Page 12 of 53
PE19.5 | Neonatal Respiratory Distress — SDL Guide
Learning Objectives
- Identify the clinical signs of neonatal respiratory distress and apply the Silverman-Anderson Retraction Score
- Describe the pathophysiology of respiratory distress syndrome (RDS), transient tachypnoea of the newborn (TTN), and meconium aspiration syndrome (MAS)
- Distinguish RDS, TTN, and MAS on clinical, radiological, and contextual grounds
- Describe the management of each condition including supportive oxygen therapy, CPAP, intubation with surfactant, and antenatal prevention of RDS
INSTRUCTIONS
Respiratory distress is the most common reason for admission to a neonatal intensive care unit. Three conditions account for the majority of neonatal respiratory distress in the first 24–72 hours: respiratory distress syndrome (RDS) due to surfactant deficiency in preterm neonates, transient tachypnoea of the newborn (TTN) due to retained fetal lung fluid in term neonates, and meconium aspiration syndrome (MAS) in neonates born through thick meconium-stained amniotic fluid. Distinguishing these conditions using gestational age, risk factors, and chest X-ray findings is a core clinical reasoning task for any doctor working in a labour room or neonatal unit. The NMC competency PE19.5 spans aetiology, clinical features, and management of all three.
References
- Ghai Essential Pediatrics, 9th ed., Ch 6 — Respiratory Distress in the Newborn (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 122 — Respiratory Distress in Newborns (textbook)
- European Consensus Guidelines on the Management of Respiratory Distress Syndrome (Sweet et al., Neonatology 2023) (guideline)
- NNF India — Guideline for Management of RDS and Surfactant Therapy (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are on duty in the neonatal unit at 6 AM when three admissions arrive simultaneously. Baby A is a 29-week preterm neonate, grunting, with subcostal retractions and RR 75/min from birth; the chest X-ray shows bilateral ground-glass opacification. Baby B is a 39-week term baby born by elective caesarean section with RR 72/min, grunting, and mild chest retractions — the X-ray shows perihilar streaky shadows with fluid in the horizontal fissure. Baby C is a 41-week post-term baby born through thick meconium-stained liquor, now with RR 80/min, barrel-shaped chest, and patchy opacification on X-ray. Three different diagnoses, three different treatments, three different prognoses. How do you prioritise and what does each baby need right now?
WHY THIS MATTERS
Respiratory distress is the most common presenting problem in the neonatal intensive care unit, accounting for 30–40% of all NICU admissions. In India, where preterm birth rates are approximately 13% (second highest globally), RDS is a leading cause of neonatal mortality and long-term morbidity. The introduction of antenatal corticosteroids and exogenous surfactant therapy has dramatically reduced RDS mortality over the past three decades, but these interventions require correct diagnosis and timely delivery. TTN, while self-limiting, is the most common cause of respiratory distress in term neonates and must be distinguished from sepsis and from RDS to avoid unnecessary antibiotic exposure. MAS carries significant morbidity due to pulmonary hypertension and chemical pneumonitis. A final-year doctor who can correctly identify and initially manage these three conditions will prevent deaths and reduce complications in every setting from a district hospital to a tertiary NICU.
RECALL
Before proceeding, recall the following foundational knowledge. From Physiology (PY): surfactant (primarily dipalmitoyl phosphatidylcholine, DPPC) is produced by type II pneumocytes and reduces alveolar surface tension, preventing collapse at end-expiration; its production is mature by approximately 34 weeks of gestation — explaining why RDS primarily affects preterm neonates. From pe11-normal-newborn: recall neonatal physiological constants — normal respiratory rate is 40–60 breaths per minute; RR >60/min constitutes tachypnoea. From pe11-normal-newborn: the APGAR score assesses condition at birth; the Silverman-Anderson Retraction Score (covered in this module) assesses the severity of respiratory distress — these are different tools for different purposes. From pe11-neonatal-resuscitation: recall the management of meconium-stained amniotic fluid at delivery — a vigorous MSAF neonate gets routine care; the respiratory complication MAS may develop despite appropriate delivery-room management.
