Page 18 of 26
PE18.{8,10-12} | Safe Vaccine Administration Workflow — SDL Guide
Learning Objectives
- Describe the components of safe vaccine practice including patient education/counselling, AEFI management, safe injection practices, documentation, and medicolegal implications (PE18.8)
- Correctly document immunization in an immunization record including all required fields (PE18.10)
- Observe and describe the administration of UIP vaccines during a clinical session (PE18.11)
- Demonstrate correct vaccine administration technique on a mannequin including correct site, route, angle, and needle selection for key UIP vaccines (PE18.12)
INSTRUCTIONS
Every vaccine administered correctly is a child protected; every programme error is a preventable harm. India's Universal Immunization Programme (UIP) covers over 26 million newborns each year, and healthcare workers are the last line of defence between a child and vaccine-preventable disease — or vaccine-preventable injury. This module operationalises safe vaccine administration: the 5 rights, cold-chain verification, route-and-site selection, step-by-step injection technique, AEFI recognition and reporting, immunization documentation, and biomedical waste management. Mastery here translates directly into child safety and programme quality.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 10 (Immunization) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 190–198 (Immunization Principles) (textbook)
- Immunization Handbook for Medical Officers, MoHFW India, 2017 (guideline)
- IAP ACVIP Recommended Immunization Schedule 2024–25 (guideline)
- Biomedical Waste Management Rules, MoEFCC India, 2016 (amended 2019) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-week-old infant is brought to your immunization session for her second-dose pentavalent vaccine. The vial has been sitting on the table for 45 minutes after being taken out of the refrigerator. The health worker prepares the dose but does not check the Vaccine Vial Monitor (VVM). She gives the injection into the buttock instead of the anterolateral thigh, and recaps the needle before dropping it into a waste bin. Three hours later, the mother calls to report the baby has a fever of 38.8°C and the injection site is swollen.
Which aspects of this encounter were unsafe, and what harm could each cause? By the end of this module you will be able to identify every error, correct it, document the AEFI, and demonstrate the right technique on a mannequin.
WHY THIS MATTERS
Vaccine-preventable deaths remain a significant contributor to under-5 mortality in India despite decades of the UIP. The programme's success depends not just on WHAT is given but HOW it is given. Programme errors — the wrong site, broken cold chain, incorrect route, or needle reuse — account for a substantial proportion of reported AEFI clusters and, in the worst cases, cause nerve injuries, abscesses, inadvertent IV injection, or transmission of blood-borne pathogens. Safe injection practices protect the child, the immunization worker, and the programme's public trust. Documentation is the medicolegal and epidemiological backbone: without an accurate immunization record, a child may be over-vaccinated (wasted doses, costs) or under-vaccinated (outbreak risk), and an AEFI investigation cannot proceed. As a graduating doctor you will supervise immunization sessions, train health workers, and counsel caregivers — all of which require confident command of this workflow.
RECALL
Before proceeding, recall the following from your study of the NIS schedule:
- The primary series vaccines given at 6, 10, and 14 weeks: pentavalent (DPT + Hep-B + Hib), OPV (oral), Rotavirus, fIPV (fractional inactivated polio).
- Birth-dose vaccines: BCG, OPV-0, Hep-B birth dose.
- The key temperature rule for the cold chain: most vaccines are stored at 2–8°C; OPV is stored at −15 to −25°C (frozen).
- You know that the anterolateral thigh is the recommended site for injections in infants and that BCG is given intradermally. Confirm these recollections — this module will reinforce and operationalise them.
Why Safe Vaccination Practice Matters
Safe vaccine administration is not merely a technical task — it is an ethical obligation, a quality-of-care standard, and a public-health imperative. The World Health Organization defines a vaccine-preventable death as one that occurs despite the existence of an effective vaccine; yet vaccine-administration errors can themselves cause harm, undermining the very benefit the programme exists to deliver. India administers hundreds of millions of vaccine doses every year through the UIP, and any systematic deviation in technique — wrong route, improper cold-chain handling, contaminated equipment — can translate into population-scale harm.
