Page 11 of 26
PE18.5 | Immunization in Special Situations — SDL Guide
Learning Objectives
- Explain the general principles that govern vaccine modification in special clinical situations — identify, classify, assess, and decide
- State the immunization approach for HIV-positive children, including CD4 thresholds for live vaccines, OPV vs IPV substitution, and timing relative to ART
- Describe immunization in children with primary immunodeficiency, undergoing chemotherapy, or following organ transplantation
- Apply the chronological age principle for preterm and low birth weight infants; state the BCG deferral criterion and the exception for hepatitis B in infants of HBsAg-positive mothers
- State the deferral intervals for live vaccines after blood products, the vaccines prioritised in asplenia, the adolescent catch-up schedule, and the vaccines recommended for travellers
INSTRUCTIONS
Most children in 'special situations' are MORE vulnerable to vaccine-preventable diseases than healthy children — HIV, asplenia, and prematurity all impair immunity or increase the consequences of infection. The reflex to withhold all vaccines from such children is not only wrong but potentially fatal. The correct approach is systematic: identify the situation, classify the vaccine as live or non-live, assess the degree of immunocompromise, and make a specific, justified decision for each vaccine. This module gives you that decision framework.
References
- Ghai Essential Pediatrics, 9th edition, Chapter on Immunization — Special Situations (textbook)
- IAP Advisory Committee on Vaccines and Immunization Practices (ACVIP) 2024 — Immunization in Special Circumstances (guideline)
- WHO Position Papers on Vaccines in Immunocompromised Patients, WHO/IVB (guideline)
- Nelson Textbook of Pediatrics, 21st edition — Immunization (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are posted in a paediatric HIV clinic. A mother brings her 10-week-old infant who was born to an HIV-positive mother. The infant's HIV status is still being confirmed by early infant diagnosis (EID). The infant is due for the 10-week NIS vaccines — pentavalent, OPV, rotavirus, and fIPV. The nurse asks: 'Can we give all the vaccines as normal? Should we skip OPV because the baby might be HIV-positive?' Meanwhile, the mother has a 4-year-old sibling who is confirmed HIV-positive with a CD4 count of 18% and is currently on ART. The 4-year-old is overdue for MR. What would you advise for each child?
WHY THIS MATTERS
Children in special clinical situations are not a small minority — in India, hundreds of thousands of children live with HIV, millions are born preterm, and children with cancer, primary immunodeficiency, organ transplants, and asplenia require individualised immunization planning throughout their childhood. A doctor who applies the standard NIS without modification to these children risks causing harm (live vaccine in a severely immunocompromised child can cause disease) or leaving them unprotected (withholding safe non-live vaccines from a child who urgently needs them). The ability to navigate these special situations confidently is a core clinical skill for any practitioner working with children.
RECALL
Recall from Vaccine Classification: vaccines are categorised as live-attenuated or non-live. Live vaccines (BCG, OPV, MR, rotavirus, JE-live, varicella) replicate in the host — this replication means they can cause disease in immunocompromised hosts. Non-live vaccines (inactivated, toxoid, subunit, conjugate: IPV, HepB, DPT, pentavalent, TT, PCV, HPV, HepA, TCV) cannot replicate and are safe even in severely immunocompromised patients, though their immunogenicity may be reduced. This live/non-live distinction is the central decision-making axis for all special situations.
Why Special Situations Require Modified Immunization Strategies
The fundamental goal of immunization — to protect the individual against vaccine-preventable disease — does not change in special situations. What changes is the risk-benefit calculation for each vaccine type. In most special situations, the majority of NIS vaccines (the non-live ones) can and should be given as scheduled or as soon as the situation is identified, because the child's vulnerability to infection is greater than that of healthy children, not less. The modification is targeted, not wholesale, and is based on a small number of well-defined principles.
The core principles that govern immunization in special situations are:
Principle 1 — Live vaccines carry replication risk in immunocompromised hosts. When the immune system cannot control a replicating attenuated organism, the attenuated pathogen can cause the disease it was designed to prevent. BCG disease in SCID, vaccine-associated paralytic poliomyelitis (VAPP) in immunodeficiency from OPV, and measles-inclusion-body encephalitis from MR in severe immunocompromise are documented outcomes. The threshold for deferring live vaccines is the degree of immunosuppression — mild-moderate immunosuppression may permit live vaccine use; severe immunodeficiency is an absolute contraindication.
Principle 2 — Non-live vaccines are safe in all immunocompromised patients but may generate a weaker immune response. They should not be withheld; in many cases (PCV, HepB, Hib in asplenia; annual influenza in HIV) they are urgently indicated.
