Page 4 of 26
PE18.{3,6,14} | Vaccine Classification and Schedules — SDL Guide
Learning Objectives
- Classify vaccines by antigen type (live-attenuated, inactivated, toxoid, subunit, polysaccharide) with examples of each
- Recall the exact National Immunization Schedule (NIS) India — age, vaccine, dose, and route from birth through adolescence
- Prescribe an age-appropriate immunization schedule after assessing a child's fitness for vaccination
- Enumerate newer vaccines included in NIS or IAP schedule (pentavalent, PCV, rotavirus, JE, HepA, TCV, fIPV, HPV, influenza, COVID) and state their specific indications
- Describe common and serious AEFI, true versus false contraindications, and the risks and benefits of immunization
INSTRUCTIONS
Vaccine-preventable diseases remain a leading cause of under-5 morbidity and mortality in India. A clinician who cannot recall the exact NIS schedule, identify vaccine types, or recognise contraindications will either leave a child unprotected or unnecessarily withhold vaccines. This module equips you with the foundational knowledge — classification, schedule, newer vaccines, and safety — that underpins every paediatric consultation involving immunization.
References
- Ghai Essential Pediatrics, 9th edition, Chapter on Immunization (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Chapter on Immunization Practices (textbook)
- IAP Advisory Committee on Vaccines and Immunization Practices (ACVIP) Recommended Immunization Schedule 2024 (guideline)
- National Immunization Schedule (NIS) India 2023, MoHFW (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are a final-year student posted in the paediatric OPD. A mother walks in with her 14-month-old son who has never received any vaccines — the family relocated repeatedly and lost the immunization card. She asks: 'Doctor, can he still get his shots? Which ones does he need now?' You realise you need to know not just which vaccines exist, but their exact schedule, classification, and whether it is safe to catch up after a gap. Getting this wrong means a child remains unprotected against measles, diphtheria, or hepatitis B — diseases that kill or permanently disable thousands of Indian children each year.
WHY THIS MATTERS
Understanding vaccine classification lets you predict behaviour — live vaccines shed virus, require cold chain, and are contraindicated in immunodeficiency; inactivated vaccines are safe in pregnancy and immunocompromised hosts. The NIS schedule encodes decades of epidemiological evidence about the optimal age for each vaccine; deviating from it without reason compromises protection. As a clinician you will encounter children with missed doses, children with special conditions (HIV, prematurity, asplenia), and parents with genuine fears — all of which require a firm factual scaffold to manage confidently.
RECALL