Safe vaccination practice has two dimensions. The first is preventing programme errors: ensuring the right child receives the right vaccine at the right dose via the right route at the right time (the '5 rights of immunization'), stored and handled correctly throughout the cold chain. The second is managing the inevitable: recognising, managing, and reporting adverse events following immunization (AEFI) promptly and correctly, distinguishing vaccine-induced reactions from coincidental events, and fulfilling reporting obligations so the national pharmacovigilance system can respond.
The medicolegal dimension is significant: a poorly documented immunization, a missed AEFI report, or an incorrectly administered vaccine can expose the administering practitioner and the facility to liability under consumer protection and medical negligence law. Conversely, a meticulously completed immunization record is the practitioner's best defence and the child's lifelong asset.
Safe Vaccine Administration Workflow
Governing Principles: The 5 Rights, Cold Chain, and Aseptic Technique
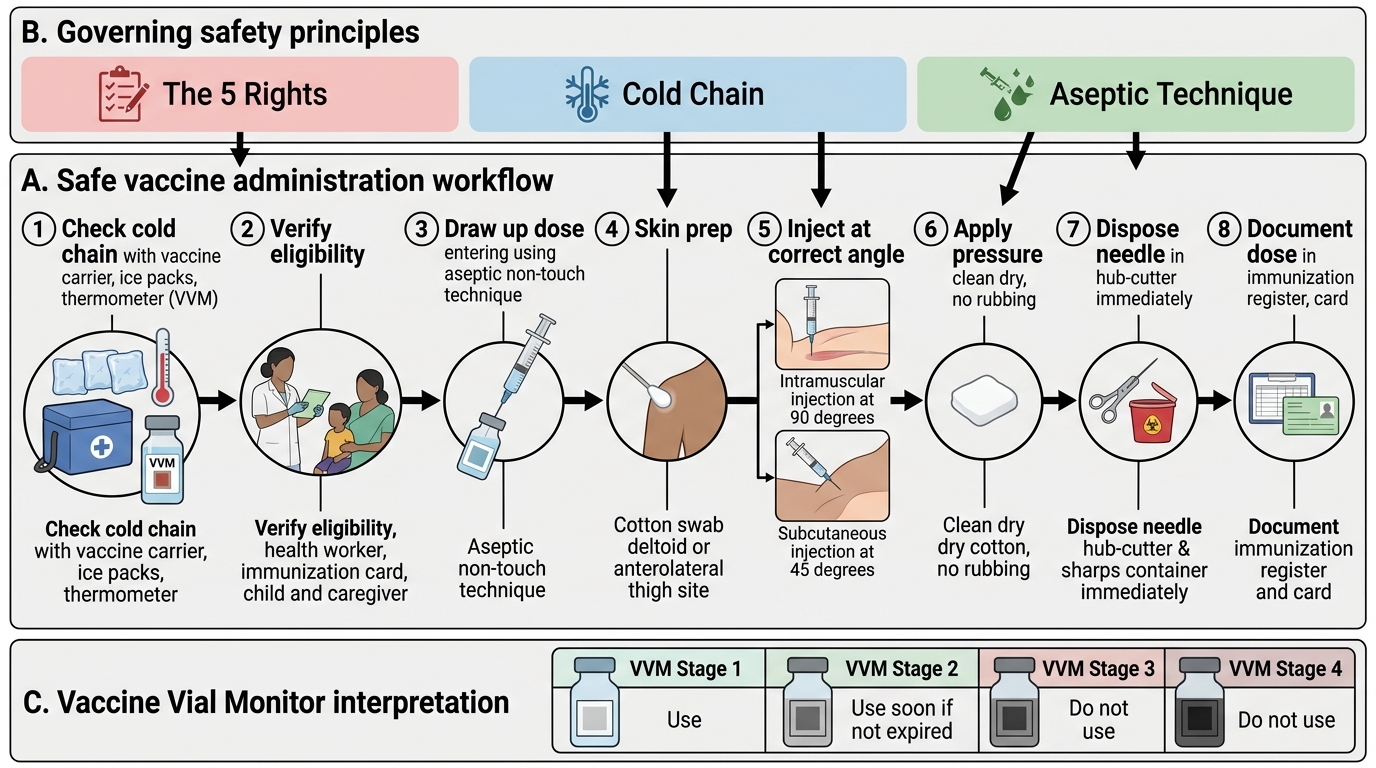
Every safe vaccine administration session is governed by three over-arching frameworks that, when applied together, prevent the majority of programme errors. Understanding WHY each framework exists is as important as memorising its steps, because it enables improvisation when resources are imperfect — as they often are in field settings. A health worker who understands the reasoning behind the cold chain, the 5 Rights, and non-touch technique can adapt correctly when a vial label is unclear, when equipment is missing, or when a child is struggling — rather than defaulting to an unsafe habit. Together these three frameworks form a unified safety system: the 5 Rights prevent identity and timing errors; the cold-chain protocol preserves vaccine potency; and aseptic technique prevents infection. Failing any one of the three can invalidate an otherwise correct administration. These principles apply equally at a district hospital outreach camp, a subcentre session, and a tertiary immunization clinic — the workflow does not change by setting, only the resources available to support it.
