Page 1 of 26
PE18.1-2 | UIP Framework and Vaccine Preventable Disease Epidemiology — SDL Guide
Learning Objectives
- Explain the historical evolution, structure, and components of India's Universal Immunization Program (UIP) and National Immunization Program (NIP)
- Describe the National Immunization Schedule (NIS) 2023: vaccines, target ages, routes, and doses
- Explain the epidemiology of major vaccine preventable diseases (VPDs) covered under the UIP, including disease burden, R0 values, and transmission
- Describe the mechanisms underpinning programme effectiveness: herd immunity thresholds, cold chain requirements, and coverage determinants
- Explain programme impact, surveillance systems, AEFI classification and reporting, and India's eradication/elimination milestones
INSTRUCTIONS
Immunisation is the single most cost-effective public health intervention available in paediatric practice. India's Universal Immunization Program reaches ~27 million infants annually, and understanding its structure, schedule, and epidemiological rationale is essential for every clinician — both to counsel families accurately and to recognise gaps in a child's immunisation status during any clinical encounter. This module equips you to apply that knowledge at the bedside and in community health settings.
References
- Ghai Essential Pediatrics, 9th edition, Chapters on Immunization and Preventive Pediatrics (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Chapter on Active Immunization (textbook)
- IAP Advisory Committee on Vaccines and Immunization Practices (ACVIP) Recommended Immunization Schedule 2023 (guideline)
- India National Immunization Schedule (NIS) 2023 — Ministry of Health and Family Welfare / NHM (program)
- WHO Immunization in Practice 2015, Module 6 (Surveillance of AEFI) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-month-old boy is brought to the district hospital with high fever, cough, coryza, and a diffuse maculopapular rash that began behind the ears two days ago and spread downward. His mother reports that she never took him for any injections — the nearest PHC is 8 km away and she could not arrange transport. On examination, Koplik's spots are visible on the buccal mucosa. The ward physician notes that three other children with similar presentations have been admitted in the past week from the same village. On inquiry, the local ASHA worker confirms that immunisation coverage in that village dropped to below 50% during the last two years. The outbreak is measles — a disease that should not exist in a well-vaccinated community.
This case is not just about one child with measles. It is about a system failure: the Universal Immunization Program exists precisely to prevent this chain of events. Understanding why outbreaks like this happen, and how the programme is designed to prevent them, is one of the most important things you will learn in paediatric public health.
WHY THIS MATTERS
As a final-year student and future clinician, you will encounter under-vaccinated children in every setting — outpatient clinics, ward admissions, IMNCI assessments, and community health postings. Immunisation status is a mandatory check in every paediatric encounter. Beyond the individual child, the paediatrician is a frontline advocate for community immunity — understanding herd immunity thresholds, the National Immunization Schedule, and how to counsel hesitant families are core competencies that directly protect child lives. India's VPD burden is still substantial: measles, rotavirus diarrhoea, pertussis, and neonatal tetanus continue to cause preventable deaths, disproportionately in children under five in low-coverage districts. The NMC CBUC competencies PE18.1 and PE18.2 reflect this reality by placing UIP structure and VPD epidemiology at the heart of paediatric training.
RECALL
Before engaging with this module, consolidate the following from your Year 1 and Year 2 foundations:
- Vaccine immunology (Microbiology / Immunology): Live-attenuated vaccines (BCG, OPV, MR, rotavirus, JE live) generally produce stronger and more durable immunity but carry a small risk of reversion or contraindication in immunosuppressed individuals. Killed/inactivated vaccines (IPV, Hep-B, Hib conjugate, DPT) are safer but may require more doses or booster schedules. Toxoid vaccines (diphtheria, tetanus toxoids in pentavalent) work by neutralising the pathogen's exotoxin, not the organism itself.
- Epidemiology basics (Community Medicine): R0 (basic reproduction number) = average number of secondary cases from one index case in a fully susceptible population. Herd immunity breaks the chain of transmission when a sufficient proportion of the population is immune. You will now apply this to specific VPDs.
- IMNCI danger signs (PE-skills arc): The IMNCI checklist includes verification of immunisation status at every contact — reinforcing that immunisation is integrated into clinical care, not siloed in preventive programmes.
Why Immunisation Is the Paediatrician's Most Powerful Tool
Vaccine preventable diseases collectively killed an estimated 1.5 million children globally each year before widespread immunisation, with the burden concentrated in low- and middle-income countries. India bore a disproportionate share: in the pre-vaccine era, smallpox, polio, and measles caused hundreds of thousands of childhood deaths annually. The introduction of systematic immunisation programmes has been described as the greatest public health achievement of the 20th century, second only to clean water and sanitation in its impact on child survival.