Clinical Presentation of Neonatal Respiratory Distress
Respiratory distress in the neonate is a clinical syndrome characterised by increased work of breathing due to reduced pulmonary compliance, airway obstruction, or surfactant deficiency. The clinical signs reflect the neonate's attempts to maintain adequate alveolar ventilation against an increased resistive or elastic load, and recognising them enables rapid triage of severity. Unlike in adults, where the patient can report dyspnoea, the neonate communicates respiratory distress entirely through observable signs — changes in respiratory rate, chest wall mechanics, airway behaviour, and oxygen saturation. The clinician who can read these signs rapidly and accurately is able to triage a distressed neonate within 60 seconds at the bedside without waiting for investigations. Each sign has a specific physiological basis: tachypnoea reflects increased minute ventilation to compensate for reduced tidal volume; grunting reflects the neonate's attempt to generate its own PEEP to prevent alveolar collapse; retractions reflect the high negative intrathoracic pressure required to inflate stiff, non-compliant lungs; nasal flaring reduces upper airway resistance to airflow; central cyanosis reflects alveolar hypoventilation or right-to-left shunting severe enough to desaturate systemic haemoglobin. Understanding the mechanism behind each sign converts a visual observation into a physiological inference.
Provided image
The cardinal signs of neonatal respiratory distress are:
- Tachypnoea — respiratory rate >60 breaths per minute (normal 40–60/min). The most sensitive and consistently present sign; the neonate increases minute ventilation primarily by increasing rate, not depth.
- Expiratory grunting — a low-pitched sound produced by partial closure of the glottis during expiration, generating intrinsic positive end-expiratory pressure (PEEP) to prevent alveolar collapse. Grunting is the neonate's physiological CPAP and is a sign of significant distress.
