Page 17 of 30
PE20.6 | Chronic Renal Failure — SDL Guide (Part 2)
Management: Slowing Progression and Treating Complications
Management of paediatric CKD is multifaceted and must simultaneously pursue two interconnected objectives: slowing the inevitable progression of CKD to kidney failure (which in children may span many years if managed optimally) and correcting each of the systemic complications that impair quality of life, physical growth, cardiovascular health, and neurodevelopmental outcomes. Because CKD in childhood unfolds during critical developmental windows — for skeletal growth, brain maturation, and cardiovascular risk accumulation — the paediatrician must actively treat complications rather than merely monitoring the trajectory. The management framework is best organised around five major therapeutic goals, each targeting a discrete and well-characterised pathophysiological mechanism, with evidence-based interventions drawn from international paediatric nephrology guidelines including KDIGO and IAP nephrology consensus statements.
1. Slowing CKD progression:
• Blood pressure control is the single most evidence-based intervention for slowing CKD progression in children. Target BP is below the 50th percentile for age, height, and sex in non-proteinuric CKD, and below the 75th percentile in heavy proteinuria. ACE inhibitors (e.g. enalapril, ramipril) or ARBs are first-line in proteinuric CKD regardless of whether BP is elevated: they reduce intraglomerular pressure and proteinuria via efferent arteriole dilatation and interrupt the TGF-β fibrosis cascade. Monitor potassium (risk of hyperkalaemia) and creatinine (initial acceptable 10–20% rise).
• Dietary protein restriction (0.8–1.0 g/kg/day in G3–G4): reduces uraemic load and may slow hyperfiltration; must be balanced against growth requirements — severe restriction in children impairs growth.
• Avoid nephrotoxins: NSAIDs, aminoglycosides, IV contrast without pre-hydration.
2. Renal osteodystrophy:
Secondary hyperparathyroidism from phosphate retention and low 1,25(OH)2D3 causes: impaired mineralisation → rickets-like changes; trabecular bone disease; growth plate dysfunction contributing to growth failure; elevated PTH-driven bone resorption. Management:
• Phosphate binders (calcium carbonate, sevelamer): given with meals to reduce phosphate absorption
• Active vitamin D (alfacalcidol or calcitriol): replaces the absent renal 1α-hydroxylase step; suppresses PTH; requires monitoring calcium to avoid hypercalcaemia
• Dietary phosphate restriction
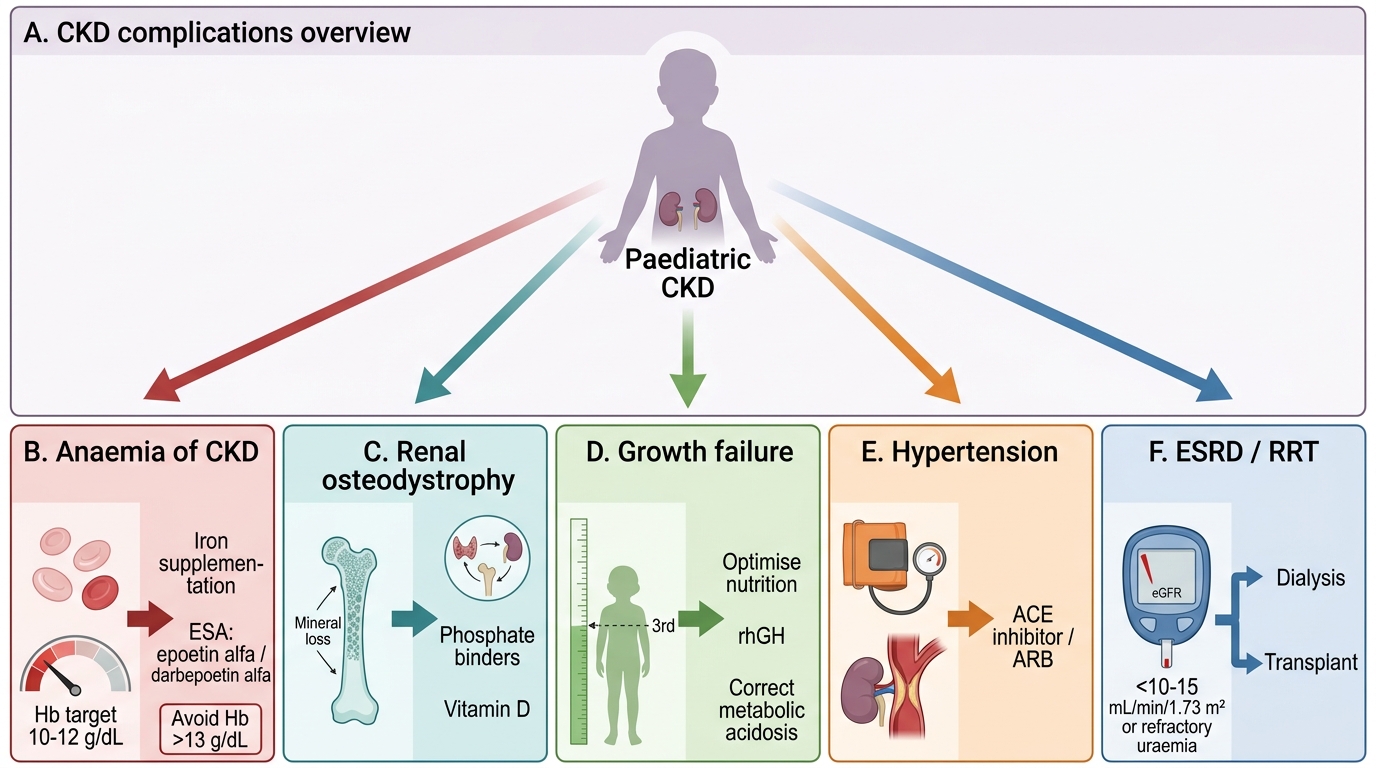
Management of Paediatric CKD Complications
3. Anaemia of CKD:
• Confirm iron deficiency before starting erythropoiesis-stimulating agents (ESAs) — iron supplementation is required concurrently (oral ferrous sulphate or IV iron sucrose in haemodialysis patients).
