Page 38 of 53
PE19.13-14 | Neonatal Sepsis — SDL Guide (Part 2)
Diagnosis: Sepsis Screen and Blood Culture
The diagnosis of neonatal sepsis is challenging because there is no single test with sufficient sensitivity and specificity to confirm or exclude the diagnosis with certainty. Clinical diagnosis is therefore probabilistic — based on risk factors, clinical signs, and a panel of laboratory markers collectively called the sepsis screen. The diagnostic process has two parallel objectives: first, to determine whether to start empirical antibiotics (using the sepsis screen and clinical assessment); and second, to identify the causative organism and its antibiotic sensitivities (using blood culture and CSF culture, which guide de-escalation or targeted therapy). It is critical to recognise that neither the sepsis screen nor blood culture should delay empirical treatment in a sick neonate — both investigations are drawn simultaneously with the decision to treat, not before it.
The NNF Sepsis Screen consists of 5 criteria; a screen is considered positive if ≥3 of the 5 are positive:
1. Total leucocyte count (TLC): <5,000/µL (leucopenia, indicating marrow depletion) or >15,000/µL (leucocytosis)
2. Immature-to-total neutrophil ratio (I:T ratio): >0.2 (elevated band forms indicate marrow stress and accelerated release of immature neutrophils)
3. C-reactive protein (CRP): >1 mg/dL (acute-phase reactant; rises 12–24 hours after infection onset; useful for monitoring response)
4. Micro-ESR: >15 mm/hour in the first 7 days of life or >20 mm/hour thereafter
5. Gastric aspirate polymorphs: >5 per high-power field on the gastric aspirate smear (reflects intra-amniotic inflammation — only relevant in first 12 hours)
Blood culture is the gold standard for definitive diagnosis. Key technical points: collect at least 1 mL of blood (the most common reason for false-negative culture in neonates is insufficient blood volume); use an aerobic blood culture bottle; collect ideally before the first antibiotic dose; sensitivity is approximately 30–40% in culture-confirmed clinical sepsis. A single blood culture is usually adequate in neonates — two cultures are not standard practice given the limited blood volume.
Lumbar puncture (CSF examination) is mandatory if meningitis is suspected (seizures, bulging fontanelle, irritability, septic neonate who is deteriorating). Up to 25–30% of neonates with bacterial sepsis have concurrent meningitis. Do not omit LP — the antibiotic regimen and duration differ significantly (14–21 days for meningitis vs 10–14 days for sepsis without meningitis).
TORCH workup for perinatal infections:
- Maternal and neonatal TORCH IgM and IgG panel (IgM does not cross the placenta; neonatal IgM positivity = active infection)
- CMV: urine CMV PCR (most sensitive); shell vial culture; CMV IgM
- HSV: vesicle swab PCR, nasopharyngeal swab, blood HSV PCR, CSF HSV PCR
- Congenital syphilis: non-treponemal test (VDRL/RPR) titres; treponemal test (TPHA/FTA-ABS); long bone X-rays
- Congenital rubella: rubella IgM; viral culture from nasopharynx, urine
- Ophthalmology for chorioretinitis (Toxoplasma, CMV, rubella, HSV)
- Cranial imaging (CT/MRI/USS): calcifications pattern — periventricular (CMV), scattered (Toxoplasma)
- Audiological assessment (newborn hearing screen) — CMV is the leading cause of non-hereditary sensorineural hearing loss
CLINICAL PEARL
Never delay antibiotics for culture results in a sick neonate. Blood culture takes 24–72 hours to grow an organism. In a neonate with a positive sepsis screen and clinical deterioration, starting empirical antibiotics immediately — after drawing the blood culture — is the correct and life-saving action. Waiting for culture results in a deteriorating neonate can be fatal within hours. Conversely, in a neonate with a positive screen but no clinical signs, close monitoring with repeat screen and culture is acceptable — you do not always need to start antibiotics for a screen-positive, clinically well neonate, but such a baby needs at least 48–72 hours of inpatient observation.