- Nasal flaring — dilation of the alae nasi during inspiration, reducing upper airway resistance. A subtle but consistent sign, especially in mild or early distress.
- Subcostal and intercostal retractions — inward movement of the chest wall below the costal margin and between the ribs during inspiration, reflecting the high negative intrathoracic pressure required to inflate stiff lungs. Subcostal retractions are more sensitive; xiphoid retraction indicates severe disease.
- Cyanosis — central cyanosis (blue tongue and mucous membranes) indicates clinically significant hypoxaemia (SpO₂ <85–90%); peripheral cyanosis (acrocyanosis) alone is a normal finding in the first hours.
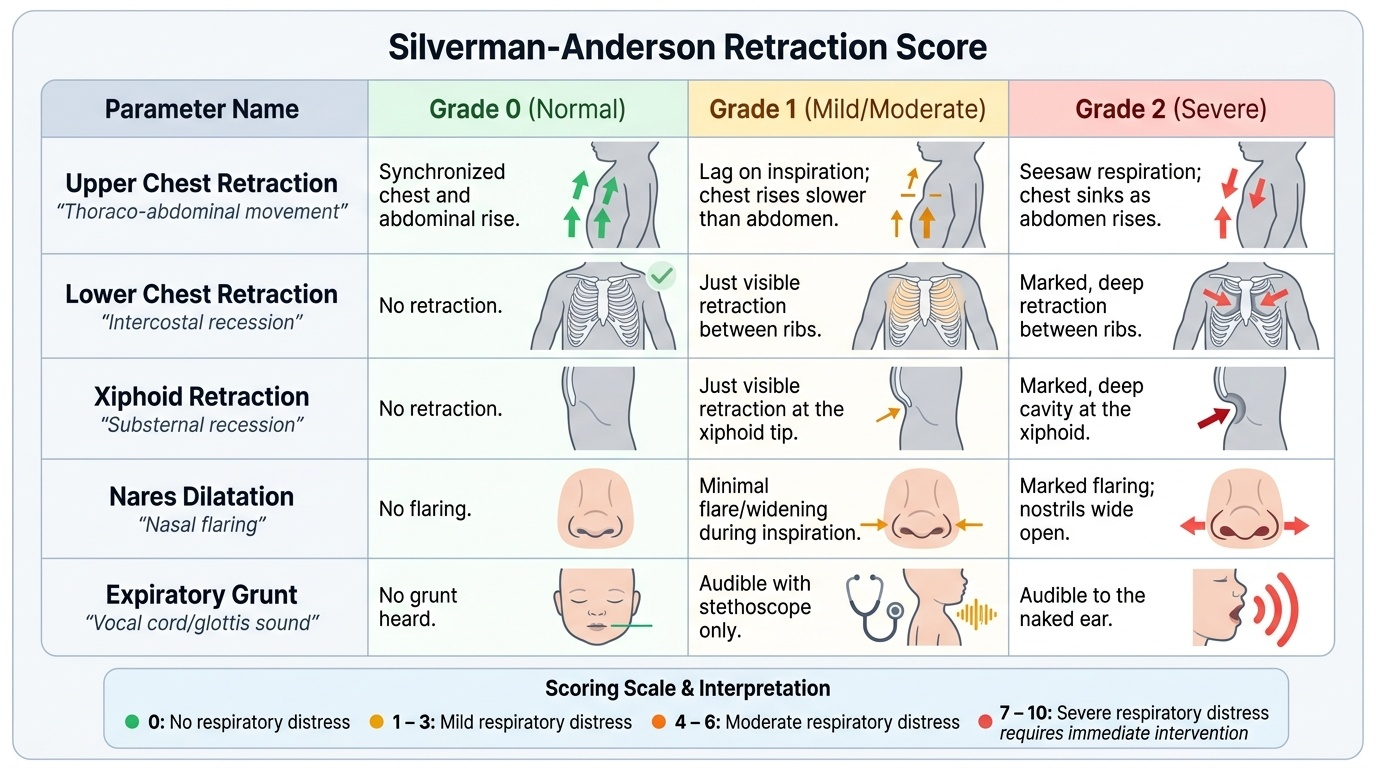
Silverman-Anderson Retraction Score is the standardised tool for quantifying the severity of respiratory distress at the bedside. It assesses five signs, each scored 0, 1, or 2:
| Parameter | 0 | 1 | 2 |
|---|---|---|---|
| Upper chest retraction | Synchronous | Lag on inspiration | See-saw |
| Lower chest retraction | None | Just visible | Marked |
| Xiphoid retraction | None | Just visible | Marked |
| Nares dilatation | None | Minimal | Marked |
| Expiratory grunt | None | Audible by stethoscope | Audible without stethoscope |
Total score: 0 = no distress; 1–3 = mild; 4–6 = moderate; ≥7 = severe (requires NICU and ventilatory support). This scoring system is specifically for monitoring respiratory distress and serial assessment of treatment response. It must not be confused with the APGAR score (which assesses immediate post-birth condition) or the Ballard Score (gestational maturity estimation).
Pathophysiology and Aetiology — RDS, TTN, and MAS
The three most important causes of neonatal respiratory distress have distinct but overlapping pathophysiological mechanisms. Understanding these mechanisms explains not just what each condition looks like, but why specific treatments work and why each entity has its characteristic clinical timeline.