In the Indian context, vaccination transitions from a clinical tool to a programmatic intervention — a national public-goods delivery system that must reach every child, including those in remote, tribal, and underserved geographies. This distinction matters for the paediatrician: while prescribing is an individual act, immunisation advocacy is a population-level responsibility. When a child presents with a VPD, the clinician's first question should not only be 'how do I treat this child?' but also 'why was this child not protected, and are there other unprotected children in this community?'
The Universal Immunization Program (UIP) is India's flagship preventive paediatric intervention, targeting 27 million infants and 30 million pregnant women annually across all states and union territories. It sits within the National Health Mission (NHM) / Reproductive and Child Health (RCH) programme framework, and its success is measured by full immunisation coverage (FIC) — the proportion of children aged 12-23 months who have received all scheduled vaccines. India's FIC rose from approximately 43% (NFHS-3, 2005-06) to 76% (NFHS-5, 2019-21), a dramatic improvement driven largely by Mission Indradhanush and intensified routine immunisation.
| Milestone | Year | Significance |
|---|---|---|
| Expanded Program on Immunization (EPI) | 1978 | India joins WHO global initiative; 6 diseases targeted |
| Universal Immunization Program (UIP) | 1985 | Expanded nationwide; goal = universal coverage |
| Pulse Polio Campaign | 1995–2014 | National Immunization Days; 172+ million children/round |
| Hepatitis B added to UIP | 2002 (phased) | National rollout by 2011 |
| Mission Indradhanush | 2014–present | Target zero-dose/under-vaccinated children; intensified rounds |
| India declared polio-free | April 2014 | WHO certification after 3 years without wild poliovirus |
| MR Campaign | 2017–2019 | Nationwide MR catch-up for 9 mo – <15 yr |
Understanding UIP as a programme delivery system (not just a vaccine list) positions the clinician to identify systemic gaps — lack of cold chain, missed sessions, vaccine hesitancy, migration — that produce clusters of unvaccinated children like the measles outbreak in the hook.
VPD Epidemiology: Burden, Transmission, and Disease Profile
Vaccine preventable diseases are defined operationally as infections against which licensed, effective vaccines exist and which are included in national schedules. India's UIP currently targets 12 diseases: tuberculosis, poliomyelitis, diphtheria, pertussis, tetanus (neonatal + childhood), hepatitis B, Haemophilus influenzae type b (Hib) disease, measles, rubella, rotavirus diarrhoea, Japanese encephalitis, and pneumococcal disease (the latter two in select states and districts under the national programme). Understanding the epidemiology of each — its mode of transmission, incubation period, pre-vaccine burden, and the rationale for vaccination — is essential for counselling families and for recognising outbreak patterns.