Principle 3 — Defer, not omit. Most live vaccines that cannot be given during a period of immunosuppression can be given later when immunosuppression is resolved or CD4 levels recover. 'Defer' means 'give when it becomes safe'; 'omit' (permanent, unconditional withholding) applies only in permanent severe immunodeficiency (SCID).
Principle 4 — Household contacts matter. If a child in the household is immunocompromised, OPV (which is shed in stool) should be replaced by IPV for all children in that household to prevent VAPP in the immunocompromised index case through contact transmission.
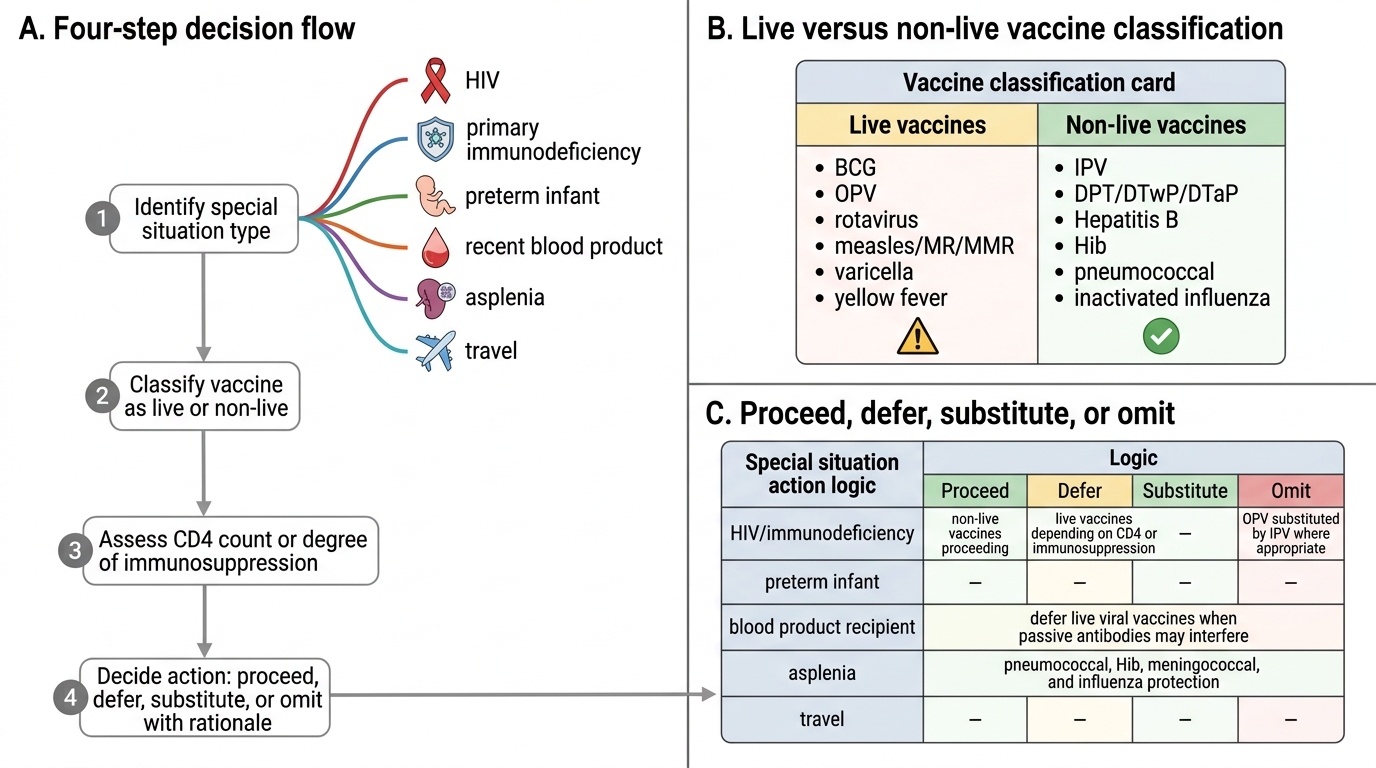
Immunization Decision Flow in Special Situations
Immunization in Children with HIV
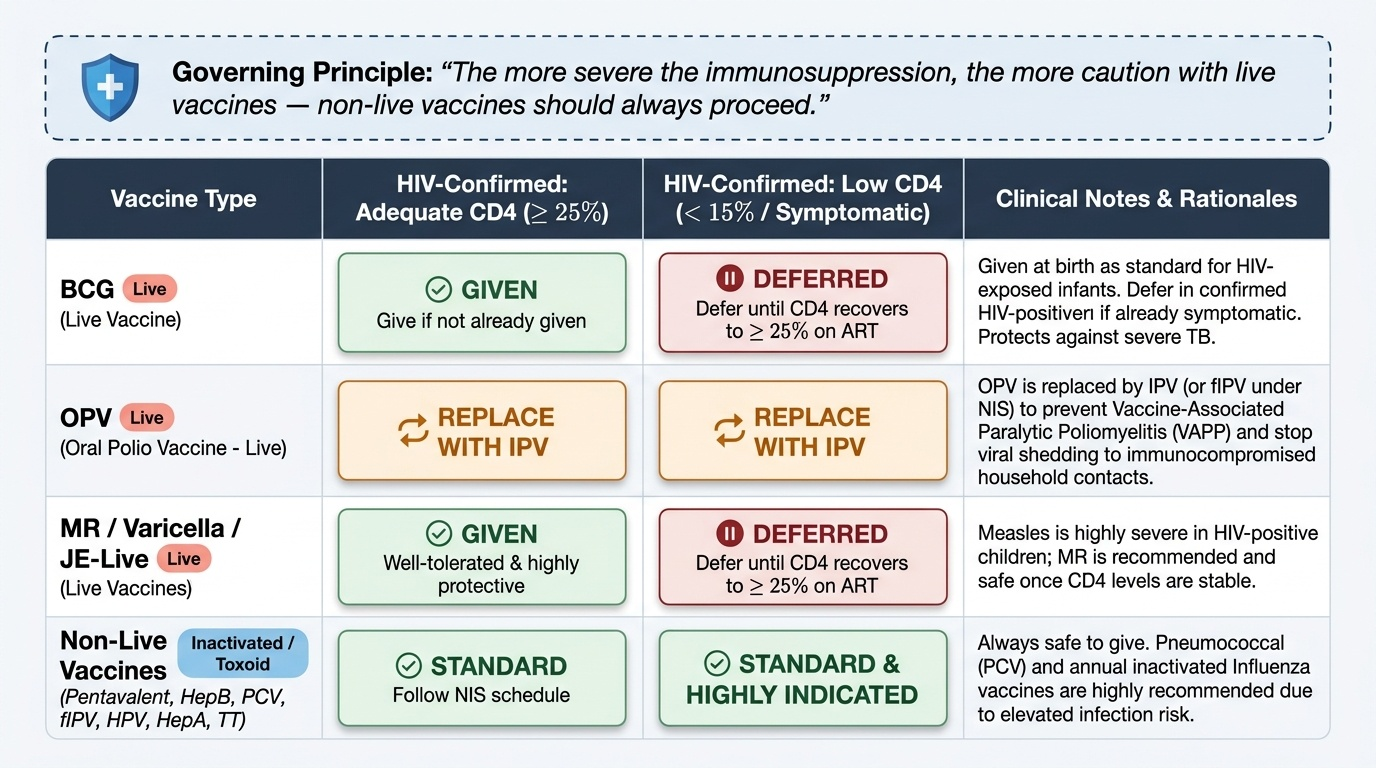
HIV in children is the most common reason for immunization modification in Indian paediatric practice. The approach depends on the child's immune status, assessed by CD4 count or percentage, and whether the child is on antiretroviral therapy (ART). The governing principle is: the more severe the immunosuppression, the more caution with live vaccines — but non-live vaccines should always proceed.
Provided image