Provided image
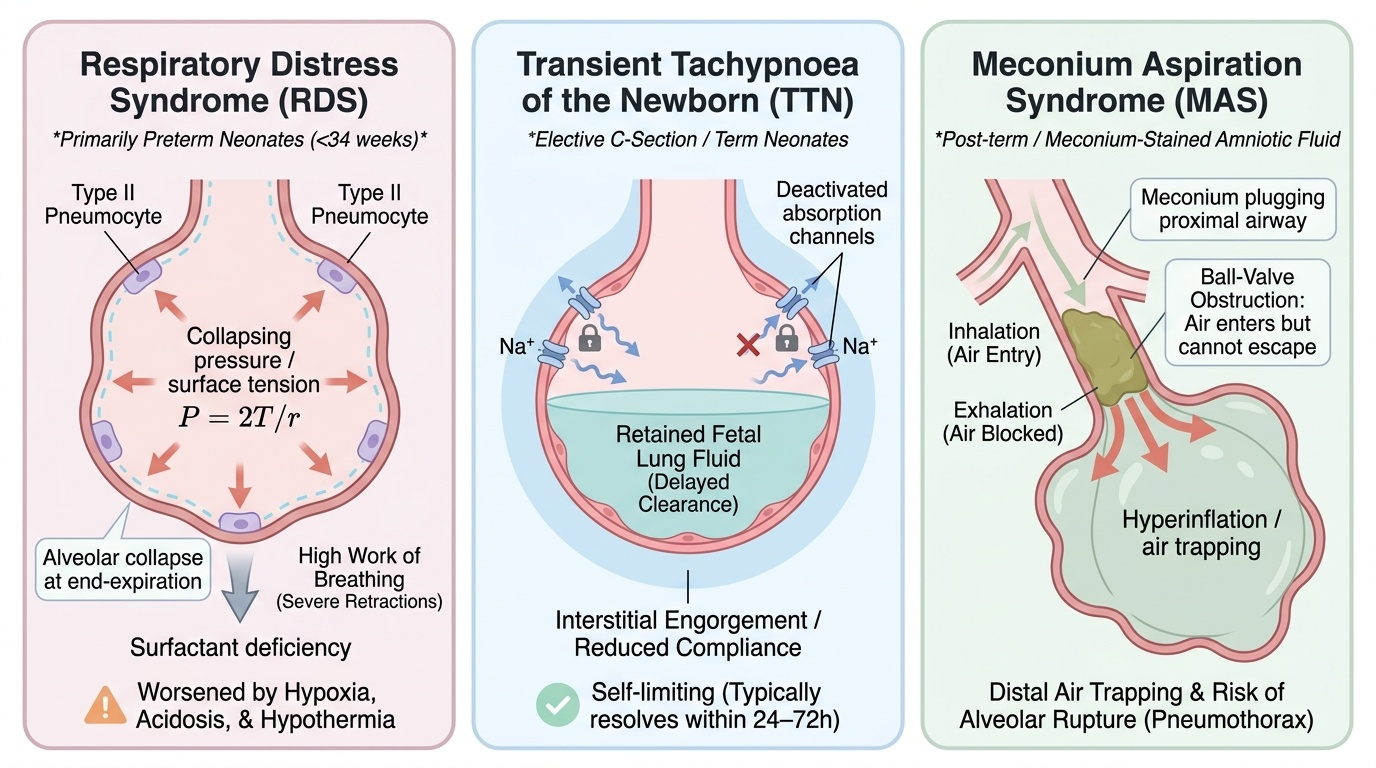
Respiratory Distress Syndrome (RDS):
Surfactant deficiency is the fundamental cause of RDS. Pulmonary surfactant is a complex mixture of phospholipids (predominantly dipalmitoyl phosphatidylcholine, DPPC) and surfactant proteins (SP-A, SP-B, SP-C, SP-D) secreted by type II alveolar pneumocytes. Its critical function is to reduce alveolar surface tension — particularly at end-expiration when alveolar radius is smallest and, by the Law of Laplace (P = 2T/r), collapsing pressure is greatest. Without adequate surfactant, alveoli collapse at end-expiration (atelectasis), and with each breath the neonate must generate very high negative intrathoracic pressure to re-expand them. This enormously increases the work of breathing and rapidly leads to respiratory failure. Type II pneumocyte maturation and surfactant synthesis are complete by approximately 34–36 weeks of gestation, explaining why RDS is almost exclusively a disease of preterm neonates (primarily <34 weeks; mild forms up to 36 weeks). Antenatal glucocorticoids (betamethasone or dexamethasone) accelerate type II pneumocyte maturation and increase surfactant synthesis when given to mothers at risk of preterm delivery — one of the most powerful preventive interventions in perinatal medicine. RDS is worsened by hypoxia, acidosis, and hypothermia, all of which further inhibit surfactant production.
