH — Knowledge for the Help of the Patient).
Question 1. A 4-year-old child is brought for ENT assessment. She has had 3 documented tonsillitis episodes per year for the past 3 years (each with fever and tonsillar exudate). She also snores loudly every night and her parents have observed brief pauses in breathing during sleep. Does she meet criteria for surgery? If so, what operation would you recommend?
Answer: Yes — she meets the Paradise criteria for tonsillectomy on the basis of ≥3 documented episodes per year for 3 consecutive years. Additionally, the history of snoring with apnoeic episodes suggests obstructive sleep apnoea (OSA) from tonsillar (and possibly adenoid) hypertrophy — a separate independent indication for surgery. Combined tonsillectomy and adenoidectomy (T&A) would be recommended, addressing both the recurrent infection and the obstruction.
Question 2. Before performing an adenoidectomy on a 5-year-old, the surgeon carefully inspects the uvula and soft palate. A bifid uvula is noted. What is the significance of this finding, and how does it change the surgical plan?
Answer: A bifid uvula is a surface marker for a possible submucous cleft palate — the triad of bifid uvula + zona pellucida (thin translucent midline zone in the soft palate) + notch in the posterior border of the hard palate. Adenoidectomy in a child with a submucous cleft (or overt cleft palate) risks velopharyngeal insufficiency (VPI) — because the adenoid is contributing to velopharyngeal closure in a child whose palatal musculature cannot compensate after its removal. The surgical plan should be revised: the adenoidectomy may be deferred or modified (partial adenoidectomy preserving some inferior tissue), and a speech and language therapy assessment should be performed pre-operatively.
Question 3. What are the three types of post-tonsillectomy haemorrhage? Which is the most important to counsel patients about before discharge?
Answer: Primary haemorrhage (within 24 hours, from inadequate intraoperative haemostasis), reactionary haemorrhage (within 24 hours, from blood pressure reversal), and secondary haemorrhage (5–10 days post-operatively, from eschar sloughing). Secondary haemorrhage is the most important to counsel about before discharge — it occurs after the patient has left hospital, is unpredictable, and requires immediate return to the emergency department for any blood from the mouth. Failure to return promptly is the avoidable risk factor associated with serious outcomes.
CLINICAL PEARL
Secondary haemorrhage after tonsillectomy is the complication most likely to kill a patient after they have already been discharged home safely. It occurs 5–10 days post-operatively when the eschar sloughs — the patient may feel well for a week before suddenly spitting fresh blood. The single most important action you can take as the doctor discharging the patient is to give the secondary haemorrhage warning clearly, repeatedly, and in writing: 'Any blood from the mouth in the 2 weeks after tonsillectomy = immediate emergency department visit, no exceptions.' Never minimise this instruction.