Page 13 of 30
PE20.5 | Acute Renal Failure — SDL Guide
Learning Objectives
- Classify acute kidney injury (AKI) in children into prerenal, intrinsic renal, and postrenal categories with key paediatric causes
- Apply KDIGO and pRIFLE staging criteria to assess AKI severity
- Recognise haemolytic uraemic syndrome (HUS) — its triad, aetiology, and critical management trap
- Plan initial management including fluid resuscitation, hyperkalaemia treatment, and indications for dialysis
- Enumerate major complications and prognostic factors of paediatric AKI
INSTRUCTIONS
Acute kidney injury is one of the leading causes of acute morbidity in paediatric wards, arising from diverse precipitants ranging from dehydrating gastroenteritis to haemolytic uraemic syndrome and obstructive uropathy. Recognising early oliguria, staging AKI correctly, and avoiding specific management traps (particularly the antibiotic-contraindication in HUS) are skills that directly determine patient outcomes. This module builds directly on your renal physiology and fluid management knowledge.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 18 — Kidney Diseases (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 550 — Acute Kidney Injury (textbook)
- KDIGO Clinical Practice Guideline for Acute Kidney Injury, 2012 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-year-old boy is brought to the emergency department with a 5-day history of bloody diarrhoea following a family picnic. Over the past 24 hours he has become pale and irritable, with markedly decreased urine output. On examination he is afebrile, mildly puffy around the eyes, blood pressure 105/70 mmHg, and has petechiae on his lower limbs. His blood tests show haemoglobin 7.2 g/dL, platelets 42,000/µL, creatinine 3.8 mg/dL, and a blood film with fragmented red cells. The junior resident reaches for an antibiotic. Should he?
WHY THIS MATTERS
Acute kidney injury affects approximately 1 in 4 critically ill children admitted to paediatric intensive care units, and community-acquired AKI — most often from dehydrating illnesses — is a daily encounter in general paediatric wards across India. Untreated or mismanaged AKI carries significant risk of permanent renal damage, hypertensive encephalopathy, and death from hyperkalaemia or fluid overload. For a final-year student entering clinical postings, the ability to promptly classify AKI (prerenal vs intrinsic vs postrenal), stage its severity, initiate correct fluid management, recognise the HUS triad, and identify dialysis indications is an essential, examinable competency that bridges pathophysiology directly to bedside action.
RECALL
Before proceeding, recall the following from Year 1/2 foundations:
- Glomerular filtration rate (GFR) and its determinants: renal perfusion pressure, filtration fraction, tubular reabsorption. A fall in GFR underlies all AKI.
- Holliday-Segar maintenance fluids: 100 mL/kg/day for first 10 kg, 50 mL/kg/day for next 10 kg, 20 mL/kg/day for each subsequent kg. This is the baseline against which fluid deficits and replacements are calculated.
- Normal urine output in children: 1–3 mL/kg/hour; oliguria = <0.5 mL/kg/h for ≥6 hours; anuria = <0.3 mL/kg/h for ≥24 hours.
- Potassium homeostasis: serum K⁺ is tightly regulated by aldosterone-mediated distal tubular excretion; oliguria rapidly causes dangerous hyperkalaemia.
- Urinalysis basics: protein, blood, casts, and specific gravity on dipstick + microscopy — you will use these to differentiate AKI types.
Clinical Presentation of AKI in Children
Acute kidney injury (AKI) in children typically presents when a parent notices that the child has passed little or no urine, develops facial puffiness, or appears acutely unwell with features suggesting an underlying trigger. The paediatrician must recognise a constellation of symptoms and signs rather than relying on a single finding, because early AKI may be subtle and easily attributed to the primary illness.