Transient Tachypnoea of the Newborn (TTN):
TTN results from delayed clearance of fetal lung fluid after birth. During fetal life, the lungs are filled with approximately 30 mL/kg of chloride-rich fluid secreted by pulmonary epithelium. During vaginal delivery, thoracic compression and a shift in pulmonary epithelial ion transport (from Cl⁻ secretion to Na⁺ absorption) initiate fluid clearance. In neonates born by elective caesarean section (without labour), breech delivery, or rapid precipitate birth, this clearance mechanism is not fully activated, and retained fluid floods the alveoli and interstitium, reducing compliance and causing tachypnoea. TTN is self-limiting because pulmonary lymphatic and capillary absorption of the retained fluid is complete within 24–72 hours — explaining its characteristically benign clinical course.
Meconium Aspiration Syndrome (MAS):
MAS involves a complex pathophysiology with four components:
1. Mechanical obstruction: meconium particles obstruct airways, causing ball-valve obstruction (air enters past the plug but cannot escape) leading to hyperinflation and air trapping, or complete atelectasis distal to a fully obstructing plug
2. Chemical pneumonitis: meconium contains bile salts, digestive enzymes, and squamous cells that cause direct chemical injury to the airway and alveolar epithelium, inducing an inflammatory response (increased cytokines, neutrophil infiltration)
3. Surfactant inactivation: meconium proteins inactivate surfactant function, adding a surfactant-deficiency component even in term neonates
4. Pulmonary hypertension: the combination of hypoxia, acidosis, and vasoactive substances in meconium triggers pulmonary vasoconstriction, causing persistent pulmonary hypertension of the newborn (PPHN) in severe MAS — right-to-left shunting through fetal channels (foramen ovale, ductus arteriosus) worsens hypoxaemia in a vicious cycle
SELF-CHECK
A 28-week preterm neonate develops respiratory distress immediately after birth. The chest X-ray shows bilateral diffuse ground-glass haziness with air bronchograms and small lung volumes. Which pathophysiological mechanism best explains this presentation?
A. Retained fetal lung fluid causing alveolar flooding
B. Surfactant deficiency causing alveolar collapse at end-expiration
C. Meconium aspiration causing airway obstruction and chemical pneumonitis
D. Congenital pneumonia causing lobar consolidation
Reveal Answer
Answer: B. Surfactant deficiency causing alveolar collapse at end-expiration
This is classic RDS in a preterm neonate. Surfactant deficiency causes alveolar collapse at end-expiration because there is insufficient surfactant to reduce surface tension and maintain alveolar patency. The resulting atelectasis produces diffuse bilateral ground-glass opacity with air bronchograms (patent large airways visible against collapsed alveoli) and small lung volumes on CXR. TTN (retained lung fluid) presents in term neonates, has perihilar streaky shadows, and resolves in 24–72 hours. MAS presents in post-term or term neonates with MSAF exposure and shows hyperinflated lungs with patchy consolidation.
Diagnosis and Investigation of Neonatal Respiratory Distress
The clinical assessment of a neonate with respiratory distress integrates gestational age, delivery context, onset timing, and investigations to reach a working diagnosis. The clinical triad of gestational age + risk factors + chest X-ray pattern differentiates the three major conditions in most cases. This triadic approach is particularly powerful because each of the three key entities — RDS, TTN, and MAS — has a highly characteristic clinical context: RDS almost never occurs in a term neonate; TTN almost never produces a hyperinflated lung on X-ray; MAS almost never occurs without exposure to meconium-stained amniotic fluid. By constructing the diagnosis from these three dimensions before ordering investigations, the clinician forms a pre-test hypothesis that makes the investigation results interpretable rather than confusing. A chest X-ray read without clinical context produces descriptive radiology; a chest X-ray read in clinical context produces a diagnosis. The investigation framework below follows this principle: interpret each result in the light of the gestational age, the delivery context, and the clinical trajectory — whether the baby is improving or worsening over the first 24–48 hours.
