Page 8 of 26
PE18.{4,9} | Cold Chain Practice — SDL Guide
Learning Objectives
- Define cold chain and explain the consequences of cold chain failure for vaccine potency
- Identify the components of the cold chain system — ILR, deep freezer, vaccine carrier, cold box, VVM — and state the temperature range and vaccines appropriate for each
- Classify vaccines as freeze-sensitive or heat-sensitive and state the handling implications for each class
- Demonstrate knowledge of the shake test, VVM reading, reconstitution technique, open vial policy, and multi-dose vial reuse rules
- Describe the steps to take when a cold chain failure is suspected, including documentation and reporting
INSTRUCTIONS
A vaccine that has been damaged by heat or freezing provides no protection, yet it is administered with the same discomfort, time, and cost as an effective vaccine — and the child leaves falsely believing they are protected. Cold chain failures are one of the most preventable causes of vaccine-preventable disease outbreaks. This module gives you the knowledge to observe, recognise, and ensure safe cold chain practice in any setting — from a district hospital ILR to a field immunization session.
References
- Ghai Essential Pediatrics, 9th edition, Chapter on Immunization (textbook)
- WHO Cold Chain Management — Training for Health Workers, WHO/IVB/2015 (guideline)
- National Cold Chain Manual, Ministry of Health and Family Welfare, Government of India (guideline)
- Park's Textbook of Preventive and Social Medicine, Chapter on Immunization (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
During a rural immunization camp, you notice the PHC health worker reaching into a vaccine carrier and pulling out vials stored directly against ice packs without any padding. Several vials of pentavalent vaccine show white flocculent material visible through the glass. Another health worker is about to administer this vaccine to a 6-week-old infant. You recognise something is wrong — but can you articulate what has happened, which vaccines are affected, and what must be done? Can you explain to the health worker, without embarrassment, why this particular 'cold chain failure' is dangerous and what the correct practice should have been?
WHY THIS MATTERS
Cold chain management is not a logistic or administrative topic — it is a clinical and public health skill. A single cold chain failure at a peripheral immunization site can render an entire session's vaccines ineffective, leaving dozens of children unprotected while their parents believe they are protected. Freeze damage to adsorbed vaccines (DPT, HepB, TT) is invisible without the shake test, meaning a damaged vial looks identical to a good one — making knowledge of the shake test, VVM reading, and temperature monitoring essential clinical skills. As a final-year student you will observe immunization sessions; competency PE18.9 requires you to understand what you are observing, not merely to watch passively.
RECALL
Recall from the Vaccine Classification module: vaccines are broadly live-attenuated or non-live (inactivated, toxoid, subunit/conjugate). The biological vulnerability of each type determines its cold chain requirements: live-attenuated vaccines (OPV, BCG, MR) are highly heat-sensitive because the attenuated organism can lose viability at elevated temperatures; non-live adsorbed vaccines (DPT, pentavalent, HepB, TT) are freeze-sensitive because their aluminium adjuvant-antigen complex is physically disrupted by freezing, destroying the immune-stimulating structure. Understanding this distinction is the conceptual foundation for cold chain management.
Cold Chain: Concept and Clinical Relevance
The cold chain is defined as the system of storage equipment, transport containers, and trained personnel that together maintain vaccines within the required temperature range from the point of manufacture to the point of administration. For most vaccines in the National Immunization Schedule, this required range is +2°C to +8°C, though some vaccines (notably OPV) require sub-zero temperatures for long-term central storage. The 'chain' metaphor is deliberate — it reflects that the system is only as strong as its weakest link: a single break in temperature control at any point in the supply chain (manufacturer → central store → district cold chain point → PHC → outreach session → clinic → administration) can render all vaccines in that batch ineffective.
The clinical relevance of cold chain management is direct and serious. Vaccines that have lost potency through temperature deviation do not protect against disease, but they are indistinguishable from effective vaccines on visual inspection alone — except for heat exposure tracked by the VVM. A child who receives a freeze-damaged pentavalent vaccine will not develop immunity to diphtheria, pertussis, tetanus, hepatitis B, or Hib, yet the health record will show vaccination completed. When an outbreak occurs, the origin may be traced to a cold chain failure that happened weeks or months earlier — making the break hard to diagnose and the consequences widespread.
