Page 1 of 15
PE1.1 | Growth Terminology and Determinants — SDL Guide
Learning Objectives
- Define the terms growth, development, maturation, velocity, distance, and catch-up growth with precision
- Describe normal patterns of weight, length/height, and head circumference gain from birth through adolescence
- Enumerate and explain the genetic, hormonal, nutritional, and environmental determinants of growth
- Apply knowledge of growth determinants to recognise growth failure and understand catch-up growth in clinical practice
INSTRUCTIONS
Growth monitoring is among the most powerful tools in paediatric clinical practice. A single anthropometric measurement tells you where a child stands; a series of measurements over time—plotted on a growth chart—reveals the trajectory of a child's health. Understanding the precise terminology of growth and the forces that shape it is the foundation for interpreting any growth chart, counselling any parent, and recognising when a child's body is signalling a problem. This module builds that foundation.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 2 (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 24–25 (textbook)
- IAP 2015 Growth Standards for Indian Children (guideline)
- WHO Child Growth Standards, WHO Multicentre Growth Reference Study, 2006 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-month-old girl is brought to a rural health centre by her anxious mother. 'She looks thin compared to her elder sister at this age,' the mother says. The child's weight is 6.2 kg, length 66 cm, and head circumference 43 cm. Before you can reassure or investigate, you need to answer two prior questions: Is this normal for her age? And if not—what could be driving it? The answers require you to know not just what growth is, but how it is measured, what it normally looks like, and what shapes it. That is what this module is about.
WHY THIS MATTERS
Growth monitoring is the paediatrician's simplest and most continuous diagnostic tool. It reveals undernutrition earlier than clinical signs appear, uncovers endocrine disorders that present insidiously, and tracks the effectiveness of interventions for chronic disease. In India, where undernutrition remains a leading cause of childhood morbidity and mortality, every healthcare worker—from the ASHA at the village level to the consultant at a tertiary centre—participates in growth surveillance. Understanding the terminology and determinants of growth is therefore not academic; it directly informs what you do at every child health visit throughout your clinical career.
RECALL
Before reading further, recall from your Physiology course:
• The anterior pituitary secretes growth hormone (GH), which stimulates the liver to produce insulin-like growth factor-1 (IGF-1); IGF-1 acts on growth-plate chondrocytes to promote longitudinal bone growth.
• The hypothalamic–pituitary–thyroid axis: thyroid hormone is permissive for GH action and essential for normal brain maturation.
• Fetal growth is largely insulin- and nutrient-driven (GH-independent in utero); postnatal growth switches to GH-IGF-1 dependence.
From Biochemistry, recall that protein and energy are the primary macronutrient determinants of somatic growth, and that micronutrients (zinc, iron, iodine) have specific regulatory roles.
Why Growth Monitoring Matters in Paediatric Practice
Growth is one of the defining features of childhood—it is the biological substrate through which genetic potential meets environmental opportunity. In clinical paediatrics, monitoring growth serves two complementary functions: surveillance of the individual child for early detection of deviation, and population-level assessment of nutritional and health status. The concept of growth as a vital sign has been operationalised in India through the Integrated Child Development Services (ICDS), the Pradhan Mantri Matru Vandana Yojana, and the Reproductive and Child Health programme, all of which mandate regular weight monitoring of children under five.
