Page 9 of 53
PE19.4 | Birth Asphyxia — SDL Guide
Learning Objectives
- Describe the clinical presentation of birth asphyxia and hypoxic-ischaemic encephalopathy (HIE) in the neonatal period
- Identify the antenatal, intrapartum, and fetal risk factors that predispose to birth asphyxia
- Explain the pathophysiology of primary and secondary energy failure in HIE and the rationale for the 6-hour therapeutic window
- Apply the Sarnat staging system to classify HIE severity (Stage I, II, III)
- Describe the immediate management of birth asphyxia including resuscitation, supportive care, and seizure control
- State the eligibility criteria for and protocol of therapeutic hypothermia in moderate-severe HIE
INSTRUCTIONS
Birth asphyxia is one of the three leading causes of neonatal mortality and morbidity in India, accounting for approximately 23% of neonatal deaths. In survivors of severe asphyxia, hypoxic-ischaemic encephalopathy (HIE) is the principal cause of cerebral palsy, intellectual disability, and epilepsy. The introduction of therapeutic hypothermia has transformed the management of moderate-to-severe HIE — but only if initiated within 6 hours of birth. As a final-year MBBS student, you will be the first doctor to assess an asphyxiated neonate in many settings; your ability to recognise HIE severity using the Sarnat classification and make a timely referral or initiate cooling is genuinely life-altering for these infants.
References
- Ghai Essential Pediatrics, 9th ed., Ch 6 — Birth Asphyxia and HIE (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 120 — Hypoxia-Ischemia (textbook)
- Azzopardi DV et al. (TOBY Trial). NEJM 2008;359:1900-1907 (journal)
- Shankaran S et al. (NICHD Trial). NEJM 2005;353:1574-1584 (journal)
- NNF India — Management of Perinatal Asphyxia and HIE, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-week baby is born by emergency caesarean section for prolonged fetal bradycardia. The delivery team resuscitates the baby for 8 minutes with PPV before spontaneous breathing begins. The cord blood pH is 6.98 and base deficit is 18 mmol/L. At 2 hours of age, the neonatal team notices the baby is lethargic, hypotonic, has continuous sucking movements of the lips, and is not feeding. The neonatal registrar turns to you: 'Sarnat stage the baby. Is this baby eligible for cooling?' You have the clinical findings in front of you and 20 minutes before the 6-hour window closes. What do you decide — and what are the next steps?
WHY THIS MATTERS
Birth asphyxia causes approximately 800,000 neonatal deaths globally each year and is a leading cause of neurodisability in survivors. In India, it accounts for roughly 23% of neonatal deaths and is the most common cause of neonatal seizures and cerebral palsy. Unlike many neonatal conditions, moderate-to-severe HIE now has an evidence-based disease-modifying treatment — therapeutic hypothermia — that reduces death or major neurodisability by approximately 25–30% in eligible neonates. However, this treatment is time-critical: it must be initiated within 6 hours of birth, during the brief window between primary and secondary neural injury. A doctor who does not recognise HIE, does not know the Sarnat staging criteria, or does not know the 6-hour window will fail to initiate this treatment in time. This module provides the complete framework for recognition, staging, and management.
RECALL
Activate the following prior knowledge before proceeding. From pe11-neonatal-resuscitation: recall that birth asphyxia is the clinical event that makes neonatal resuscitation necessary; effective resuscitation reduces the depth and duration of asphyxia and may prevent or mitigate HIE. From pe11-normal-newborn: recall the APGAR score — a persistently low APGAR (≤3 at 5 minutes) is one of the clinical criteria used to diagnose birth asphyxia. From Physiology (PY): recall cerebral blood flow autoregulation, the role of ATP in neuronal ion pump maintenance, and the concept of ischaemia-reperfusion injury. These physiological principles directly explain the two phases of HIE injury (primary and secondary energy failure). From Pathology: recall the concepts of necrosis (acute ATP depletion) and apoptosis (delayed programmed cell death) — both occur in HIE, and therapeutic hypothermia primarily targets the secondary apoptotic phase.