HIV-exposed, not yet confirmed (early infancy): Before the infant's HIV status is confirmed by polymerase chain reaction (PCR), the standard NIS schedule is followed except that OPV is replaced by IPV where possible, given that the infant may be HIV-positive. BCG is given at birth as standard, since the risk of disseminated BCG in an HIV-exposed infant is low and the risk of tuberculosis (highly endemic in India) in an unvaccinated HIV-positive infant is high — the balance favours giving BCG at birth.
HIV-confirmed, asymptomatic, CD4 ≥25% (or age-appropriate count): The NIS schedule can largely be followed. Specifically:
• BCG: Give if not already given; defer if child is already symptomatic.
• OPV: Replace with IPV (to prevent VAPP in the child and prevent shedding to immunocompromised household contacts). Under NIS, fIPV can fulfil this requirement.
• MR: Give — MR is recommended for HIV-positive children with CD4 ≥25% because measles is particularly severe in HIV and the attenuated virus is generally well-tolerated at adequate CD4 levels (per WHO/IAP guidance).
• Non-live vaccines (pentavalent, HepB, TT, fIPV, PCV, HPV, HepA): All given as standard schedule.
HIV-confirmed, symptomatic or CD4 <15% (severe immunosuppression):
• Live vaccines DEFERRED — BCG, MR, varicella, JE-live — until CD4 recovers to ≥25% on ART.