Provided image
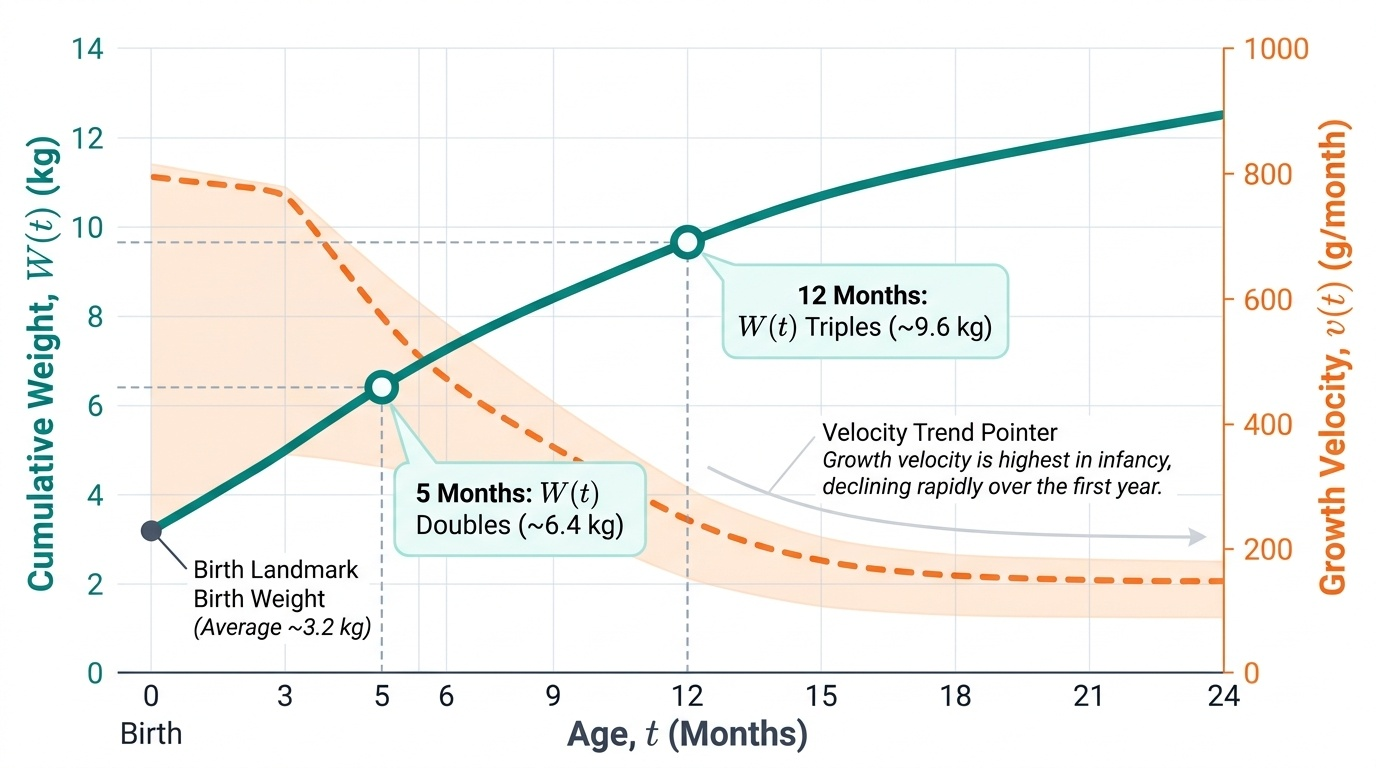
The clinical importance of growth monitoring arises from a simple biological fact: growth velocity is highest and most vulnerable to perturbation during infancy and early childhood. A child who is growing normally is almost certainly thriving in the broad sense—well-nourished, free of significant chronic disease, and experiencing adequate psychosocial stimulation. Conversely, growth faltering (a sustained drop in weight-for-age percentile) is among the earliest measurable signals of an underlying problem, often preceding clinical signs of illness or malnutrition by weeks to months. For the final-year MBBS student entering clinical postings, competence in growth monitoring begins with mastery of terminology and the science of determinants covered in this module.
Key Terminology: Growth vs Development
Precision in terminology is essential because the terms 'growth' and 'development' are often used interchangeably in lay language but carry distinct, operationally important meanings in paediatrics. Confusing them leads to errors in assessment, documentation, and counselling.
Growth refers to a quantitative increase in physical dimensions—size, mass, or organ volume. It is measured in grams, centimetres, or millilitres and is objective and reproducible. Development, by contrast, refers to a qualitative increase in functional capacity and complexity—the acquisition of skills, behaviours, and adaptive responses. Development is assessed by observing milestone attainment, not by measuring physical dimensions.