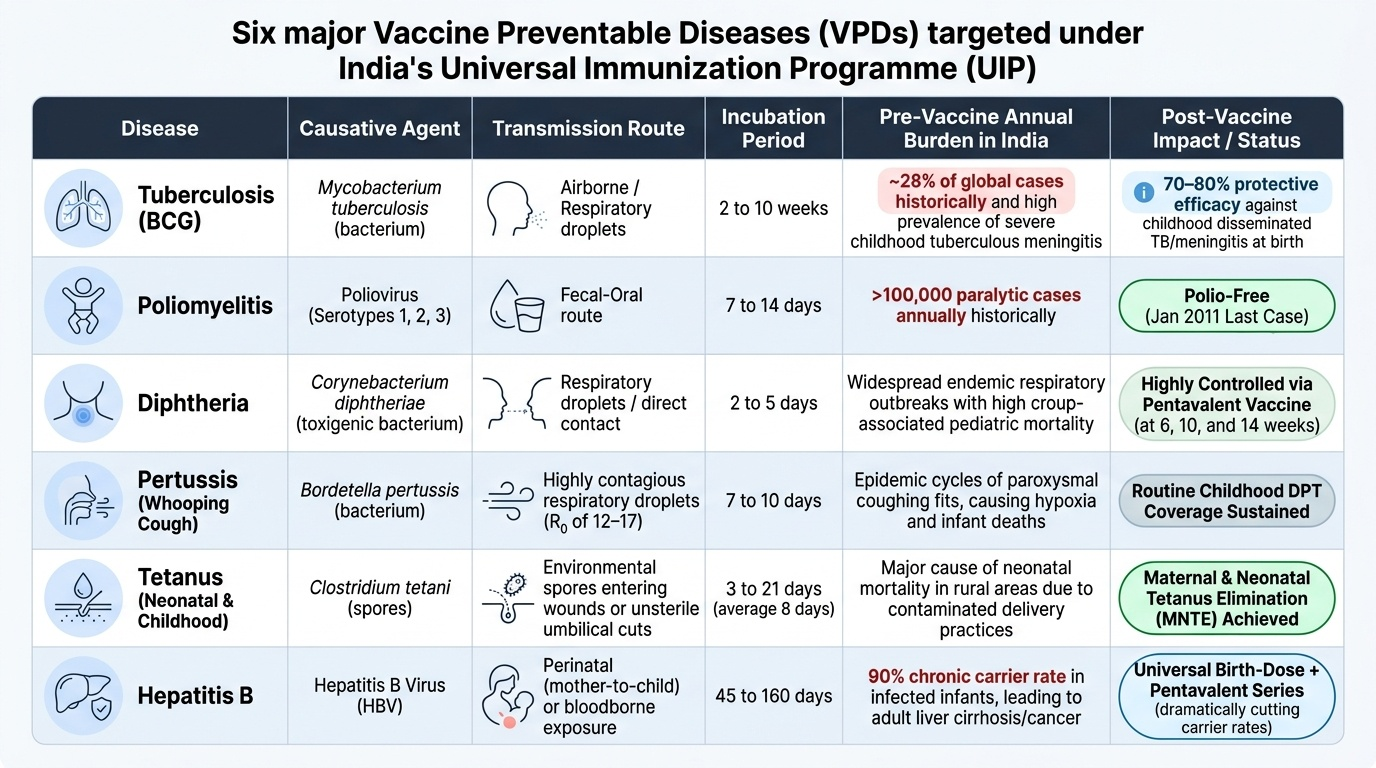
Provided image
Tuberculosis (BCG): Despite BCG, India has the highest TB burden globally (~28% of global cases). BCG at birth targets severe childhood forms — disseminated TB and tuberculous meningitis — where efficacy is 70-80%, while its protection against pulmonary TB in adults is variable. The window period for BCG is birth to 1 year; after 1 year, intradermal BCG is given if not received, but efficacy for meningeal/miliary TB is lower when delayed.
Poliomyelitis (OPV/IPV): Poliovirus (types 1, 2, 3 — enterovirus family) spreads by faeco-oral route. Pre-vaccine India reported >100,000 paralytic polio cases annually. Wild poliovirus type 2 was eradicated globally in 1999; type 3 in 2019; India's last wild poliovirus case was in January 2011, and WHO certification of polio-free status came in April 2014. The NIS now uses fIPV (fractional intradermal IPV) at 6 and 14 weeks alongside OPV, ensuring protection against all three serotypes, including type 2 (for which mOPV2 is no longer in routine use).
Diphtheria, Pertussis, Tetanus: Diphtheria is an upper respiratory tract toxigenic infection (Corynebacterium diphtheriae); pertussis is a highly contagious catarrhal–paroxysmal cough (Bordetella pertussis, R0 12-17, among the highest known pathogens); neonatal tetanus remains a cause of neonatal death in unvaccinated populations. All three are targeted by the pentavalent vaccine (DPT + Hep-B + Hib conjugate) at 6, 10, and 14 weeks.
Hepatitis B: Perinatally acquired HBV progresses to chronic carrier state in 90% of infants infected at birth, versus <5% in adults — making birth-dose vaccination critical. The NIS birth dose within 24 hours interrupts this perinatal transmission route. Horizontal transmission in early childhood is the other major route in India.
Haemophilus influenzae type b (Hib): A leading cause of bacterial meningitis and epiglottitis in children under 5. Hib conjugate vaccine (included in pentavalent) has reduced Hib meningitis by >90% in countries with high coverage. Hib disease is more severe in the first 2 years of life, justifying the 6/10/14-week primary series.
Measles and Rubella (MR): Measles (R0 12–18) is the most infectious respiratory pathogen known, making it the sentinel VPD for herd immunity thresholds. Pre-vaccine India: ~1 million measles deaths/year. Rubella causes congenital rubella syndrome (CRS) — cataracts, cardiac defects, sensorineural deafness — when infection occurs in the first trimester. The MR campaign (2017–19) targeted immunity gaps from birth-cohort-only vaccination.
Rotavirus: Leading cause of severe diarrhoeal dehydration in children under 5 globally; India accounts for ~23% of global rotavirus deaths. Fomite and faeco-oral spread; very low infectious dose. The rotavirus oral vaccine series (6/10/14 weeks in NIS) has reduced rotavirus-associated hospitalisations by ~40-60% in high-coverage settings.