The cardinal presenting features of paediatric AKI span several organ systems. Oliguria (urine output <0.5 mL/kg/h) or anuria is the most consistent indicator, though non-oliguric AKI — in which urine output is preserved but kidney function is impaired — also occurs, particularly with aminoglycoside nephrotoxicity. Oedema develops as sodium and water are retained; it first appears periorbital (especially in the morning) and then in dependent parts, progressing to generalised anasarca in severe cases. Hypertension results from volume overload and renin–angiotensin system activation, and in children can rapidly precipitate hypertensive encephalopathy with headache, visual disturbance, and seizures. Haematuria — microscopic or macroscopic — signals glomerular or tubular injury and is a key pointer to intrinsic renal disease. Constitutional features of the underlying cause are typically prominent: vomiting, diarrhoea, and dehydration in gastroenteritis-associated prerenal AKI; pallor and petechiae in haemolytic uraemic syndrome; dysuria and loin pain in obstructive or infective causes.
Key presenting features to elicit on history and examination:
• Duration and amount of urine output
• Recent diarrhoeal illness, vomiting, fever, fluid intake
• Drug exposure — NSAIDs, aminoglycosides, contrast agents
• Family history of renal disease or hearing loss (Alport syndrome)
• Blood pressure (always measured in a child with oliguria — hypertension is both a clue and a complication)
• Oedema pattern, signs of dehydration vs fluid overload
• Skin: pallor, jaundice, petechiae, purpura (points to HUS or vasculitis)
The distinction between a child who is dehydrated and oliguric (prerenal AKI, most common in Indian practice) and one who is oedematous and hypertensive with haematuria (intrinsic renal AKI) guides the immediate next step: fluid challenge vs fluid restriction.
Paediatric AKI Pathways Leading to Oliguria
Pathophysiology and Aetiology
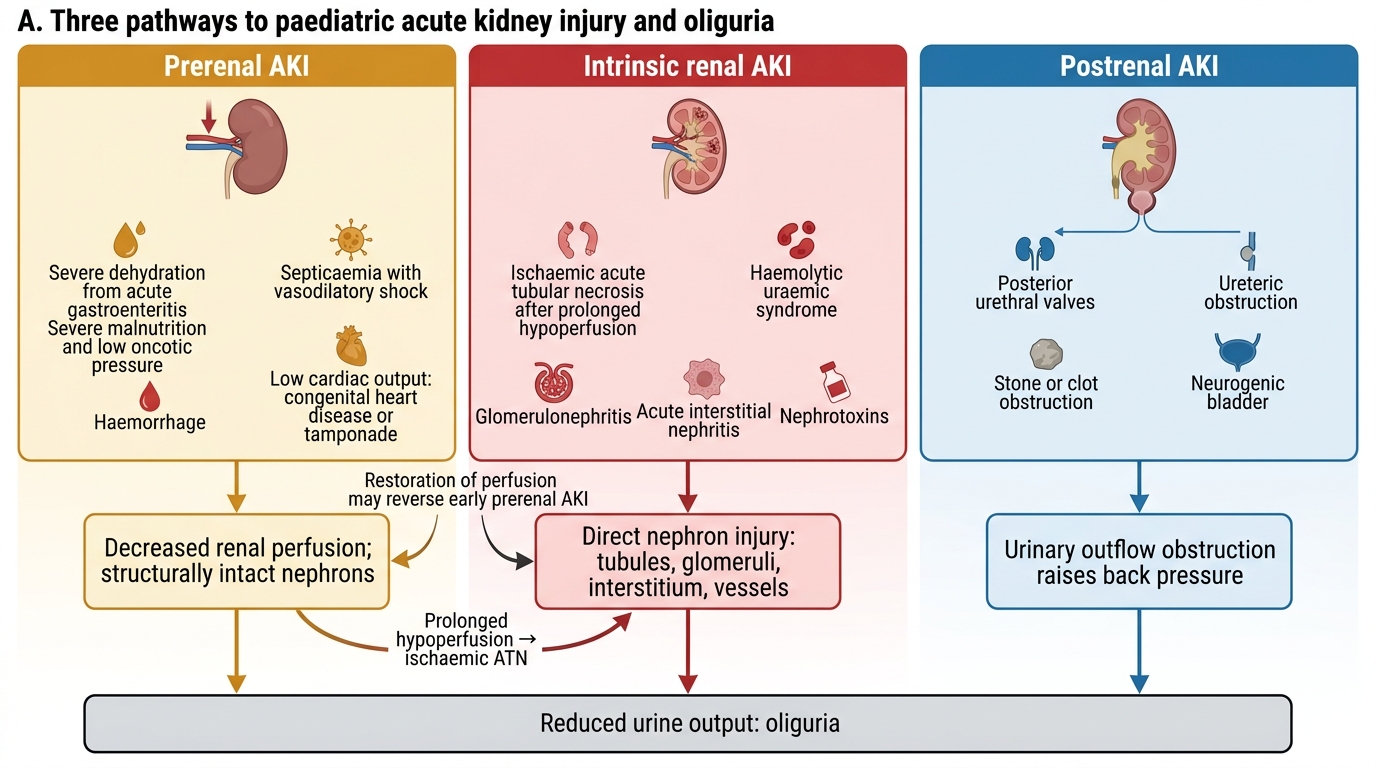
AKI in children is classified into three mechanistic categories — prerenal, intrinsic renal, and postrenal — each with distinct pathophysiological pathways and paediatric-specific causes. Understanding this classification is not merely taxonomic: it directly dictates whether fluid should be given or withheld, a distinction that can be life-saving or life-threatening.