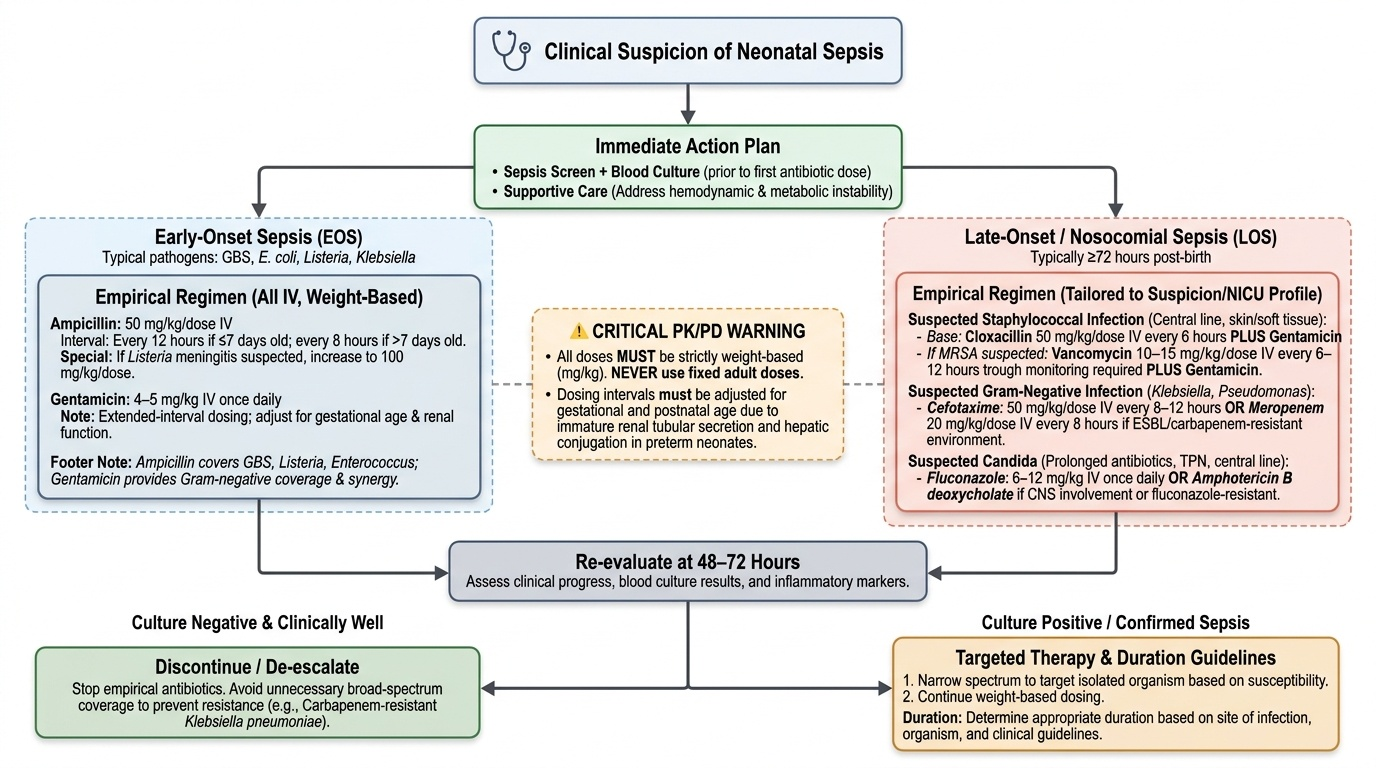
Management: Empirical Antibiotics and Supportive Care
Management of neonatal sepsis integrates empirical antibiotic therapy (targeted at the likely organisms based on EOS vs LOS classification), supportive care addressing the haemodynamic and metabolic consequences of sepsis, and organism-specific treatment once culture results are available. The principle of empirical therapy is to achieve broad-spectrum coverage of the likely pathogens without unnecessarily broad-spectrum use that drives antibiotic resistance — a particular concern in Indian NICUs where carbapenem-resistant Klebsiella pneumoniae is increasingly prevalent. All antibiotic doses in neonates must be weight-based (mg/kg); fixed adult doses are never appropriate. Dosing intervals must also be adjusted for gestational age and postnatal age, because renal tubular secretion and hepatic conjugation both mature over the first weeks of life — immature renal function prolongs drug half-life, requiring less-frequent dosing in very preterm neonates compared with term babies.