Cold chain failures are classified by cause: heat exposure (power outages, refrigerator malfunction, vials left outside the cold chain at ambient temperature); freezing (ice packs in direct contact with freeze-sensitive vaccines in vaccine carriers, or thermostat malfunction in ILRs); mishandling (vials stored past expiry, opened vials stored incorrectly, reconstituted vaccines not used within the prescribed window); and transport errors (inadequate insulation, prolonged transit beyond the carrier's capacity). Of these, freezing of adsorbed vaccines during transport is particularly common and particularly insidious because the vial appears unchanged after thawing.
Cold Chain Equipment and Vaccine Flow
Components of the Cold Chain System
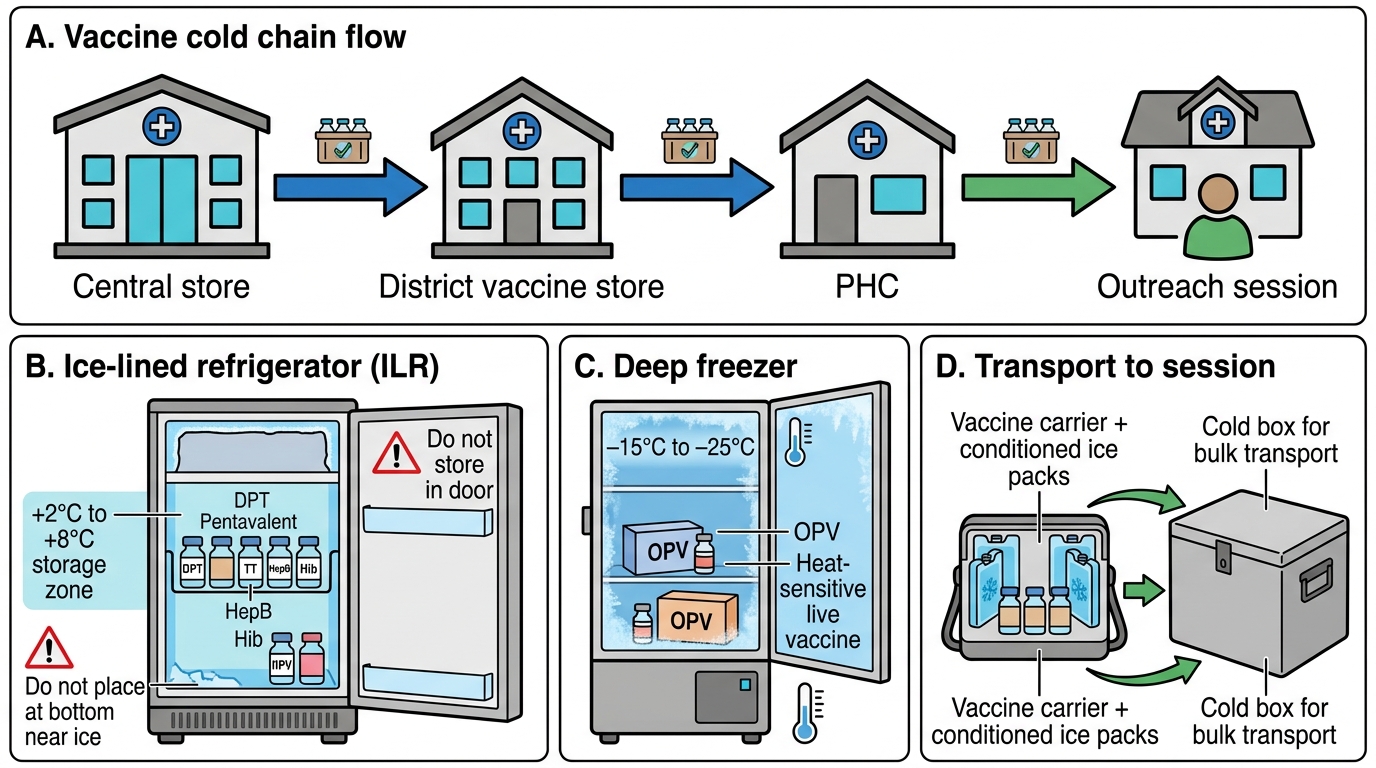
The cold chain system consists of five main categories of equipment, each with a defined temperature range and a specific role in the supply chain from central storage to point of administration.