Prerenal AKI is the most common category in Indian paediatric practice, accounting for approximately 60–70% of community-acquired cases. It results from decreased renal perfusion with structurally intact nephrons. Causes include volume depletion (acute gastroenteritis with severe dehydration — the single most common trigger in India), septicaemia (vasodilatory shock), severe malnutrition with low plasma oncotic pressure, haemorrhage, and low cardiac output states (severe congenital heart disease, cardiac tamponade). The kidney responds by maximally conserving sodium and water, producing concentrated oliguria. If perfusion is restored promptly, full recovery ensues. Prolonged prerenal hypoperfusion transitions to ischaemic acute tubular necrosis (ATN), the most common intrinsic AKI pattern.
Intrinsic renal AKI involves damage to the nephron itself — glomerulus, tubules, interstitium, or renal vasculature:
• Haemolytic Uraemic Syndrome (HUS): the commonest cause of intrinsic AKI in children. Characterised by the clinical triad of microangiopathic haemolytic anaemia (MAHA), thrombocytopenia, and AKI. Most cases (diarrhoea-associated HUS, D+HUS) follow Escherichia coli O157:H7 (EHEC) infection — the bacteria produce Shiga toxin, which damages glomerular endothelium, activates the complement pathway, and triggers thrombotic microangiopathy. Critical trap: antibiotics are CONTRAINDICATED in EHEC-HUS because they lyse the bacteria and massively increase Shiga toxin release, worsening the thrombotic microangiopathy and renal outcome.
• Acute Post-infectious Glomerulonephritis (APSGN): follows Group A Streptococcal infection (throat/skin); immune complex deposition in the glomerulus; typically presents 1–3 weeks after streptococcal pharyngitis.
• Ischaemic/Nephrotoxic ATN: follows prolonged prerenal state or direct tubular toxins (aminoglycosides, NSAIDs, IV contrast, cisplatin).
• Acute interstitial nephritis: drug hypersensitivity (beta-lactams, sulphonamides, allopurinol); triad of fever, rash, eosinophilia.
• Rapidly progressive (crescentic) glomerulonephritis: emergency — rapidly destroys glomeruli; seen with Goodpasture disease, ANCA vasculitis, severe APSGN.