Provided image
Empirical antibiotic regimens (weight-based, all doses IV):
For EOS (covers GBS, E. coli, Listeria, Klebsiella):
- Ampicillin 50 mg/kg/dose every 12 hours (neonates <7 days, every 8 hours if >7 days) PLUS
- Gentamicin 4–5 mg/kg once daily (extended-interval dosing; adjust based on renal function and gestational age)
- Ampicillin provides coverage for GBS, Listeria, and Enterococcus; gentamicin provides synergy and gram-negative coverage
- If Listeria meningitis suspected (gram-positive rods on CSF): increase ampicillin dose to 100 mg/kg/dose and add gentamicin for synergy
For LOS (nosocomial/NICU-acquired):
- Replace ampicillin with cloxacillin 50 mg/kg/dose IV every 6 hours if Staphylococcal infection is suspected (central-line associated, skin/soft tissue source)
- If MRSA is prevalent or suspected: vancomycin 10–15 mg/kg/dose IV every 6–12 hours (adjust for renal function; trough monitoring)
- For gram-negative LOS (Klebsiella, Pseudomonas): cefotaxime 50 mg/kg/dose IV every 8–12 hours or meropenem 20 mg/kg/dose every 8 hours in carbapenem-resistant/ESBL-producer environments
- Suspected Candida (immunocompromised, prolonged antibiotics, central line, TPN): fluconazole 6–12 mg/kg IV once daily; amphotericin B deoxycholate if fluconazole-resistant or CNS involvement
Duration of antibiotic therapy:
- Culture-negative with clinically suspected sepsis (screen positive, clinical signs): 5–7 days
- Culture-positive sepsis (bacteraemia): 10–14 days
- Bacterial meningitis: 14–21 days (gram-negative bacillary meningitis usually 21 days)
TORCH-specific treatments:
- HSV encephalitis/disseminated disease: acyclovir 60 mg/kg/day IV in 3 divided doses for 14 (SEM) to 21 (CNS/disseminated) days
- Symptomatic congenital CMV: valganciclovir 16 mg/kg/dose orally twice daily for 6 months (reduces hearing deterioration)
- Congenital syphilis: benzathine penicillin G 50,000 units/kg IM as a single dose (asymptomatic, adequately treated mother) or aqueous penicillin G 50,000 units/kg IV every 12 hours × 10 days (symptomatic)
- Hepatitis B prevention: HBIg 0.5 mL IM + HBV vaccine within 12 hours of birth for babies of HBsAg-positive mothers
Supportive care:
- Maintain normothermia (neutral thermal environment)
- Correct hypoglycemia (glucose <45 mg/dL is common in sepsis; see Neonatal Hypoglycemia SDL)
- Haemodynamic support: normal saline 10 mL/kg IV bolus for shock; dopamine infusion for refractory hypotension
- Respiratory support: supplemental oxygen, CPAP, or mechanical ventilation as needed
- Correct coagulopathy (DIC): fresh frozen plasma (FFP) 10 mL/kg; platelet transfusion if platelets <50,000/µL with active bleeding
- IV immunoglobulin (IVIG): not routinely recommended; may be considered in documented IgG deficiency or refractory sepsis in preterm neonates (limited evidence)
SELF-CHECK
A 10-day-old, 1.2 kg preterm neonate in the NICU has a central umbilical venous catheter and has been on TPN for 8 days. She develops temperature instability, abdominal distension, and thrombocytopenia. Blood culture grows a yeast. What is the most appropriate empirical antifungal agent?
A. Ampicillin + gentamicin
B. Fluconazole 6–12 mg/kg/day IV
C. Acyclovir 60 mg/kg/day IV
D. Meropenem 20 mg/kg/dose IV
Reveal Answer
Answer: B. Fluconazole 6–12 mg/kg/day IV
This preterm neonate has the classic risk factors for Candida LOS: prematurity, long-standing central venous catheter, prolonged TPN, and prolonged antibiotic exposure. The yeast on blood culture is Candida (most likely C. albicans or C. parapsilosis in a NICU setting). Fluconazole 6–12 mg/kg/day IV is the first-line antifungal for Candida sepsis in neonates. Amphotericin B deoxycholate is used if fluconazole-resistant species (C. krusei, C. glabrata) are suspected or if CNS involvement is documented. The central line should also be removed, as it is the likely biofilm source.
Self-Assessment
Apply your knowledge of neonatal sepsis through these integration questions.
Q1. A term neonate, born at 38 weeks after 26 hours of ruptured membranes, develops fever (38.2°C) and poor feeding at 18 hours of age. What organisms must you cover empirically and what antibiotic regimen do you start?
Answer: This is EOS (onset <72 hours, risk factor of prolonged ROM >18 hours). Cover GBS, E. coli, Listeria, and Klebsiella. Start ampicillin (50 mg/kg/dose IV every 12 hours) + gentamicin (4–5 mg/kg once daily IV). Draw blood culture before the first dose.
Q2. Name the five NNF sepsis screen criteria and state what score constitutes a positive screen.
Answer: (1) TLC <5,000 or >15,000/µL; (2) I:T ratio >0.2; (3) CRP >1 mg/dL; (4) micro-ESR >15 mm/hr (first 7 days) or >20 thereafter; (5) gastric aspirate polymorphs >5/HPF. Screen is positive if ≥3 of 5 criteria are met.
Q3. A 3-week-old term neonate has hepatosplenomegaly, jaundice, petechial rash, and microcephaly. Urine CMV PCR is positive. What is the diagnosis and treatment?
Answer: Symptomatic congenital CMV infection. Treatment: valganciclovir 16 mg/kg/dose orally twice daily for 6 months. This has been shown to reduce the rate of hearing deterioration in symptomatic congenital CMV. Audiological follow-up is mandatory as CMV is the most common cause of non-hereditary sensorineural hearing loss.
Q4. What is the most critical reason to perform LP in a neonate with suspected sepsis?
Answer: Up to 25–30% of neonates with bacteraemia have concurrent bacterial meningitis. If LP is omitted, meningitis is missed and undertreated — the standard course for bacteraemia (10–14 days) is insufficient for meningitis (14–21 days). Additionally, the organism may grow only in CSF culture (particularly with gram-negative bacillary meningitis), so LP provides both diagnostic and prognostic information.