Before proceeding, recall from Year 1 Physiology and Biochemistry: the adaptive immune response involves B-lymphocytes that produce antigen-specific antibodies and long-lived memory cells. T-helper cells support this response. Vaccines work by exposing the immune system to an antigen (or an attenuated/killed pathogen) without causing disease, thereby generating immunological memory so that future encounter with the real pathogen triggers a rapid, protective secondary response. The concept of herd immunity — protection of unvaccinated individuals when enough of the population is immune — explains why high coverage rates matter at the community level, not only for the individual child.
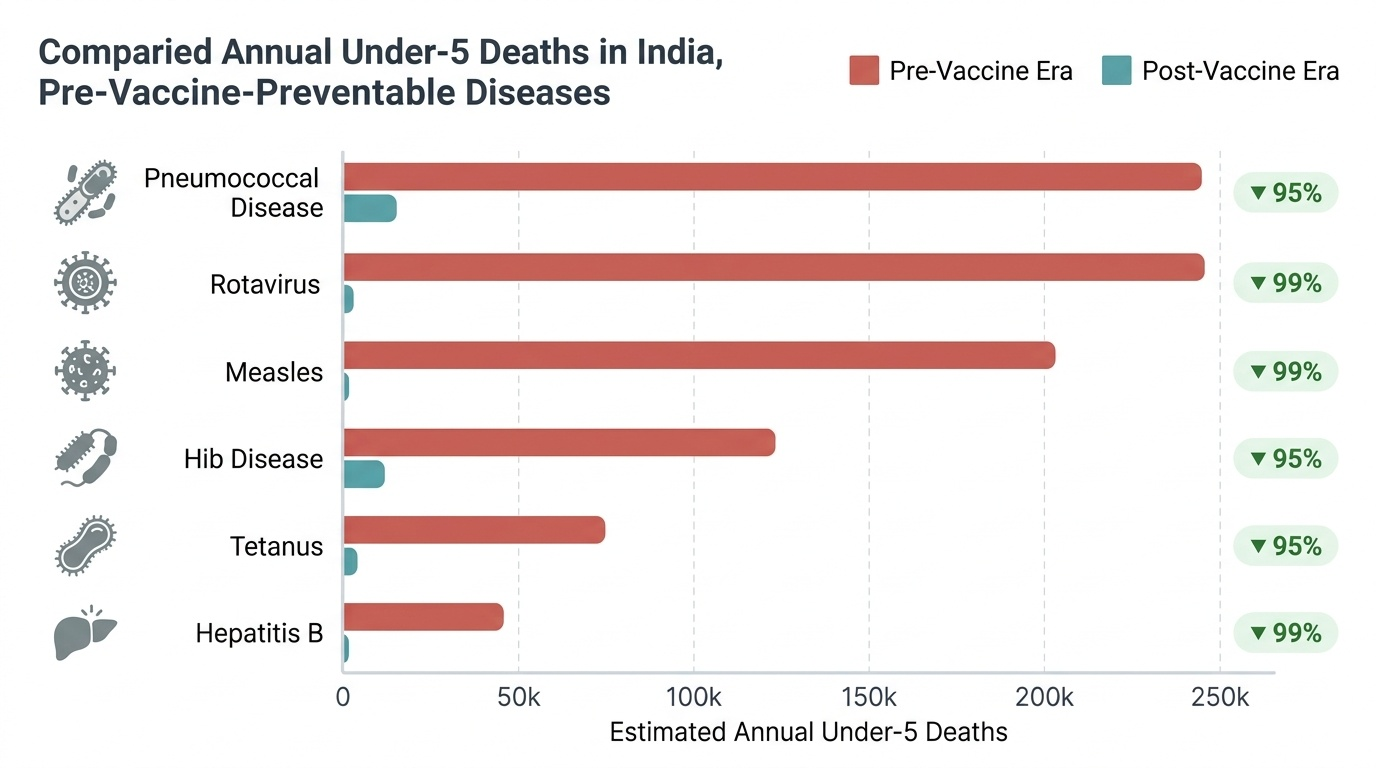
Why Immunization Matters: Disease Burden and the Role of Vaccines
Vaccine-preventable diseases (VPDs) continue to impose an enormous health burden on children in India and globally, despite dramatic progress over the past five decades. Measles alone caused over 140,000 global deaths in 2018 (WHO), with India accounting for a significant proportion; neonatal tetanus, once a leading killer, has been nearly eliminated in India through maternal TT immunization and clean delivery practices; and poliomyelitis has been eradicated from India as of 2014, a direct result of intensive OPV campaigns. Diphtheria, pertussis, hepatitis B, Haemophilus influenzae type b (Hib) meningitis, rotavirus gastroenteritis, and pneumococcal pneumonia collectively account for millions of episodes of severe illness and hundreds of thousands of preventable deaths annually in the under-5 age group across low- and middle-income countries.
Provided image
Vaccines confer protection through two mechanisms: direct protection of the immunized individual via humoral and cell-mediated immunity, and indirect (herd) protection of unimmunized or inadequately immunized individuals when vaccination coverage in the community reaches a critical threshold. For measles, this herd immunity threshold is approximately 92–95%, which is why even a small drop in coverage can trigger outbreaks among susceptible clusters. Understanding this epidemiological context explains why the NIS is designed as a population-level programme and why maintaining high coverage — not just vaccinating individual patients in your OPD — is a professional responsibility.
The burden of VPDs is highest in the first two years of life when passively acquired maternal antibodies wane (typically by 3–6 months) and the child's own adaptive immunity is maturing. This window of vulnerability is precisely why the NIS front-loads its primary series in the first 14 weeks of life and schedules boosters at 16–24 months and 5–6 years to reinforce waning immunity.
As a clinician, framing immunization as a cornerstone of preventive paediatrics — not an administrative task — is the attitudinal foundation on which every subsequent clinical decision about vaccines rests.