Postrenal AKI results from obstruction to urine flow. In children, causes include posterior urethral valves (PUV — the single most important congenital cause; boys only), bilateral pelvi-ureteric junction (PUJ) obstruction, bilateral urolithiasis, and extrinsic compression from a pelvic mass. Obstruction must involve BOTH kidneys (or a solitary kidney) to cause AKI. Early relief of obstruction leads to recovery; prolonged obstruction causes irreversible nephron loss.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
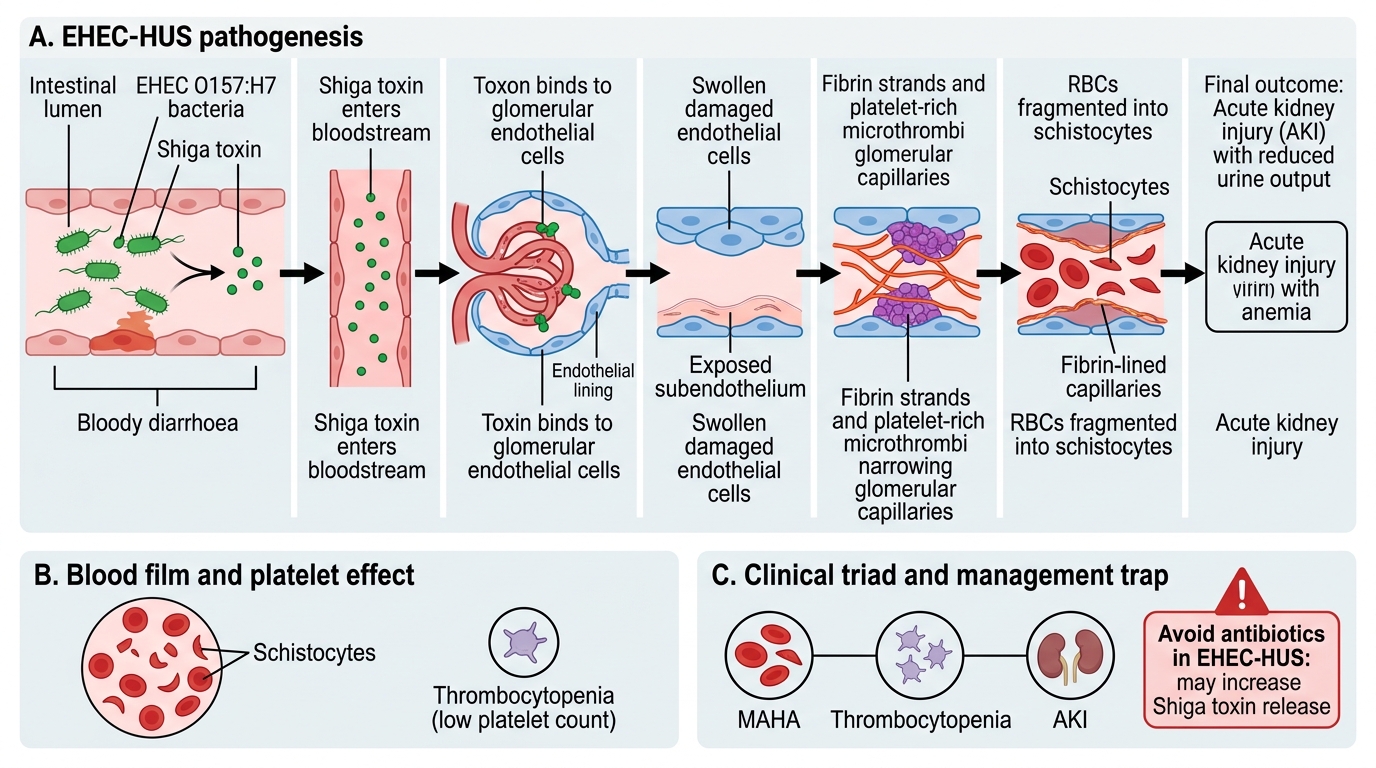
Pathogenesis of EHEC-Associated Haemolytic Uraemic Syndrome
SELF-CHECK
A 5-year-old presents with 4 days of bloody diarrhoea, now pale with petechiae and oliguria. Blood film shows fragmented RBCs. Which single management decision is MOST critical in this case?
A. Start broad-spectrum antibiotics immediately to clear the causative organism
B. Avoid antibiotics because they increase Shiga toxin release and worsen outcomes
C. Begin high-dose corticosteroids to suppress the immune-mediated haemolysis
D. Perform urgent renal biopsy to confirm the diagnosis before any treatment
Reveal Answer
Answer: B. Avoid antibiotics because they increase Shiga toxin release and worsen outcomes
This presentation is classic EHEC-associated haemolytic uraemic syndrome (HUS) — the triad of MAHA (fragmented RBCs), thrombocytopenia, and AKI following bloody diarrhoea. The critical management trap is that antibiotics (especially those that damage bacterial cell walls) cause massive release of Shiga toxin from lysed EHEC O157:H7, dramatically worsening the thrombotic microangiopathy and renal outcomes. Antibiotics are therefore CONTRAINDICATED in EHEC-HUS. Corticosteroids have no proven benefit in typical D+HUS, and biopsy is not the first step.