Provided image
The 5 Rights of Immunization adapt the pharmacology '5 rights of medication administration' to vaccines:
1. Right patient — verify the child's name, age, and the caregiver's identity against the immunization card; ensure the child meets the eligibility criteria for today's dose and has no current contraindications (acute febrile illness ≥38.5°C; previous anaphylaxis to the vaccine or its components; specific immunological contraindications for live vaccines, e.g. severe immunodeficiency).
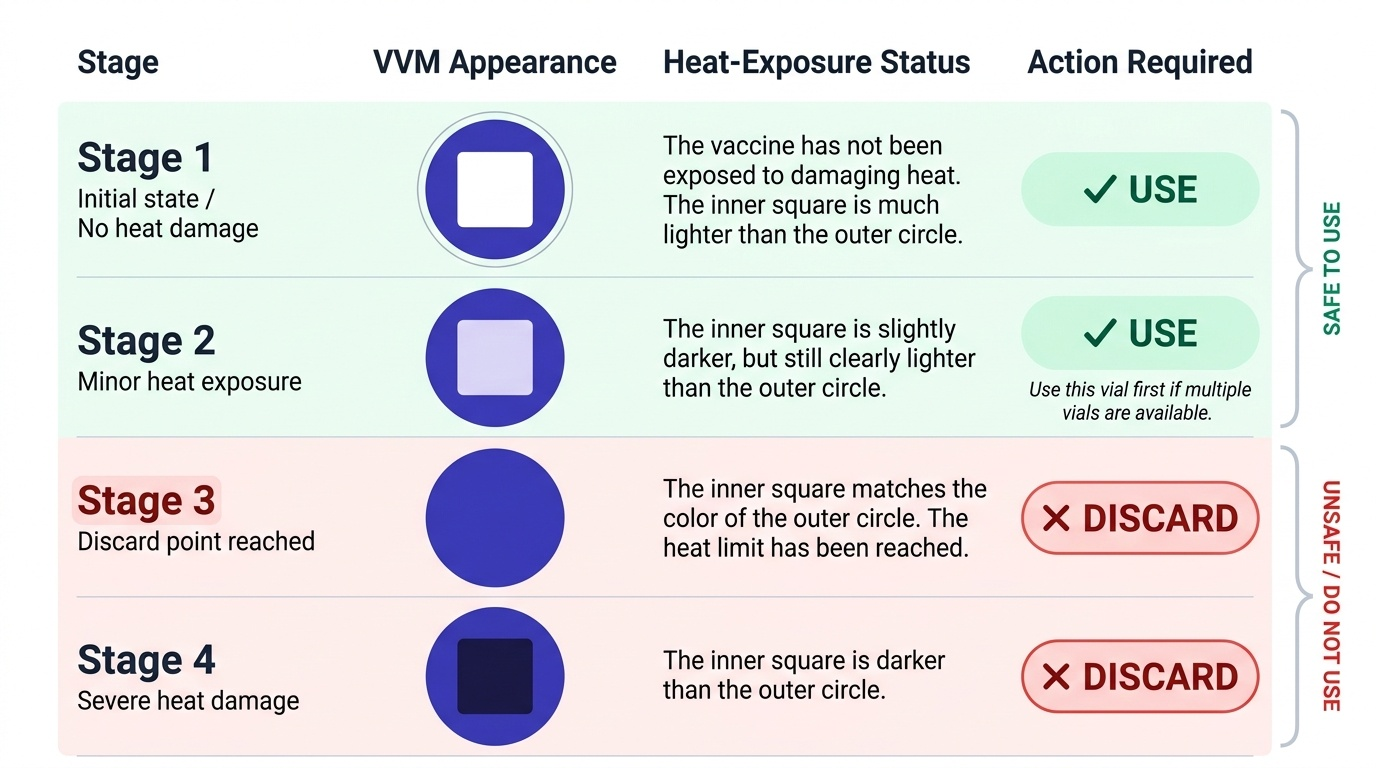
2. Right vaccine — match the vial label to the scheduled vaccine; check the Vaccine Vial Monitor (VVM) — a heat-sensitive label that changes colour irreversibly if the cold chain has been broken (VVM stage 1 or 2 = usable; stage 3 or 4 = discard).
3. Right dose — verify the volume (0.5 mL for most injectable vaccines; 0.05 mL for BCG neonates; 0.1 mL for fIPV fractional dose ID; 2 drops oral for OPV). Use the correct syringe (0.5 mL or 1 mL auto-disable syringe for injectables; BCG requires a separate 1 mL syringe with 26 G needle).
4. Right route — intramuscular (IM), subcutaneous (SC), intradermal (ID), or oral — see the Route and Site section for the map.
5. Right time — given today's visit falls within the recommended window; interval from previous dose is adequate (minimum 4-week interval between pentavalent doses); no recent live vaccine in the last 28 days for another live vaccine.
Cold chain integrity at the point of use: Vaccines must never be left outside the cold chain longer than stipulated. At the session site, vaccines are placed in a vaccine carrier with ice packs maintaining 2–8°C; OPV and varicella maintain −15 to −25°C until just before use. The VVM is the real-time indicator — check it on EVERY vial before drawing up. Reconstituted vaccines (BCG, MR, JE) are used within 4 hours of reconstitution and must not be re-frozen. Opened multi-dose vials of non-reconstituted vaccines (e.g. OPV, Hep-B) may be used for up to 4 weeks under the multi-dose vial policy (MoHFW MDVP) provided the VVM is intact, the cold chain was maintained, and no contamination occurred.