Provided image
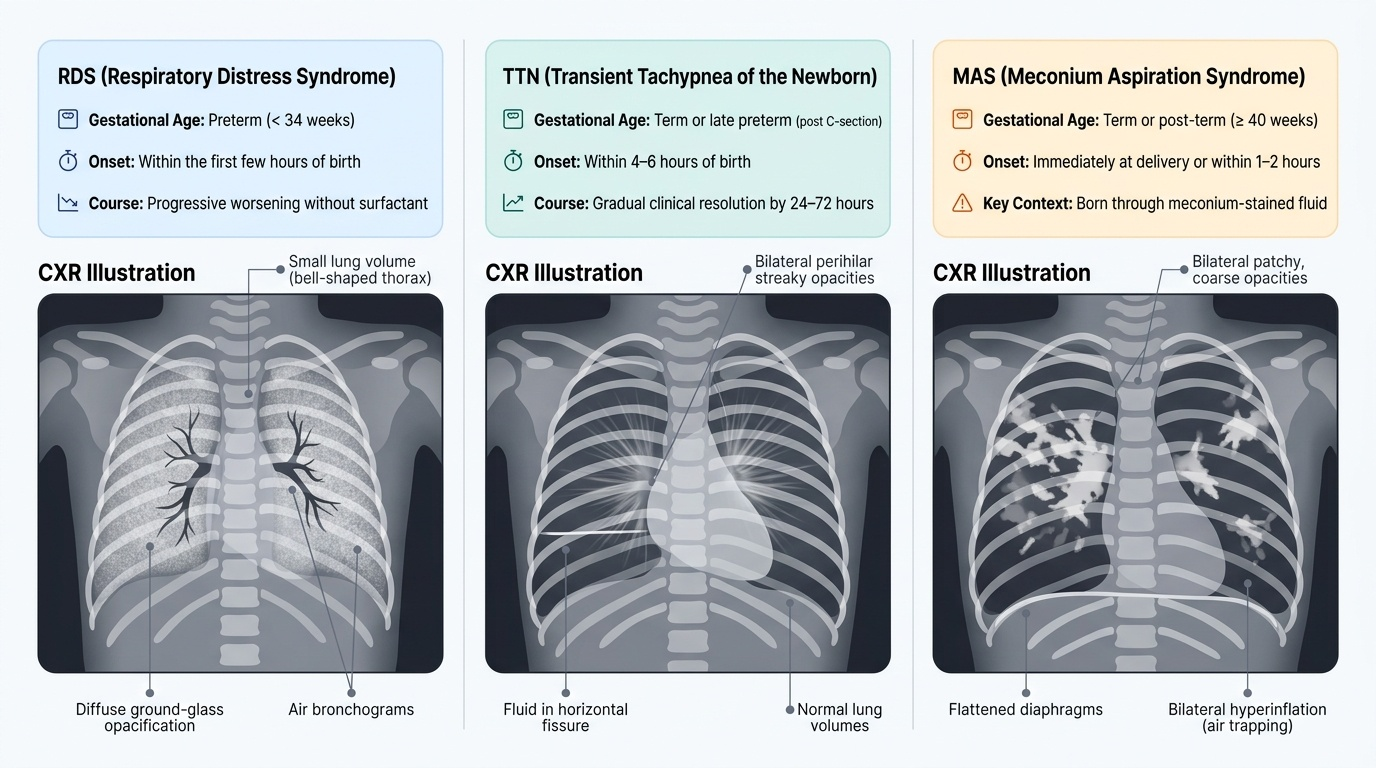
Clinical discrimination by gestational age and context:
- RDS: typically <34 weeks GA (occasionally late preterm 34–36 weeks); onset within the first few hours of birth; progressive worsening without treatment
- TTN: term or late preterm, especially after elective caesarean section without labour; onset within the first 4–6 hours; clinical improvement by 24–72 hours
- MAS: term or post-term (>40 weeks); born through meconium-stained amniotic fluid; onset at delivery or within 1–2 hours; course variable (mild self-limiting to severe with PPHN)
Chest X-ray (CXR) — the most important single investigation:
- RDS: diffuse bilateral ground-glass opacity (uniform haze) with air bronchograms (patent central airways visible against collapsed background); small lung volumes (rib count ≤8 posterior ribs); heart borders may be obscured
- TTN: perihilar streaky shadows (engorged pulmonary lymphatics); fluid in the horizontal fissure (right-sided); mild bilateral haze; normal or slightly large lung volumes; clears by 24–48 hours
- MAS: hyperinflated lungs (flattened diaphragm, rib count >9); coarse patchy bilateral opacities (atelectasis and consolidation alternating with hyperinflated areas); may show air leak complications (pneumothorax, pneumomediastinum)
Arterial blood gas: hypoxaemia (low PaO₂) with respiratory acidosis (high PaCO₂) indicates ventilatory failure; metabolic acidosis indicates end-organ hypoxia. Serial blood gas guides oxygen therapy and ventilator settings.
Sepsis screen: neonatal pneumonia (Group B Streptococcus, E. coli) can present identically to RDS or TTN. A sepsis screen (CBC with differential, CRP, blood culture) should be performed and empirical antibiotics started in any neonate with respiratory distress when infection cannot be excluded — neonatal sepsis does not wait for culture results.
Echocardiography: mandatory in MAS to assess for PPHN, right ventricular function, and to exclude cyanotic congenital heart disease (which can also cause respiratory distress and cyanosis in the first days).