Maturation is a third related concept: the process by which tissues and organs acquire their full adult functional capacity. Maturation may precede, accompany, or follow growth—for example, the immune system matures over years after birth even as it is already physically present.
Within growth itself, two further distinctions matter clinically:
- Distance (attained) growth: the cumulative size at a given point in time—e.g. a child's weight of 8 kg at 12 months. This is what a single measurement gives you.
- Velocity (incremental) growth: the rate of growth over a defined interval—e.g. weight gain of 200 g per month between 6 and 12 months. Velocity is more sensitive for detecting growth problems than attained size alone, because a small child growing rapidly may be healthier than a larger child growing slowly.
Catch-up growth describes the accelerated growth that occurs after removal of a growth-limiting factor—such as nutritional rehabilitation after undernutrition, or thyroxine replacement in hypothyroidism. Catch-up growth requires both the limiting factor to be removed and adequate nutritional support; it demonstrates the biological elasticity of the growing child.
| Term | Definition | Key measurement | Clinical use |
|---|---|---|---|
| Growth | Quantitative increase in physical dimensions | Weight (g/kg), length/height (cm), HC (cm) | Undernutrition, obesity, organic disease screening |
| Development | Qualitative acquisition of functional skills | Milestone attainment (age-based) | Neurodevelopmental assessment, early intervention |
| Maturation | Functional completion of tissue/organ capacity | Bone age, sexual maturity rating (Tanner) | Puberty assessment, endocrine disorders |
| Velocity | Rate of change per unit time | g/month, cm/year | Early detection of growth faltering |
| Catch-up growth | Accelerated growth post-limiting-factor removal | Delta weight, delta height over interval | Response to treatment, nutritional rehabilitation |
Normal Growth Patterns Across Childhood
Understanding what constitutes normal growth requires knowledge of the expected incremental rates at different ages—not as a memorised list, but as a conceptual map of the biological transitions that drive them. Growth is not linear across childhood: it follows a characteristic deceleration curve in which the highest velocity occurs in infancy and then progressively slows until the pubertal