• OPV replaced by IPV (as above).
• All non-live vaccines should still be given — and in fact PCV (pneumococcal) and annual influenza (inactivated) are particularly indicated in this group due to the high risk of pneumococcal and influenza disease.
• After ART is started and CD4 recovers to ≥25%, live vaccines can be (re-)given to complete the schedule.
Timing with ART: The optimal timing for live vaccines in HIV is when the child is clinically stable on ART with recovering CD4. There is no fixed CD4 number for 'safe' live vaccine administration beyond the ≥25% guideline — clinical judgment and IAP/WHO guidance should be consulted for individual cases.
SELF-CHECK
A 4-year-old confirmed HIV-positive child on ART for 6 months has a CD4 percentage of 28%. He has not received his second MR vaccine. Which of the following is the correct immunization decision?
A. Defer MR indefinitely as all live vaccines are contraindicated in HIV
B. Give MR today, as the child has adequate CD4 levels (≥25%) and measles risk is high in HIV
C. Give IPV instead of MR as a non-live substitute
D. Check CD4 absolute count and defer until it exceeds 500 cells/µL
Reveal Answer
Answer: B. Give MR today, as the child has adequate CD4 levels (≥25%) and measles risk is high in HIV
MR (measles-rubella) is a live vaccine, but WHO and IAP recommend it for HIV-positive children who are clinically stable and have adequate immune function, defined as CD4 ≥25% for children aged 12 months to 5 years. At CD4 28%, this child meets the threshold. Measles is particularly severe and often fatal in HIV-positive children; the benefit of protection outweighs the risk of the attenuated virus at this CD4 level. Option A is incorrect — live vaccines are NOT uniformly contraindicated in HIV; CD4 assessment governs the decision. IPV is not a substitute for MR (it covers polio, not measles). CD4 absolute count threshold of 500 is not the IAP/WHO criterion used in this context.
Immunization in Primary Immunodeficiency, Chemotherapy, and Transplant
Children with primary immunodeficiency (PID), those undergoing chemotherapy, and those who have received organ transplants represent distinct but conceptually related special situations where the ability to mount and control an immune response is severely or transiently impaired. The approach differs slightly among these groups because the duration and reversibility of immunosuppression differs: PID is often permanent, chemotherapy is transient but profoundly suppressive during treatment, and transplant recipients remain on long-term moderate immunosuppression. In all three, the live/non-live distinction is the central axis — but the timing of when live vaccines can be safely (re-)introduced differs significantly, and understanding these differences is essential for planning individualised immunization schedules.
Primary immunodeficiency (PID): PID encompasses a spectrum from severe combined immunodeficiency (SCID — the most severe, with absent T- and B-cell function) to selective IgA deficiency (mild). The severity of PID determines the vaccine modification:
• SCID and severe PID: All live vaccines are permanently contraindicated — BCG at birth in an undiagnosed SCID infant can cause fatal disseminated BCG disease. If SCID is diagnosed after BCG was given, the child requires anti-TB prophylaxis and monitoring for BCG disease. OPV is contraindicated (VAPP risk). MR, varicella, rotavirus — all withheld. Non-live vaccines can be given but may generate poor immune responses due to the underlying B-cell defect; the child may need IVIG replacement therapy for passive protection.
• Milder PID (complement deficiency, phagocytic defects, isolated antibody deficiencies): Assessment is individualised. Complement-deficient children have impaired killing of encapsulated organisms — they especially benefit from PCV, meningococcal, and Hib vaccines. Some of these children can receive live vaccines; specialist input is required.
Chemotherapy and malignancy: Children on active chemotherapy for haematological malignancy or solid tumours are severely immunosuppressed during treatment and for a period after. The general approach:
• During active chemotherapy: Defer live vaccines entirely. Non-live vaccines may be given but seroconversion is likely reduced; consider repeating doses after treatment.
• Timing: Live vaccines may be given ≥3–6 months after completion of chemotherapy, once the immune system has recovered (lymphocyte counts and vaccine-specific titres are reassuring indicators). This window varies by the agent used.
• Before starting chemotherapy (pre-treatment catch-up): If time permits, complete all due live vaccines at least 4 weeks before immunosuppression begins (4-week safety window ensures an adequate response before the immune system is suppressed).
Organ transplantation: Similar approach to chemotherapy. Pre-transplant: complete all age-appropriate vaccines at least 4 weeks (live) or 2 weeks (non-live) before transplant date. Post-transplant (on immunosuppression): defer all live vaccines for at least 2 years (some guidelines longer); all non-live vaccines can be re-given from 6 months post-transplant. Annual influenza (inactivated) is particularly important in transplant recipients.