Clinical Presentation of Birth Asphyxia
Birth asphyxia is defined as the failure of adequate gas exchange at or around the time of birth, leading to a combination of hypoxia (reduced oxygen delivery to tissues), hypercarbia (accumulation of carbon dioxide), and metabolic acidosis (lactate accumulation due to anaerobic metabolism). The clinical consequence of sustained asphyxia affecting the brain is hypoxic-ischaemic encephalopathy (HIE) — the spectrum of neurological injury ranging from transient irritability to coma and death.
The clinical presentation of birth asphyxia unfolds in two temporal phases. The immediate phase (birth to the first minutes) is characterised by the features that prompt resuscitation: the baby fails to breathe or only gasps at birth, has poor or absent muscle tone (floppy), is pale or centrally cyanosed, and has a heart rate below 100 bpm. The APGAR score quantifies this — a score of ≤3 at 5 minutes (persistent severe depression) is one of the accepted clinical criteria for birth asphyxia, alongside cord blood gas abnormalities. A normal APGAR at 1 minute does not exclude asphyxia that occurred earlier; conversely, a low 1-minute APGAR often improves with resuscitation without sequelae.
The encephalopathy phase (hours 2–48) is when the neurological injury from asphyxia becomes clinically manifest as HIE. The baby may have appeared to recover initially after resuscitation, only to deteriorate as the secondary energy failure cascade (described in the next section) causes neuronal death. The hallmark features of HIE are:
- Altered consciousness: hyperalertness (mild) → lethargy or stupor (moderate) → coma (severe)
- Tone abnormalities: hypertonia/jitteriness (mild) → hypotonia (moderate) → complete flaccidity (severe)
- Seizures: neonatal seizures typically begin within 6–24 hours of birth in moderate HIE; they may be subtle (lip smacking, cycling movements, eye deviation, apnoea) or overt (tonic/clonic)
- Autonomic dysfunction: tachycardia, pupillary abnormalities, temperature instability
- Feeding difficulty: absent or weak suck reflex
Systemic manifestations of birth asphyxia beyond the brain include: acute kidney injury (oliguria, haematuria), hepatic dysfunction (elevated transaminases), cardiomyopathy (poor contractility, tricuspid regurgitation on echo), NEC (gut ischaemia), coagulopathy (DIC), and adrenal haemorrhage. Multi-organ dysfunction portends a worse prognosis.
Causes and Risk Factors for Birth Asphyxia
Aetiology and Risk Factors for Birth Asphyxia
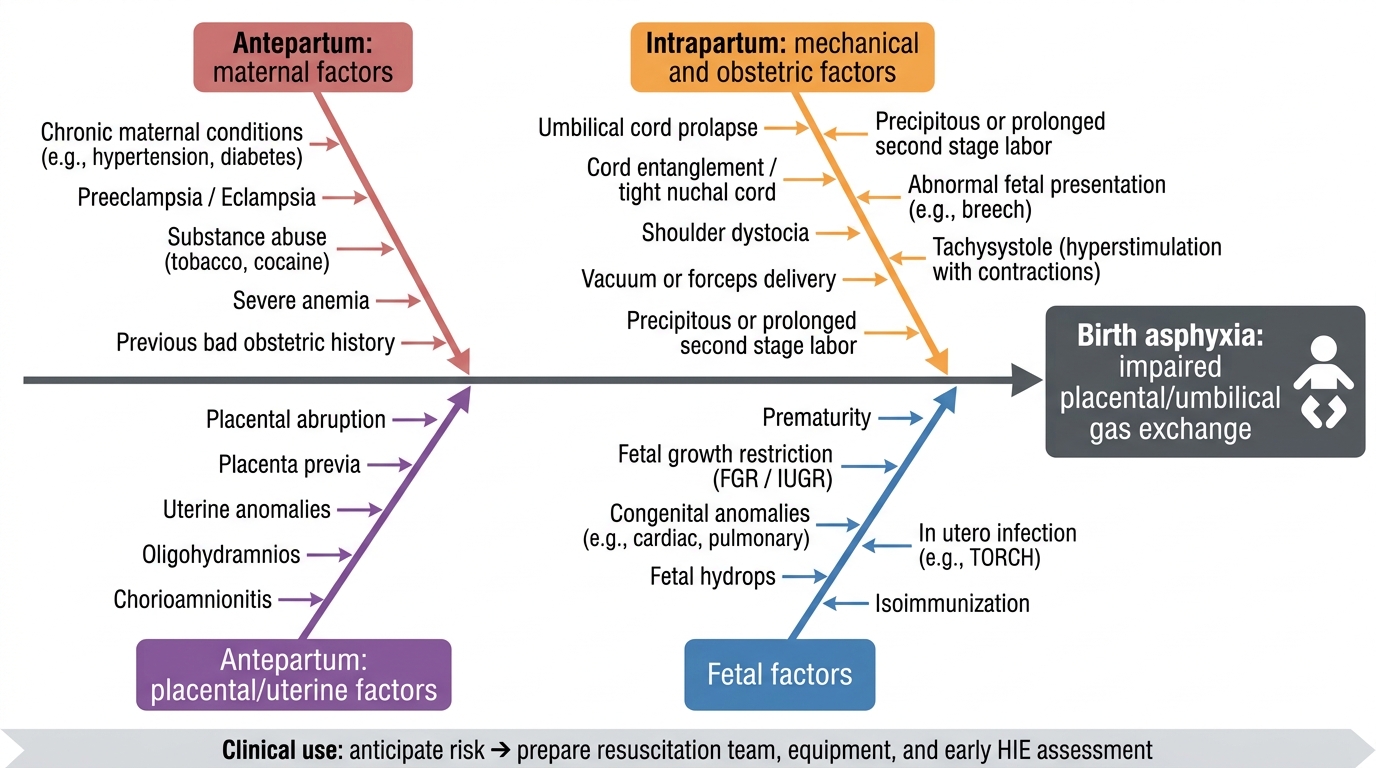