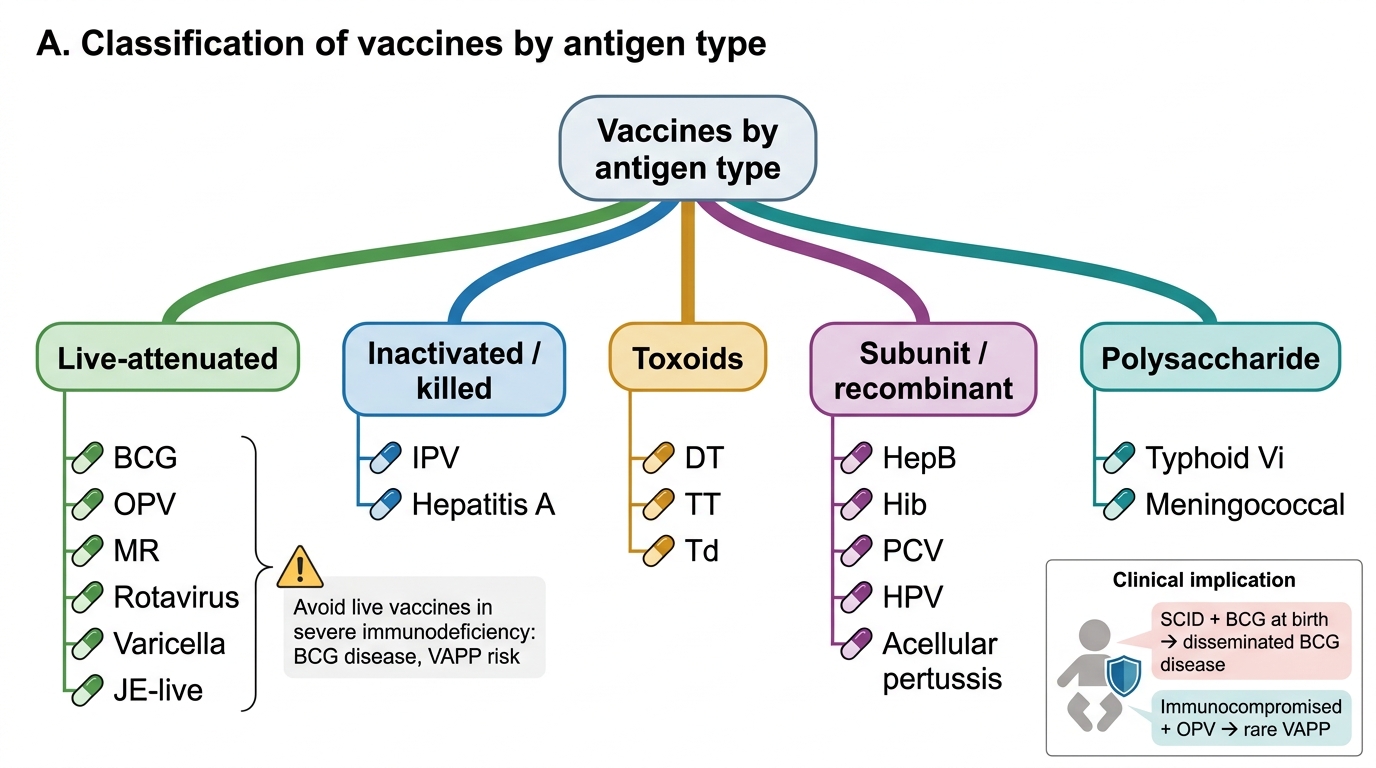
Classification of Vaccines
Vaccines are classified by the nature of the antigen they present to the immune system. This classification is clinically important because it determines storage requirements, contraindication profiles, and the immune response pattern (single-dose vs multi-dose for primary immunity, need for adjuvants, duration of protection).
Live-attenuated vaccines contain viable, weakened pathogens that replicate in the host and stimulate a robust, long-lasting immune response closely mimicking natural infection. Because the organism replicates, a small inoculum (one or two doses) is usually sufficient for lifelong immunity. However, this replication also means that live vaccines can cause disease in immunocompromised hosts and are generally contraindicated in pregnancy and in children with primary immunodeficiency, HIV with low CD4 counts, or on immunosuppressive therapy. Examples in the NIS: BCG (Mycobacterium bovis — Calmette-Guérin strain), OPV (Sabin trivalent/bivalent oral poliovirus), MR/MMR (measles-rubella or measles-mumps-rubella), rotavirus (Rotarix, Rotavac — oral), JE live (SA 14-14-2 strain), and varicella.
Inactivated (killed) vaccines contain whole pathogens or their components that have been killed/inactivated and cannot replicate. They are safer in immunocompromised patients but generally require multiple doses (primary series) and boosters because the immune response is weaker than with live vaccines. Adjuvants (aluminium salts) are commonly added to enhance immunogenicity. Examples: IPV/fIPV (inactivated Salk poliovirus), hepatitis A (inactivated), whole-cell pertussis (historical; replaced by acellular in many countries).
Toxoid vaccines contain inactivated bacterial toxins (toxoids). They protect against the toxin-mediated effects of disease rather than infection per se. Examples: TT/Td (tetanus toxoid ± reduced-antigen diphtheria), DT (diphtheria-tetanus toxoid). The DPT/pentavalent vaccine combines toxoids with other components.