Ice-Lined Refrigerator (ILR): The ILR is the primary cold chain equipment at PHC and district level. It maintains vaccines at +2°C to +8°C. It has a refrigerating ice lining around the inner walls, which maintains the correct temperature even during power outages of up to several hours — a critical advantage in areas with intermittent power supply. Freeze-sensitive vaccines (DPT, pentavalent, TT, HepB, Hib, fIPV) are stored in the ILR. Vaccines must never be stored in the door (temperature fluctuates) or the bottom compartment (risk of contact with ice that forms). Unopened multi-dose vials of non-live vaccines can be stored in the ILR for reuse at the next session, subject to the open vial policy.
Deep Freezer: Maintains vaccines at −15°C to −25°C. Used for long-term storage of heat-sensitive live vaccines, principally OPV (which must be stored at −20°C at the central and district level to preserve maximum potency). BCG and MR vaccines (freeze-dried) may be stored at −15°C to −25°C or at +2°C to +8°C depending on the level of the supply chain.
Vaccine Carrier: A portable insulated container (styrofoam or thick plastic) used for transporting vaccines and for storage at outreach/field sessions. Loaded with conditioned ice packs (ice packs that have been left at room temperature until the water in them just begins to melt, so they are at 0°C rather than −15°C). The conditioned ice packs prevent the carrier temperature from falling below 0°C, thereby protecting freeze-sensitive vaccines while still maintaining the ≤+8°C range. A properly loaded vaccine carrier maintains the correct temperature for up to 12 hours. Freeze-sensitive vials must be wrapped in paper or foam and not placed in direct contact with ice packs.
Cold Box: A larger version of the vaccine carrier used for bulk transport from district to PHC. Maintains temperature for 24–48 hours depending on ambient temperature and load.
Vaccine Vial Monitor (VVM): A heat-sensitive chemical indicator affixed to each vaccine vial by the manufacturer. As the vial is exposed to cumulative heat, the inner square of the VVM darkens progressively. Reading: if the inner square is LIGHTER than the outer circle → vaccine is usable (Stages 1–2); if the inner square is the SAME or DARKER than the outer circle → discard (Stages 3–4). The VVM does NOT detect freeze damage — only heat exposure.
| Vaccine | Storage Equipment | Temperature | Sensitivity | Special Notes |
|---|---|---|---|---|
| OPV | Deep freezer (central); ILR (peripheral) | −20°C central; +2 to +8°C peripheral | Highly heat-sensitive | Most vulnerable of all NIS vaccines to heat |
| BCG | Deep freezer or ILR | −15 to −25°C or +2 to +8°C | Heat-sensitive (freeze-dried) | Reconstitute only what will be used; discard after 4 h |
| MR | Deep freezer or ILR | −15 to −25°C or +2 to +8°C | Heat-sensitive (freeze-dried) | Reconstitute; discard after 4 h |
| Pentavalent | ILR | +2 to +8°C | Freeze-sensitive | DO NOT freeze |
| DPT/TT/Td | ILR | +2 to +8°C | Freeze-sensitive | DO NOT freeze |
| HepB | ILR | +2 to +8°C | Freeze-sensitive | DO NOT freeze |
| fIPV | ILR | +2 to +8°C | Freeze-sensitive | DO NOT freeze; single-use vial |
SELF-CHECK
At an outreach immunization session, you find that the vaccine carrier's ice packs were not conditioned before loading and were straight from the deep freezer (at −20°C). Which group of vaccines in the carrier is most at risk from this error?