Birth asphyxia results from any event that interrupts or impairs placental/umbilical gas exchange in the peripartum period. Risk factors are conventionally categorised by their timing relative to labour, but the clinically critical point is that identifying risk factors before delivery allows the team to prepare — both for resuscitation and for early HIE assessment. This anticipatory approach is one of the most practical skills the clinician can develop: walking into a delivery room and mentally cataloguing whether the incoming baby has a high, moderate, or low probability of needing resuscitation determines whether experienced staff are present, equipment is tested and ready, and the neonatology team is pre-alerted. A team that is surprised by an asphyxiated neonate loses precious seconds; a team that anticipated the risk begins the golden minute from a position of preparedness. The three-category framework below — antepartum, intrapartum, neonatal — is not merely academic; it maps onto the clinical sequence of antenatal care, labour room monitoring, and delivery room readiness that collectively determine whether a baby experiences avoidable asphyxia.
Antepartum (pre-existing conditions that compromise fetal oxygenation):
- Maternal: pre-eclampsia/eclampsia, chronic hypertension, severe anaemia (Hb <7 g/dL), diabetes mellitus with poor control, cardiac or respiratory disease, infections (chorioamnionitis), drug abuse
- Placental: placental insufficiency leading to intrauterine growth restriction (IUGR), placenta praevia, abruptio placentae (sudden complete placental separation = worst scenario)
- Umbilical: cord around the neck (nuchal cord), true knot in cord
- Fetal: multiple gestation, severe fetal anaemia (Rh isoimmunisation), fetal hydrops, major congenital anomalies
Intrapartum (acute events during labour):
- Prolonged or obstructed labour (>18 hours)
- Precipitate delivery (fetal head compression)
- Cord prolapse — fetal head compresses the cord against the pelvis → complete occlusion of umbilical blood flow; a true obstetric emergency
- Uterine rupture
- Severe fetal bradycardia (Category III CTG) not acted upon promptly
- Thick meconium-stained amniotic fluid (MSAF) — a marker of fetal distress but also a risk for meconium aspiration syndrome
- General anaesthesia for operative delivery (maternal hypotension)
- Shoulder dystocia
Neonatal (post-delivery factors): prematurity (especially <34 weeks, immature lungs), respiratory distress syndrome, congenital heart disease, sepsis, severe anaemia.