growth spurt provides a second peak before growth ceases at epiphyseal fusion. Each phase is driven by distinct hormonal mechanisms: infancy by nutrition and thyroid hormone, mid-childhood by GH/IGF-1, and puberty by sex steroids superimposed on GH. Knowing these transitions allows the clinician to interpret any individual measurement against the expected range for that age and growth phase, and to recognise immediately when a child's velocity is outside the expected corridor.
Provided image
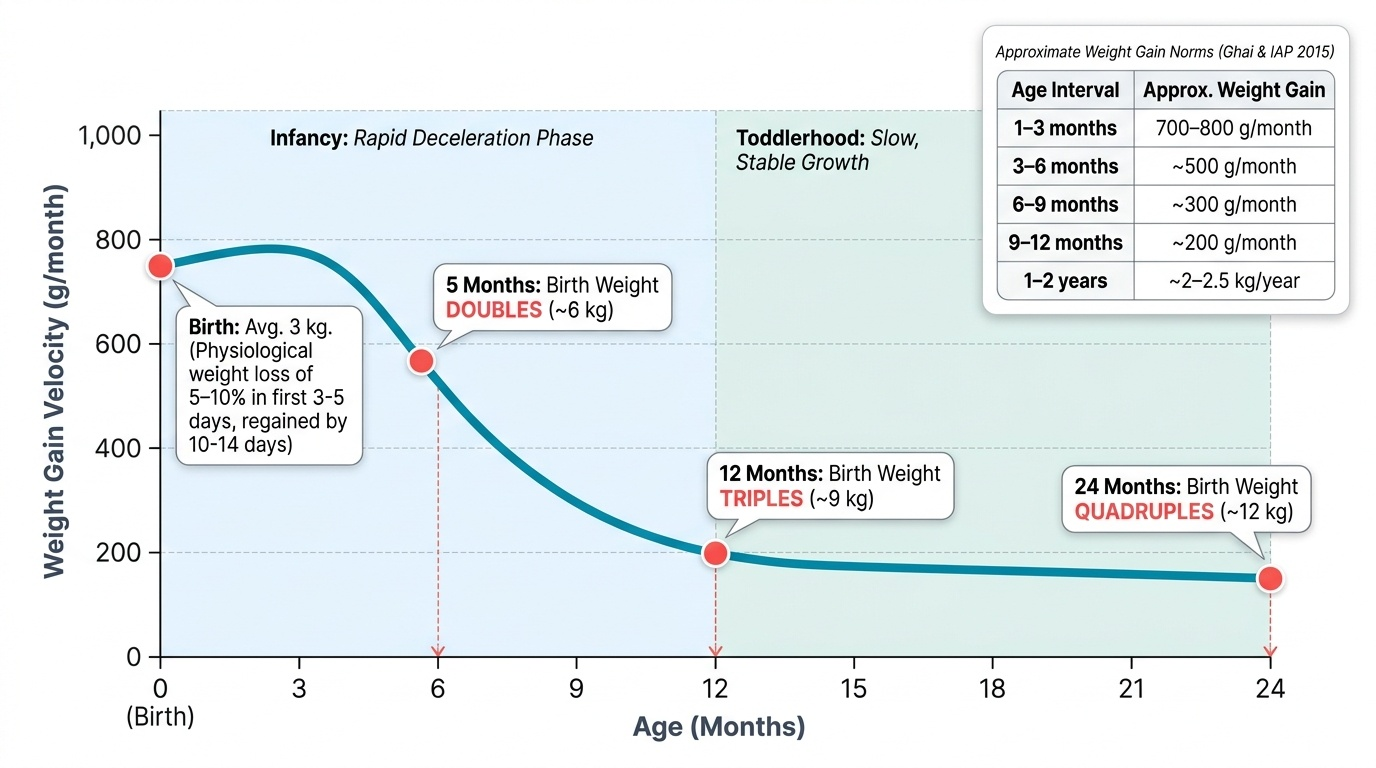
Weight gain norms (approximate, per Ghai's and IAP 2015):
- Birth weight: average 3 kg in a term Indian newborn. Physiological weight loss of 5–10% occurs in the first 3–5 days (regained by 10–14 days).
- Infancy (rapid phase): gains approximately 700–800 g/month in months 1–3, decelerating to ~500 g/month at 3–6 months, ~300 g/month at 6–9 months, and ~200 g/month at 9–12 months.
- Key landmarks: birth weight doubles by approximately 5 months, triples by 12 months, and quadruples by 2 years. These are high-yield landmarks for clinical use.
- Beyond infancy: weight gain slows to approximately 2–3 kg/year in pre-school and school-age years, then accelerates during the pubertal growth spurt.
Length/height norms:
- Birth length: ~50 cm. Increases by approximately 25 cm in year 1 (reaching ~75 cm), then 12–13 cm in year 2 (reaching ~87 cm), and approximately 5–6 cm/year in middle childhood.
- Adult height prediction uses parental heights (mid-parental height ± 6.5 cm for boys/girls).
Head circumference (HC):
- Birth: ~34 cm. Gains ~2 cm/month in the first 3 months, then ~1 cm/month for months 4–6, then ~0.5 cm/month for months 7–12, reaching ~47 cm at 12 months.
- Chest circumference equals head circumference at approximately 1 year; beyond this age, chest circumference exceeds head circumference. This crossover is a simple clinical landmark.
- HC reflects brain growth: rapid expansion in the first 2 years mirrors rapid cortical development; deviation from expected HC percentiles warrants neurological evaluation.
SELF-CHECK
A child's weight is 9 kg and length is 75 cm. The most likely age is:
A. 3 months
B. 6 months
C. 12 months
D. 18 months
Reveal Answer
Answer: C. 12 months
Birth weight (~3 kg) triples by 12 months (~9 kg). Birth length (~50 cm) increases by ~25 cm in year 1, reaching ~75 cm at 12 months. Both measurements together point to 12 months.