A. OPV, because it is the most heat-sensitive vaccine
B. DPT and pentavalent, because they are freeze-sensitive and direct contact with −20°C ice can freeze them
C. BCG, because it is a live vaccine
D. MR, because it is a freeze-dried vaccine requiring reconstitution
Reveal Answer
Answer: B. DPT and pentavalent, because they are freeze-sensitive and direct contact with −20°C ice can freeze them
Placing unconditional deep-freezer ice packs (−20°C) directly in contact with vaccines risks freezing the vaccines in the carrier. DPT, pentavalent, TT, and HepB are adsorbed (aluminium adjuvant) vaccines that are freeze-sensitive — freezing physically disrupts the adjuvant-antigen complex and destroys immunogenicity, while the vials appear unchanged after thawing. Ice packs must be conditioned (allowed to sit at room temperature until the outside water begins to melt, reaching ~0°C) before use with freeze-sensitive vaccines. OPV is actually tolerant of sub-zero temperatures; BCG and MR (freeze-dried) can generally withstand −15 to −25°C storage.
Vaccine Handling Technique: Storage, Transport and Administration
Safe vaccine handling encompasses correct storage procedures in the ILR, proper transport in the vaccine carrier, reconstitution technique for lyophilised vaccines, and application of the open vial policy. Each step has a critical checkpoint that prevents vaccine wastage and ensures potency.
ILR loading and management: Vaccines should be loaded into the ILR in a first-in, first-out (FIFO) order so that older stock is used first. The door pockets of the ILR should NOT be used for vaccines (temperature fluctuation). The ILR temperature should be checked twice daily and recorded on a temperature log. The ILR must NOT be overloaded — adequate space is needed for cold air circulation. Ice formation on ILR walls (due to overcooling) should be defrosted regularly; ice-encrusted vials indicate a thermostat problem.
Conditioning ice packs for transport: Ice packs taken from the deep freezer must be conditioned before use in a vaccine carrier by leaving them at room temperature until you can hear the water inside sloshing — indicating the pack has reached approximately 0°C. This prevents the carrier interior from dropping below 0°C and freezing the adsorbed vaccines. Conditioned ice packs are then placed on all four sides and the top of the vaccine carrier, with a layer of paper or foam separating them from the vaccine vials.