In India, the most common contributors in community and district hospital settings are: absent or inadequate antenatal care, undetected IUGR, cord prolapse diagnosed late, and delay in operative delivery for fetal distress. Strengthening obstetric surveillance and timely delivery remains the most impactful preventive strategy.
Pathophysiology of Hypoxic-Ischaemic Encephalopathy (HIE)
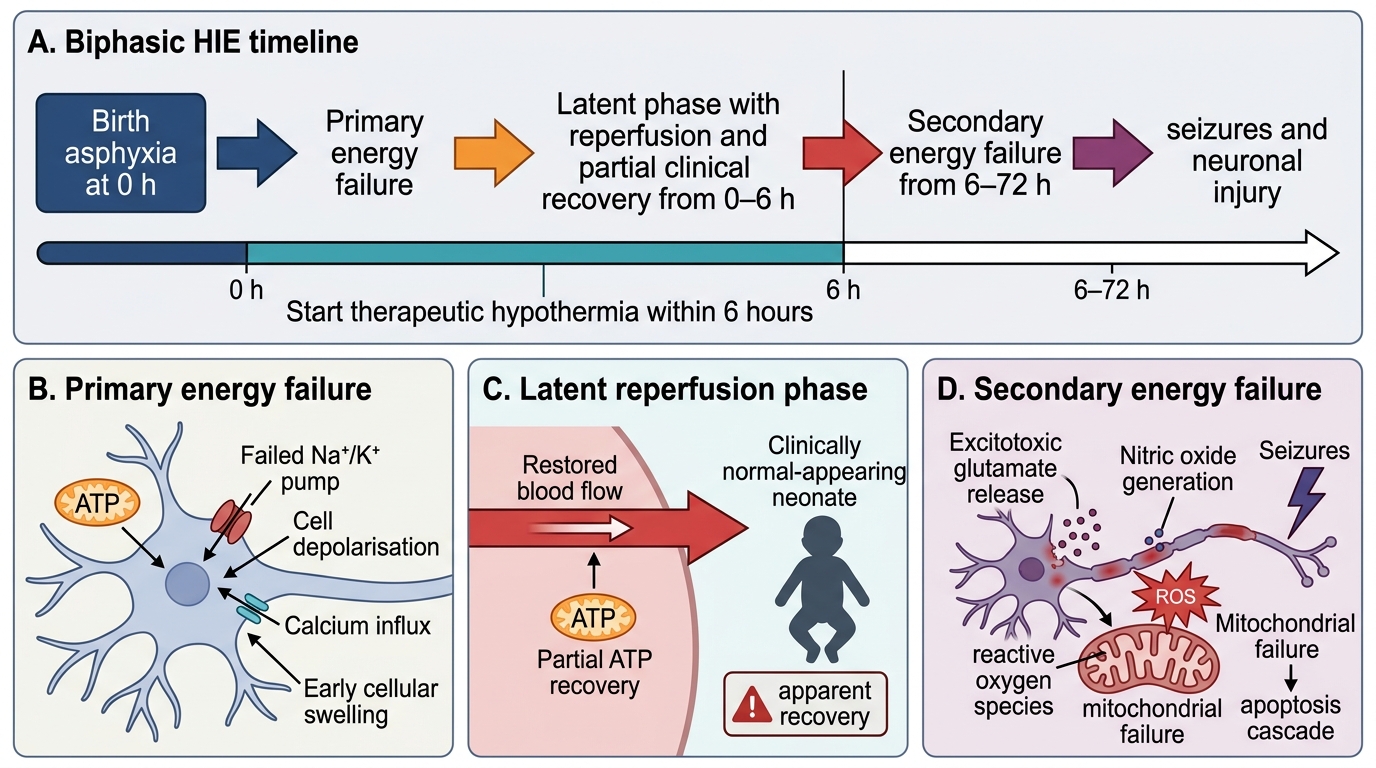
The brain injury of HIE unfolds in two temporally distinct phases after the asphyxic insult, a pattern that has direct therapeutic implications and explains why therapeutic hypothermia works only if initiated within 6 hours.