Japanese Encephalitis (JE): Zoonotic flaviviral encephalitis transmitted by Culex mosquitoes, endemic in at least 24 Indian states (UP, Bihar, Assam, West Bengal, Tamil Nadu most affected). R0 varies by vector density; 20-30% mortality, 30-50% of survivors have neurological sequelae. JE vaccine (SA-14-14-2 live-attenuated or inactivated) is in NIS for endemic districts.
| VPD | Causative Agent | R0 | Herd Immunity Threshold |
|---|---|---|---|
| Measles | Paramyxovirus | 12–18 | 92–95% |
| Pertussis | Bordetella pertussis | 12–17 | ~92–94% |
| Polio | Enterovirus (types 1–3) | 5–7 | ~80–85% |
| Mumps | Paramyxovirus | 4–7 | ~75–86% |
| Diphtheria | Corynebacterium diphtheriae | 6–7 | ~83–85% |
| Hepatitis B | HBV | 2–4 (perinatal) | ~67–75% |
Structure of India's Universal Immunization Program (UIP) and National Immunization Schedule
The Universal Immunization Program (UIP) is implemented through the National Health Mission (NHM) under the Ministry of Health and Family Welfare. The programmatic chain runs from the national Cold Chain Point (CCP) at national level through state, regional, and district vaccine stores, down to the Primary Health Centre (PHC), sub-centre, and outreach session site — where the Auxiliary Nurse Midwife (ANM) is the primary vaccinator. The ASHA (Accredited Social Health Activist) and anganwadi worker play demand-generation roles, mobilising families and ensuring session attendance.
The National Immunization Schedule (NIS) 2023 is the authoritative Indian document for vaccine timing. It is not the same as the IAP Advisory Committee on Vaccines and Immunization Practices (ACVIP) recommended schedule, which also includes vaccines not yet in the government programme (e.g. chickenpox, typhoid conjugate, 6-in-1). For NMC/NIS examination purposes, the government NIS is the reference.
The NIS 2023 by age-point is:
At birth (within 24–72 hours):
- BCG — intradermal 0.05 mL (left deltoid) — tuberculosis
- OPV-0 — 2 drops oral — polio (first contact dose, birth dose)
- Hepatitis B (HepB-0) — 0.5 mL IM (anterolateral thigh) — within 24 hours for maximum perinatally-acquired HBV prevention
At 6 weeks (42 days):
- Pentavalent 1 (DPT + HepB + Hib) — 0.5 mL IM anterolateral thigh
- OPV-1 — 2 drops oral
- Rotavirus 1 — oral liquid
- fIPV-1 — 0.1 mL intradermal (right anterolateral thigh)
At 10 weeks (70 days):
- Pentavalent 2 — 0.5 mL IM
- OPV-2 — 2 drops oral
- Rotavirus 2 — oral liquid
At 14 weeks (98 days):
- Pentavalent 3 — 0.5 mL IM
- OPV-3 — 2 drops oral
- Rotavirus 3 — oral liquid
- fIPV-2 — 0.1 mL intradermal
At 9–12 months:
- MR 1 (Measles-Rubella) — 0.5 mL SC
- JE 1 — in endemic districts — 0.5 mL SC
- Vitamin A 1st dose — 1 lakh IU oral (at 9 months with MR)
At 16–24 months:
- MR 2 — booster
- DPT booster 1 — 0.5 mL IM
- OPV booster — 2 drops oral
- JE 2 — endemic districts
- Vitamin A 2nd dose onward every 6 months until 5 years
At 5–6 years:
- DPT booster 2 — 0.5 mL IM (school entry)
Vaccine types in the NIS:
- Live-attenuated: BCG, OPV, MR, Rotavirus, JE (SA-14-14-2 live-attenuated strain in endemic districts)
- Killed/inactivated: fIPV (inactivated poliovirus — all 3 serotypes), Hepatitis B
- Toxoid: DPT (diphtheria and tetanus are toxoids; pertussis is whole-cell killed)
- Conjugate: Hib conjugate (polysaccharide conjugated to carrier protein — essential for T-cell dependent response in infants <2 years)
The NIS operates through fixed-site sessions (PHC/sub-centre) and outreach sessions (village sites) on a schedule of typically 2 sessions per month per sub-centre. The Intensified Mission Indradhanush (IMI) targets zero-dose and under-vaccinated children through special catch-up campaigns, particularly in high-risk (urban slums, migrant, tribal, hard-to-reach) populations.