Subunit, recombinant, and conjugate vaccines present specific purified antigens (proteins or polysaccharides chemically conjugated to a protein carrier to enhance T-cell-dependent immunity in infants). These are highly safe and suitable for immunocompromised hosts. Examples: HepB (recombinant HBsAg), Hib (polysaccharide conjugated to protein — in pentavalent), PCV13 (13-valent pneumococcal conjugate vaccine), HPV (recombinant virus-like particles — bivalent/quadrivalent/nonavalent), acellular pertussis (aP, used in some combination vaccines).
Polysaccharide vaccines (plain, unconjugated) stimulate T-cell-independent B-cell responses and are poorly immunogenic in children under 2 years. They are not part of the routine NIS paediatric schedule but are used in specific situations. Examples: typhoid Vi polysaccharide (for children ≥2 years; replaced in NIS by typhoid conjugate vaccine TCV), meningococcal plain polysaccharide (limited use; conjugate preferred).
Classification of Vaccines by Antigen Type
Key clinical implication of classification: If a child is found to have primary immunodeficiency after receiving BCG at birth, BCG disease (local or disseminated) can occur — a serious complication. Similarly, OPV-associated polio (vaccine-associated paralytic poliomyelitis, VAPP) can rarely occur in immunocompromised recipients of OPV — one reason fIPV has replaced type-2 OPV in the NIS and why IPV is preferred in immunocompromised hosts.
SELF-CHECK
A 6-week-old infant with X-linked severe combined immunodeficiency (SCID) is brought for routine immunization. Which NIS vaccine given at birth could cause disseminated disease in this infant?
A. Hepatitis B vaccine
B. BCG
C. IPV (injected polio)
D. Tetanus toxoid
Reveal Answer
Answer: B. BCG
BCG is a live-attenuated mycobacterial vaccine. In immunocompromised hosts (SCID, DiGeorge syndrome, HIV with low CD4), the live organism can replicate unchecked and cause local BCG disease, regional lymphadenitis, or fatal disseminated BCG infection. Hepatitis B (subunit), IPV (inactivated), and tetanus toxoid are all non-live and safe even in immunocompromised patients.
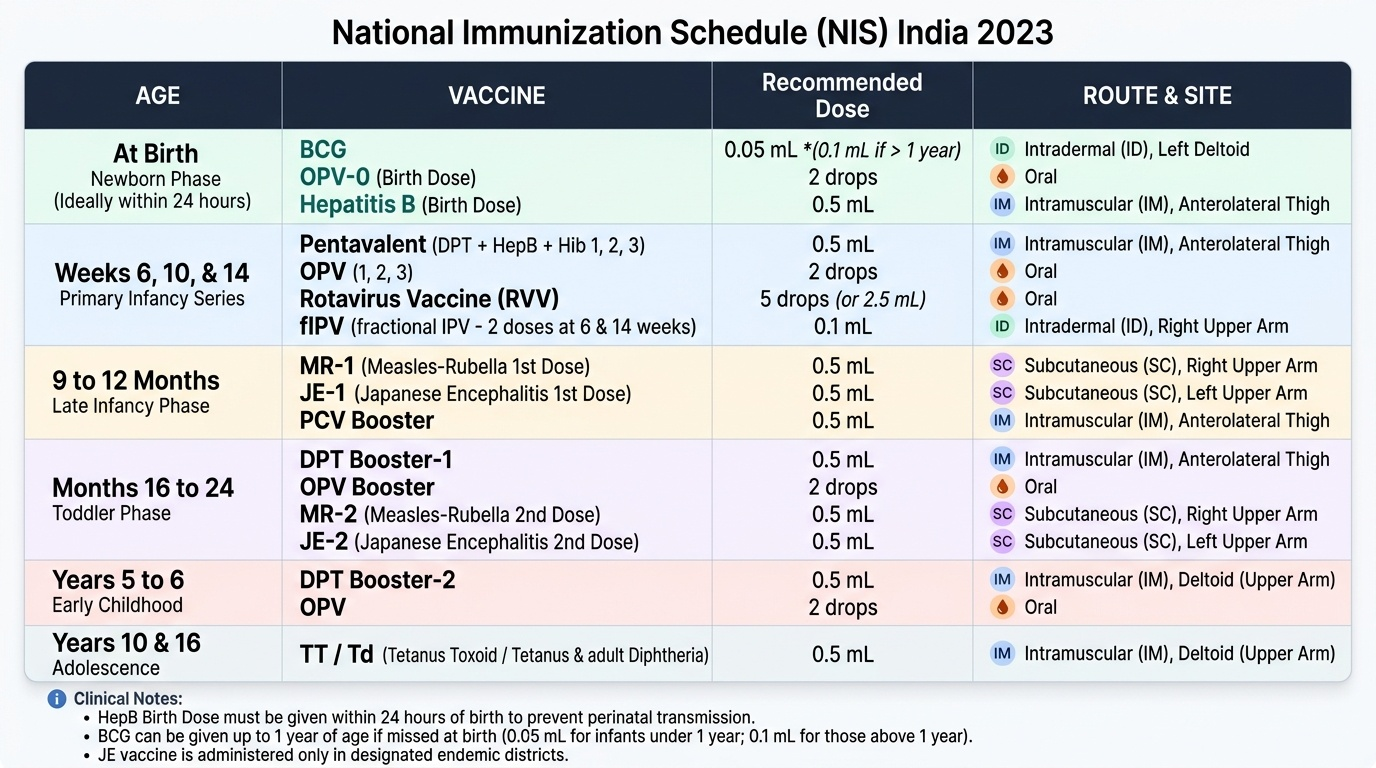
National Immunization Schedule (NIS) India
The National Immunization Schedule (NIS) India is the Government of India's official schedule for free vaccines under the Universal Immunisation Programme (UIP). As a clinician you must know this schedule exactly — the age, vaccine name, dose, and route — because deviations without clinical justification leave children unprotected at the most vulnerable developmental windows. The NIS is a carefully designed, evidence-based timeline that matches vaccine administration to the age of maximum susceptibility and the stage of immunological