Non-touch aseptic technique (NTAT): The critical aseptic rule for vaccine administration is that the needle and the rubber septum of the vial must never be touched or contaminated. Hands are washed before preparation. Alcohol swabbing of the rubber septum before needle insertion is not routinely required for multi-dose vials under Indian UIP guidelines (and may degrade rubber seals), but the insertion must be clean. The skin at the injection site need not be swabbed with alcohol for immunocompetent children in field sessions (MoHFW guidance), though a clean, dry skin surface is adequate. Never aspirate — the WHO (2015) and IAP advise against aspiration before injection for immunization (it increases pain, tissue trauma, and procedure time without benefit at recommended anatomical sites where major vessels are not present).
SELF-CHECK
A health worker is about to administer DPT to a 10-week-old infant. She checks the VVM and finds it has turned to stage 3 (the inner square is the same colour as the outer ring). What should she do?
A. Administer the vaccine — the VVM stage 3 indicates the cold chain was briefly interrupted but the vaccine is still potent
B. Discard the vial and obtain a new one — VVM stage 3 indicates the discard point has been reached
C. Shake the vial vigorously and administer — agitation restores potency
D. Store the vial in the freezer and administer at the next session
Reveal Answer
Answer: B. Discard the vial and obtain a new one — VVM stage 3 indicates the discard point has been reached
VVM stage 3 (inner square matches outer ring) is the DISCARD POINT — the vaccine has been exposed to sufficient heat to potentially reduce potency and must not be used. VVM stage 4 (inner square darker than outer ring) also means discard. Only stages 1 and 2 are acceptable for use. Shaking and refreezing do not restore heat-damaged vaccines.