| Feature | RDS | TTN | MAS |
|---|---|---|---|
| Gestational age | Preterm <34 wk | Term/late preterm | Term/post-term |
| Risk factor | Prematurity | Elective CS, no labour | MSAF, fetal distress |
| Onset | At birth, worsens | 4–6 h, improves | At birth |
| CXR | Ground-glass + air bronchograms | Perihilar streaks + fissure fluid | Hyperinflated + patchy |
| Lung volumes | Small | Normal/large | Increased |
| Blood gas | Hypoxia + hypercapnia | Mild hypoxia | Variable, can be severe |
| Course | Progressive without Rx | Resolves 24–72 h | Variable |
| Specific treatment | Surfactant + CPAP | Supportive | CPAP + iNO for PPHN |
SELF-CHECK
A term neonate born by elective caesarean section at 38+4 weeks develops tachypnoea (RR 68/min) and mild subcostal retractions at 3 hours of age. Chest X-ray shows perihilar streaky shadows with fluid in the right horizontal fissure. SpO₂ is 93% in room air. What is the most likely diagnosis and expected clinical course?
A. RDS — will worsen without surfactant therapy
B. TTN — likely to resolve spontaneously within 24–72 hours
C. MAS — requires CPAP and evaluation for pulmonary hypertension
D. Congenital pneumonia — requires immediate broad-spectrum antibiotics
Reveal Answer
Answer: B. TTN — likely to resolve spontaneously within 24–72 hours
TTN is the most common cause of respiratory distress in term neonates, particularly after elective caesarean section without labour (the compression-induced lung fluid clearance mechanism is not activated). The X-ray pattern — perihilar streaky opacities and fluid in the horizontal fissure — reflects retained lung fluid in pulmonary lymphatics and fissures. TTN is self-limiting: as pulmonary lymphatics absorb the retained fluid over 24–72 hours, respiratory distress resolves without specific treatment. Supportive care (supplemental oxygen to maintain SpO₂ ≥94%, monitoring) is all that is required. If distress persists beyond 72 hours, the diagnosis should be reconsidered and sepsis/pneumonia excluded.