maturity: front-loading the primary series in the first 14 weeks of life exploits the period before maternal antibodies wane, while booster doses at 16–24 months and 5–6 years reinforce immunity as passive protection fades and the child enters school with its attendant social-exposure risks. Memorising this schedule is not an exercise in rote learning — it is the clinical infrastructure on which every immunization consultation rests.
Provided image
The NIS schedule (current as of 2023) is organised by age:
At birth (within 24 hours, ideally in hospital):
• BCG — 0.05 mL intradermal, left deltoid region
• OPV-0 (birth dose) — 2 drops oral
• Hepatitis B (birth dose) — 0.5 mL intramuscular (anterolateral thigh)
The hepatitis B birth dose must be given within 24 hours of birth to interrupt perinatal transmission. BCG should ideally be given at birth but may be given up to 1 year; the dose is 0.05 mL for infants under 1 year and 0.1 mL for those above 1 year.
At 6 weeks, 10 weeks, and 14 weeks (primary series):
• Pentavalent (DPT + HepB + Hib) — 0.5 mL IM (3 doses)
• OPV (oral) — 2 drops (3 doses)
• Rotavirus vaccine — oral (2 or 3 doses depending on brand — Rotavac 3 doses; Rotarix 2 doses; give per schedule)
• fIPV (fractional inactivated poliovirus, intradermal) — 0.1 mL ID, at 6 weeks and 14 weeks (2 doses)
Note: fIPV (one-fifth the standard IPV dose, given intradermally at the right deltoid) replaced the type-2 component of OPV after the global withdrawal of monovalent OPV-2 in 2016, maintaining seroconversion while conserving vaccine supply.
At 9–12 months:
• MR (Measles-Rubella) — 0.5 mL subcutaneous (1st dose)
• JE (Japanese Encephalitis, live SA 14-14-2 strain) — 0.5 mL subcutaneous; in endemic districts only
• Vitamin A supplementation — 100,000 IU oral (1st dose at 9 months)
• PCV booster — if PCV was in the primary series (state/programme specific)
At 16–24 months (booster):
• DPT booster — 0.5 mL IM (1st booster)
• OPV booster — 2 drops oral
• MR-2 (2nd dose) — 0.5 mL subcutaneous
• JE-2 (2nd dose in endemic districts)
• Vitamin A — 200,000 IU oral (every 6 months from 18 months to 5 years)
At 5–6 years:
• DPT booster (2nd booster) — 0.5 mL IM
• OPV booster
At 10 years:
• TT/Td — 0.5 mL IM
At 16 years:
• TT/Td — 0.5 mL IM
Catch-up immunization: A child who has missed doses does NOT start the series from scratch for most vaccines (with some exceptions). The general principle is to continue from where the schedule was interrupted — the 'primary series' doses still count regardless of the interval between doses. However, doses given too early (before the minimum age or minimum interval) must be repeated. For children presenting after 12 months who have never been vaccinated, refer to the IAP catch-up schedule.