Route and Site Selection for UIP Vaccines
Selecting the correct anatomical site and injection route is one of the highest-stakes technical decisions in vaccine administration. An error here can cause a local abscess, inadvertent nerve injury (e.g. sciatic nerve injury from gluteal injection — a never-event in paediatric immunization), vaccine failure from subcutaneous deposition of an IM vaccine, or a BCG keloid from deep injection. The governing principle is: match the route and site to the vaccine's formulation and the child's age. The route is determined by the vaccine's antigen and adjuvant composition — intramuscular delivery provides faster vascular uptake and reduced local reactogenicity for adjuvanted vaccines, while intradermal delivery exploits the high density of dendritic cells in the dermis for BCG's mycobacterial antigens, and subcutaneous delivery suits live-attenuated viral vaccines that replicate in the local lymph nodes. Getting the route wrong does not merely waste a dose; it can produce an exaggerated local reaction (IM vaccine given SC), inadequate immune priming (SC vaccine given IM), or a programme-error AEFI investigation.
Intramuscular (IM) injections:
IM vaccines are deposited into the muscle belly, which has a rich blood supply for rapid absorption and a low density of immune-sensitising cells that would cause local reactions. The preferred sites are:
- Anterolateral thigh (vastus lateralis muscle): the default site for ALL IM injections in infants (< 1 year). The muscle mass is largest at this site in infancy, and there are no major nerves or vessels at risk when the injection is given into the middle third of the lateral thigh. Use a 23–25 G needle, 16 mm (5⁄8 inch) length, 90° angle, inserting into the anterolateral aspect.
- Deltoid muscle (upper arm, 2–3 finger-breadths below the acromion): preferred for children ≥ 1 year, adolescents, and adults once the deltoid has adequate muscle mass. Use a 23–25 G needle, 16–25 mm length, 90° angle.
The gluteal region is CONTRAINDICATED as an injection site for vaccines in children — the gluteal muscles are poorly developed in infants, the sciatic nerve is at risk, and vaccine absorption is suboptimal from the fatty layer overlying the gluteus in infants.
Subcutaneous (SC) injections:
SC vaccines (MR, MMR, varicella, JE live) are deposited into the subcutaneous tissue at 45°. Site: right upper arm (or anterolateral thigh in infants). Use a 25 G, 16 mm needle at 45°. The subcutaneous tissue tolerates these attenuated viral vaccines well; IM injection of SC vaccines causes unnecessary local reactions.
Intradermal (ID) injections:
BCG is given intradermally into the dermis of the right deltoid region (just below the attachment of the deltoid muscle on the right arm). Volume: 0.05 mL in neonates (< 1 month), 0.1 mL in older infants and children. Use a 26 G, 10 mm needle at a 15° angle, bevel facing upward, inserted parallel to the skin surface. A correct ID injection produces a bleb (small raised wheal, 5–7 mm diameter) — if no bleb forms, the injection was likely IM and the dose is lost. BCG should be given to the right arm ONLY for standardisation (facilitates scar identification at school entry screening).
Oral and other routes:
OPV is given orally — 2 drops from the dropper bottle directly onto the tongue. If the child spits out the dose within 30 seconds, the dose should be repeated. Rotavirus vaccine is given orally (0.5–1.5 mL depending on brand, directly into the mouth). Nasal influenza vaccine (if used) is administered as one spray per nostril with a special device.