Diagnosis and Investigation
The diagnostic approach to paediatric AKI has two parallel objectives: confirming AKI and staging its severity, and identifying the underlying category (prerenal vs intrinsic vs postrenal) so that management is targeted correctly. Both objectives can usually be achieved with a focused but systematic set of investigations that proceed from bedside observations through urinalysis and biochemistry to imaging. Careful integration of clinical findings with laboratory data is essential, because in children — unlike adults — creatinine baseline values are much lower, making percentage-change criteria more meaningful than absolute thresholds.
Confirming and staging AKI:
AKI is defined and staged using KDIGO (Kidney Disease: Improving Global Outcomes) criteria, which are based on serum creatinine and urine output. In paediatric practice, the pRIFLE (paediatric Risk, Injury, Failure, Loss, End-stage) staging system — which uses estimated GFR rather than raw creatinine, making it more sensitive for children — is also widely used.
| KDIGO Stage | Creatinine criterion | Urine output criterion |
|---|---|---|
| Stage 1 | ×1.5 baseline in 7 days OR rise ≥0.3 mg/dL in 48 h | <0.5 mL/kg/h for ≥6 h |
| Stage 2 | ×2.0 baseline | <0.5 mL/kg/h for ≥12 h |
| Stage 3 | ×3.0 baseline OR ≥4 mg/dL OR RRT needed | <0.3 mL/kg/h for ≥24 h or anuria ≥12 h |
IMPORTANT: A child's baseline creatinine is lower than an adult's (often <0.4–0.5 mg/dL in young children), so even a creatinine of 1.5 mg/dL represents significant AKI — never interpret paediatric creatinine against adult reference ranges.
Differentiating prerenal from intrinsic renal AKI using urine indices:
Urine indices exploit the kidney's normal tubular responses: in prerenal states, intact tubules conserve sodium avidly, producing concentrated urine with low urine sodium; in intrinsic (tubular) injury, this concentrating ability is lost.
| Index | Prerenal AKI | Intrinsic (ATN) AKI |
|---|---|---|