The Shake Test (for adsorbed freeze-sensitive vaccines): The shake test is used to detect freeze damage in adsorbed vaccines (DPT, pentavalent, HepB, TT). Procedure: (1) Take a control vial of the same vaccine that is known to have been stored correctly; (2) Shake both the suspect vial and the control vial vigorously for 10–15 seconds; (3) Hold both vials against a light source and observe the rate of sedimentation. Result: If the suspect vial sediments (settles) at the same rate as or SLOWER than the control → vaccine is likely unaffected (use if VVM passes); if the suspect vial sediments FASTER than the control → vaccine has been frozen and the antigen-adjuvant complex disrupted → DISCARD. The rationale: freezing causes the aluminium adjuvant particles to aggregate into larger clumps that settle more rapidly after shaking.
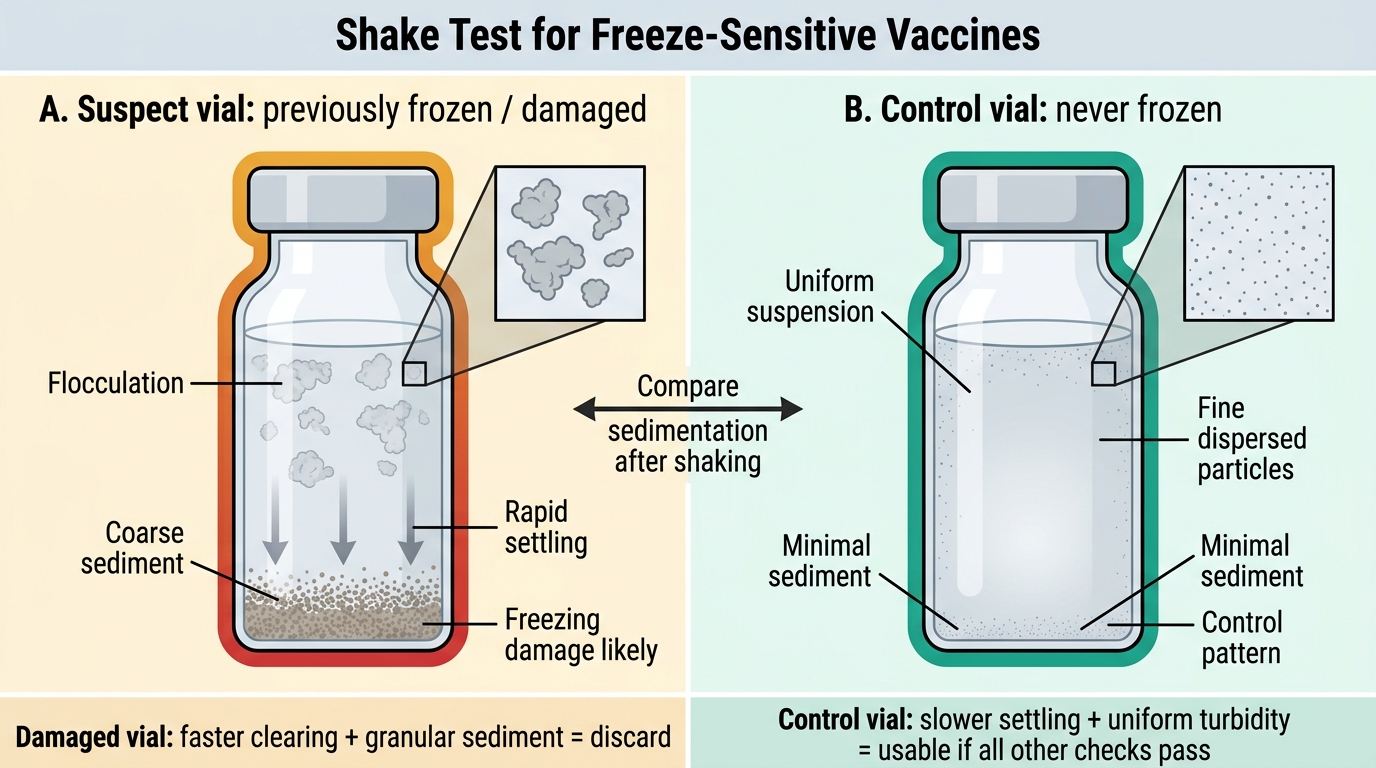
Shake Test for Freeze-Damaged Vaccines
Reconstitution technique (BCG, MR, varicella): Use ONLY the manufacturer-supplied diluent (the reconstitution solution is vaccine-specific and must not be substituted). Add the correct volume of diluent to the lyophilised powder. Mix gently by inverting — do NOT shake vigorously. Once reconstituted, store at +2°C to +8°C and use within 4 hours (WHO/IAP recommendation for BCG and MR). Discard any unused reconstituted vaccine after the session, even if the vial is not empty. Label the reconstituted vial with the time of reconstitution.
Open Vial Policy (OVP): Under the NIS Open Vial Policy (2014), multi-dose vials of vaccines that meet the following criteria may be kept and used at subsequent sessions: the vaccine has not expired; the VVM is in the usable zone; the vial has been stored at the correct temperature; the vial has not been contaminated. Vaccines NOT to be reused under any circumstances once opened: BCG, MR, all reconstituted lyophilised vaccines, and varicella. Opened vials of pentavalent, OPV, and TT may be reused at subsequent sessions within 28 days (pentavalent) or the schedule window (OPV), provided VVM, expiry, and temperature are verified each time.
CLINICAL PEARL
The freeze-sensitive vaccine trap during transport: The most common cold chain failure that students misidentify is freezing of adsorbed vaccines. Because ice is associated with 'cold preservation' in everyday thinking, many students assume that a vial that has been frozen and then thawed is still good — after all, frozen food thaws safely. This is incorrect for adsorbed vaccines. Freezing DPT, HepB, or pentavalent disrupts the physical structure of the aluminium adjuvant, permanently inactivating the immune-stimulating matrix. The vial looks completely normal after thawing — no turbidity, no colour change, no precipitate detectable by eye. The ONLY way to detect this damage at point-of-use is the shake test. Always perform the shake test on suspect vials and never skip it because the vaccine 'looks fine.'