| Vaccine | Route | Site | Needle | Volume |
|---|---|---|---|---|
| BCG | ID | Right deltoid region | 26 G, 10 mm, 15° | 0.05 mL (neonate) / 0.1 mL (older) |
| Hep-B birth | IM | Anterolateral thigh | 23–25 G, 16 mm, 90° | 0.5 mL |
| OPV | Oral | Mouth (tongue) | Dropper | 2 drops |
| Pentavalent | IM | Anterolateral thigh (< 1 yr) | 23–25 G, 16 mm, 90° | 0.5 mL |
| fIPV | ID | Right anterolateral thigh | 26 G, 10 mm, 15° | 0.1 mL (fractional) |
| Rotavirus | Oral | Mouth | Oral applicator | Per brand |
| MR/MMR | SC | Right upper arm | 25 G, 16 mm, 45° | 0.5 mL |
| JE (live) | SC | Right upper arm | 25 G, 16 mm, 45° | 0.5 mL |
| PCV | IM | Anterolateral thigh | 23–25 G, 16 mm, 90° | 0.5 mL |
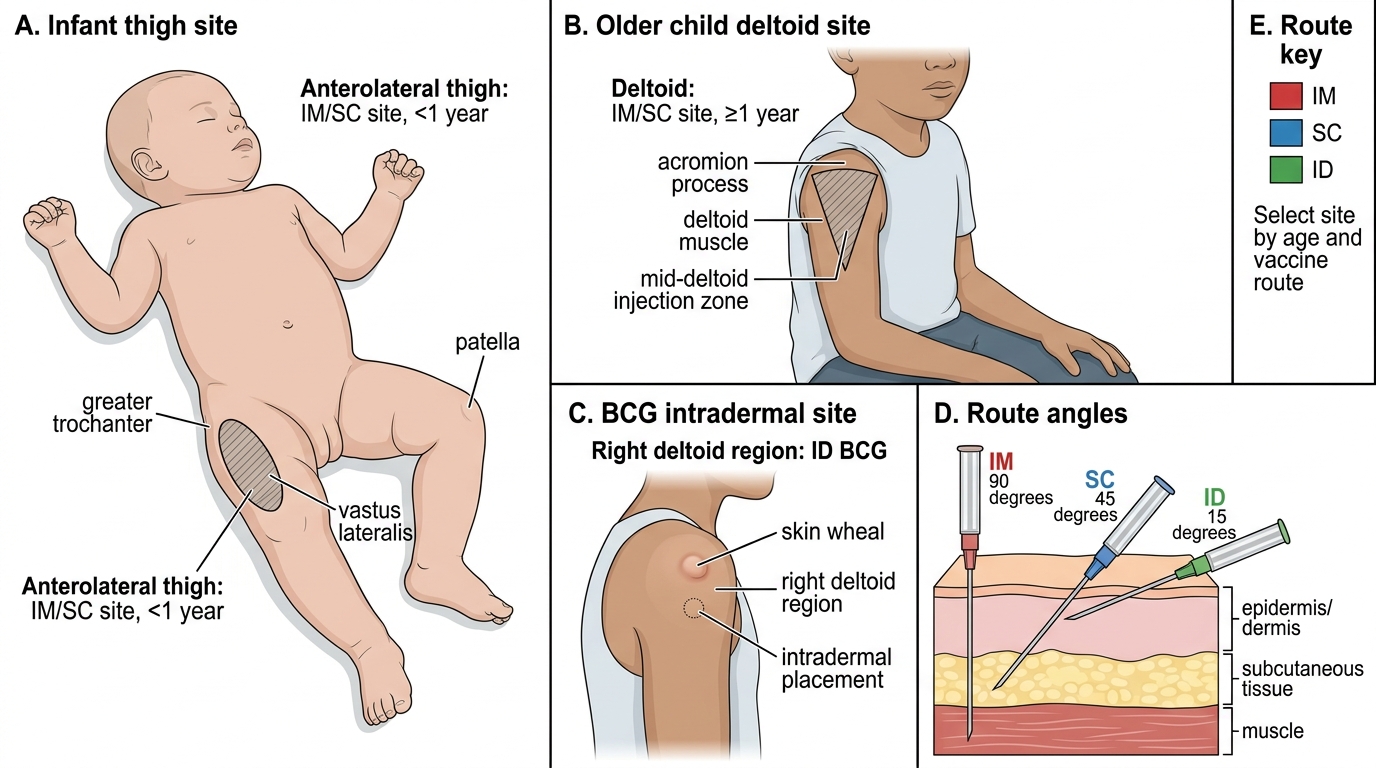
Vaccine Injection Sites and Route Angles in Children