| Urine sodium (mEq/L) | <20 | >40 |
| Fractional excretion of Na⁺ (FENa) | <1% | >2% |
| Urine osmolality (mOsm/kg) | >500 | <350 |
| Urine:plasma creatinine | >40:1 | <20:1 |
Note: FENa may be falsely low in early contrast nephropathy and myoglobinuria.
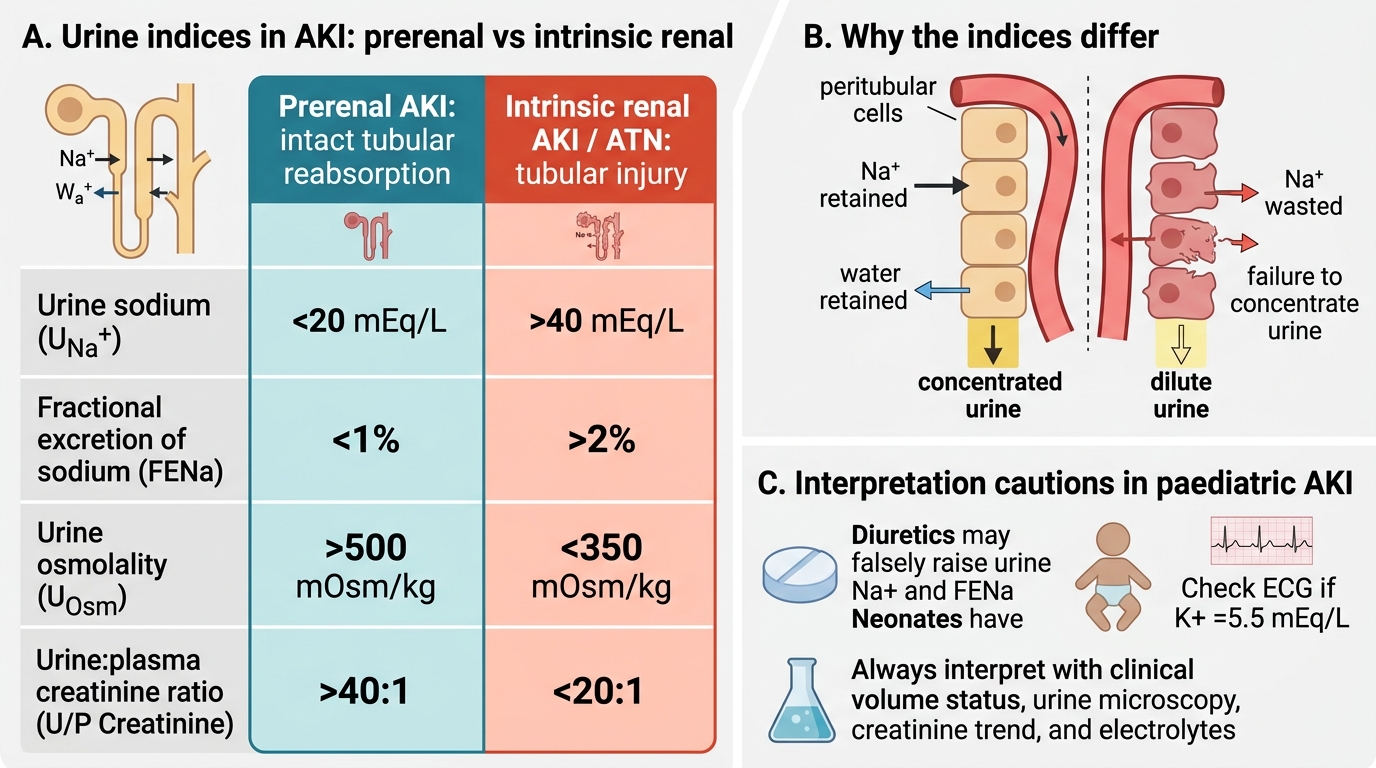
Urine Indices in Prerenal vs Intrinsic Renal AKI
Key investigations in paediatric AKI:
• Serum biochemistry: creatinine, urea (BUN), electrolytes (Na⁺, K⁺ — critical), bicarbonate, phosphate, calcium, albumin
• Urine: dipstick (protein, blood, leucocytes), microscopy (RBC casts = glomerulonephritis; granular casts = ATN; WBC casts = interstitial nephritis), urine sodium + creatinine for FENa
• Full blood count: haemoglobin + blood film (fragmented RBCs/schistocytes = HUS), platelet count
• ASOT and throat/skin swab if APSGN suspected; complement C3/C4 (low in APSGN and lupus nephritis)
• Renal ultrasonography: size, echogenicity, corticomedullary differentiation, hydronephrosis (key for postrenal obstruction), bladder distension
• ECG: mandatory if K⁺ >5.5 mEq/L — peaked T waves (earliest sign), prolonged PR, wide QRS, sine-wave pattern, VF (sequence of hyperkalaemia)
• Renal biopsy indications: atypical HUS (no diarrhoeal prodrome), rapidly progressive GN, AKI with systemic disease (vasculitis, lupus), unexplained AKI not resolving after 3–4 weeks
CLINICAL PEARL
ECG before treating hyperkalaemia: In any child with AKI and a potassium ≥5.5 mEq/L, perform an ECG before making a treatment decision. Peaked T waves are the earliest ECG change (K⁺ ~5.5–6.5), but a wide QRS or sine-wave pattern demands immediate calcium gluconate (cardioprotection) before other measures. Serum potassium level alone does not determine urgency — the ECG integrates the cellular risk. Also remember that pseudohyperkalaemia (haemolysis of the blood sample) is common in paediatric blood draws, especially if the child cried — always repeat before acting on a surprisingly high result.