Phase 1 — Primary energy failure (during the asphyxic insult): When cerebral blood flow and oxygen delivery are interrupted, mitochondrial oxidative phosphorylation fails and ATP production ceases. Without ATP, the Na⁺/K⁺-ATPase pump on neuronal membranes stops working, leading to membrane depolarisation, massive influx of sodium, calcium, and water into cells, and efflux of potassium. This cytotoxic oedema initiates necrotic cell death in the most vulnerable regions (the watershed zones, basal ganglia, and thalami in term neonates). Simultaneously, anaerobic glycolysis generates lactate, causing the characteristic metabolic acidosis of birth asphyxia. If the asphyxia is reversed by resuscitation, some neurons recover — but the injury cascade does not simply stop.
Reperfusion interval — the latent phase (hours 0–6 after birth): After resuscitation and restoration of cerebral blood flow, a brief latent phase occurs where the EEG may normalise and clinical signs may improve transiently. This window of apparent stability is critically important — it is the therapeutic window during which hypothermia can interrupt the secondary injury cascade. Neuronal ATP partially recovers during this phase, and cerebral blood flow is restored.
Phase 2 — Secondary energy failure (hours 6–72): Secondary energy failure is triggered by the reperfusion-induced cascade:
- Excitotoxicity: massive release of glutamate from injured neurons activates NMDA and AMPA receptors, causing sustained calcium influx and mitochondrial calcium overload
- Oxidative stress: reperfusion generates reactive oxygen species (ROS) — superoxide, hydroxyl radical, peroxynitrite — that damage lipid membranes, proteins, and DNA
- Nitric oxide (NO) toxicity: induced NO synthase in activated microglia produces neurotoxic levels of NO
- Apoptotic cascade: cytochrome c release from damaged mitochondria activates caspase-3, triggering programmed neuronal death over 24–72 hours
- Inflammation: microglial activation, cytokine release (TNF-α, IL-1β, IL-6) perpetuate injury
Why hypothermia works: Reducing core temperature to 33–34°C slows the enzymatic rate of all these processes — excitotoxicity, free-radical generation, apoptosis — during the 6-hour latent window before secondary failure is established. After 6 hours, the secondary cascade is already underway and the neural damage is less modifiable by cooling.
Biphasic Pathophysiology of HIE
SELF-CHECK
A neonate is born at term with birth asphyxia. At 2 hours of age, the baby appears clinically normal. The neonatal team reassures the parents that the baby has recovered. At 8 hours, the baby develops seizures. Which pathophysiological mechanism best explains this sequence?
A. Primary energy failure causing immediate irreversible necrosis
B. Secondary energy failure following a latent phase of apparent recovery
C. Neonatal hypoglycaemia unrelated to the asphyxic insult
D. Sepsis presenting at 8 hours of age
Reveal Answer
Answer: B. Secondary energy failure following a latent phase of apparent recovery
This is the classic biphasic pattern of HIE. After the initial asphyxic insult causes primary energy failure, there is a latent phase (hours 0–6) where neuronal ATP partially recovers and clinical signs transiently improve — giving a false impression of recovery. Secondary energy failure then develops (hours 6–72), driven by excitotoxicity, oxidative stress, and apoptotic cascades initiated during reperfusion. Seizures typically manifest during or after the secondary phase. This biphasic pattern is precisely why therapeutic hypothermia must be initiated DURING the latent phase (within 6 hours), not after seizures appear.