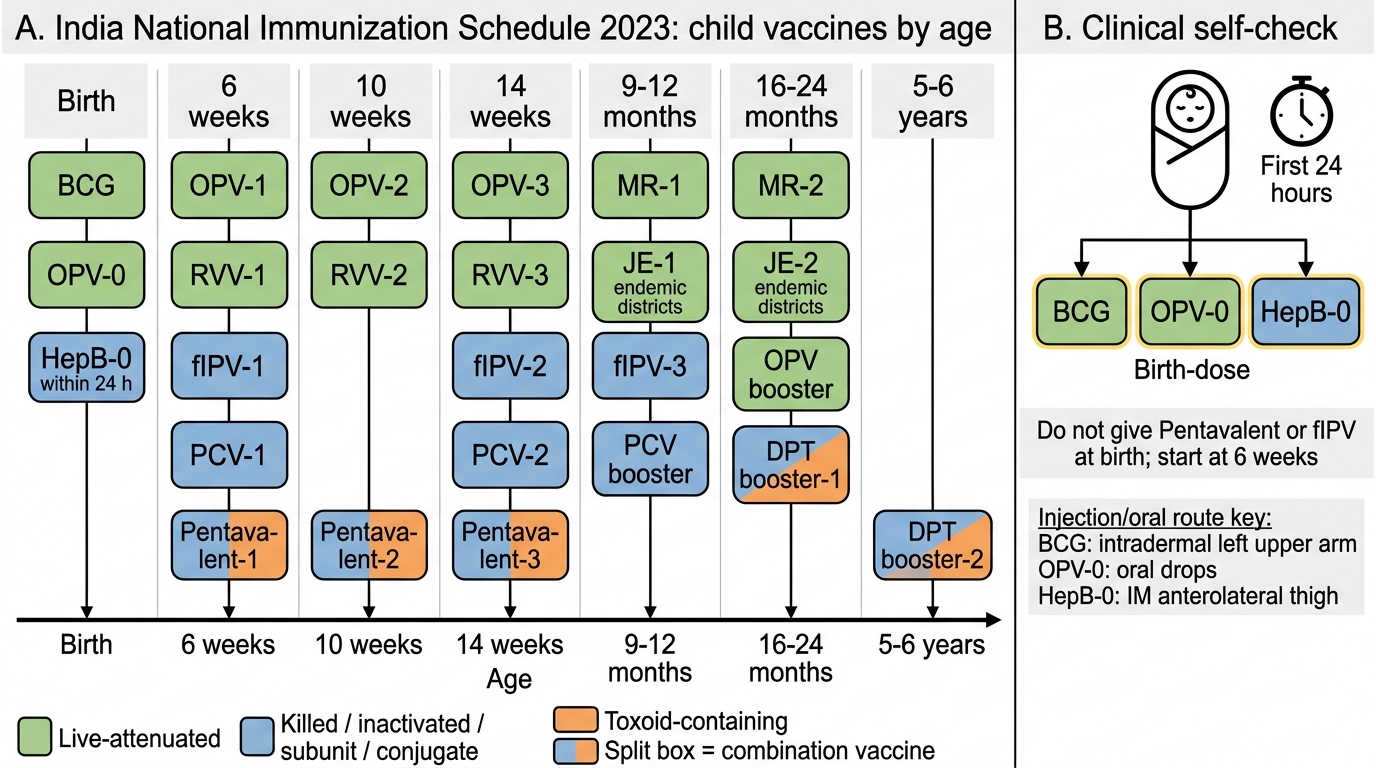
India National Immunization Schedule 2023
SELF-CHECK
A healthy newborn is delivered at a district hospital. The mother has unknown hepatitis B status. Which vaccines should be given within the FIRST 24 hours according to the India NIS 2023?
A. BCG + OPV-0 only
B. BCG + OPV-0 + Hepatitis B (HepB-0)
C. Pentavalent 1 + OPV-0 + BCG
D. HepB-0 + fIPV-1 + BCG
Reveal Answer
Answer: B. BCG + OPV-0 + Hepatitis B (HepB-0)
The India NIS 2023 birth-dose vaccines are BCG (intradermal, left deltoid), OPV-0 (oral), and Hepatitis B-0 (within 24 hours IM anterolateral thigh). Pentavalent and fIPV are given at 6 weeks, not at birth. The HepB birth dose within 24 hours is critical for preventing perinatally-acquired HBV, which progresses to chronic carrier state in ~90% of vertically-infected infants.