• Epoetin alfa or darbepoetin alfa (weight-based subcutaneous dosing): target Hb 10–12 g/dL; avoid exceeding 13 g/dL (increased cardiovascular and thrombotic risk at high Hb).
4. Growth failure:
• Optimise nutrition: ensure adequate caloric and protein intake; nasogastric or gastrostomy feeds if required.
• Correct metabolic acidosis (sodium bicarbonate supplementation) — acidosis blunts GH action and accelerates protein catabolism.
• Recombinant human growth hormone (rhGH): indicated for children with CKD-associated short stature (height <3rd percentile or impaired growth velocity); given subcutaneously daily; shown to significantly improve height velocity and final adult height; can be used pre-transplant but should be stopped after transplantation (when endogenous GH often recovers).
5. Renal replacement therapy (RRT) — preparation and timing:
• Initiate dialysis at eGFR <10–15 mL/min/1.73m² or with refractory uraemic symptoms/complications.
• Peritoneal dialysis (PD): preferred for infants and young children (continuous, home-based, avoids vascular access); automated PD (APD/CAPD).
• Haemodialysis (HD): for older children, those with peritoneal failure, or post-transplant complications.
• Renal transplantation: the definitive treatment of choice in children; superior to dialysis for growth, neurodevelopment, and quality of life; pre-emptive transplantation (before starting dialysis) is ideal. Living related donor is preferred. Children should be on the transplant waiting list by G4.
SELF-CHECK
A 10-year-old with CKD G4 from reflux nephropathy has Hb 8.2 g/dL, serum ferritin 12 ng/mL, and transferrin saturation 15%. What is the CORRECT sequence of management for his anaemia?
A. Start epoetin alfa immediately at weight-based dose; add iron if Hb does not respond after 4 weeks
B. Iron supplementation first to replete stores; then add erythropoiesis-stimulating agent once iron status is adequate
C. Blood transfusion to rapidly correct Hb, then maintain with periodic transfusions as needed
D. No treatment required until Hb falls below 6 g/dL or the child is symptomatic
Reveal Answer
Answer: B. Iron supplementation first to replete stores; then add erythropoiesis-stimulating agent once iron status is adequate
Before starting ESAs, iron deficiency must be corrected. This child has low ferritin (12 ng/mL) and low transferrin saturation (15%), indicating iron-deficient erythropoiesis. Starting ESA without adequate iron stores produces a poor response ('functional iron deficiency') and wastes the drug. The correct sequence is: iron supplementation first (oral ferrous sulphate 3–6 mg elemental iron/kg/day, or IV iron if oral is insufficient), then reassess iron stores, then add ESA if anaemia persists. Repeated blood transfusions create allosensitisation that can complicate future transplantation — avoid unless urgent.
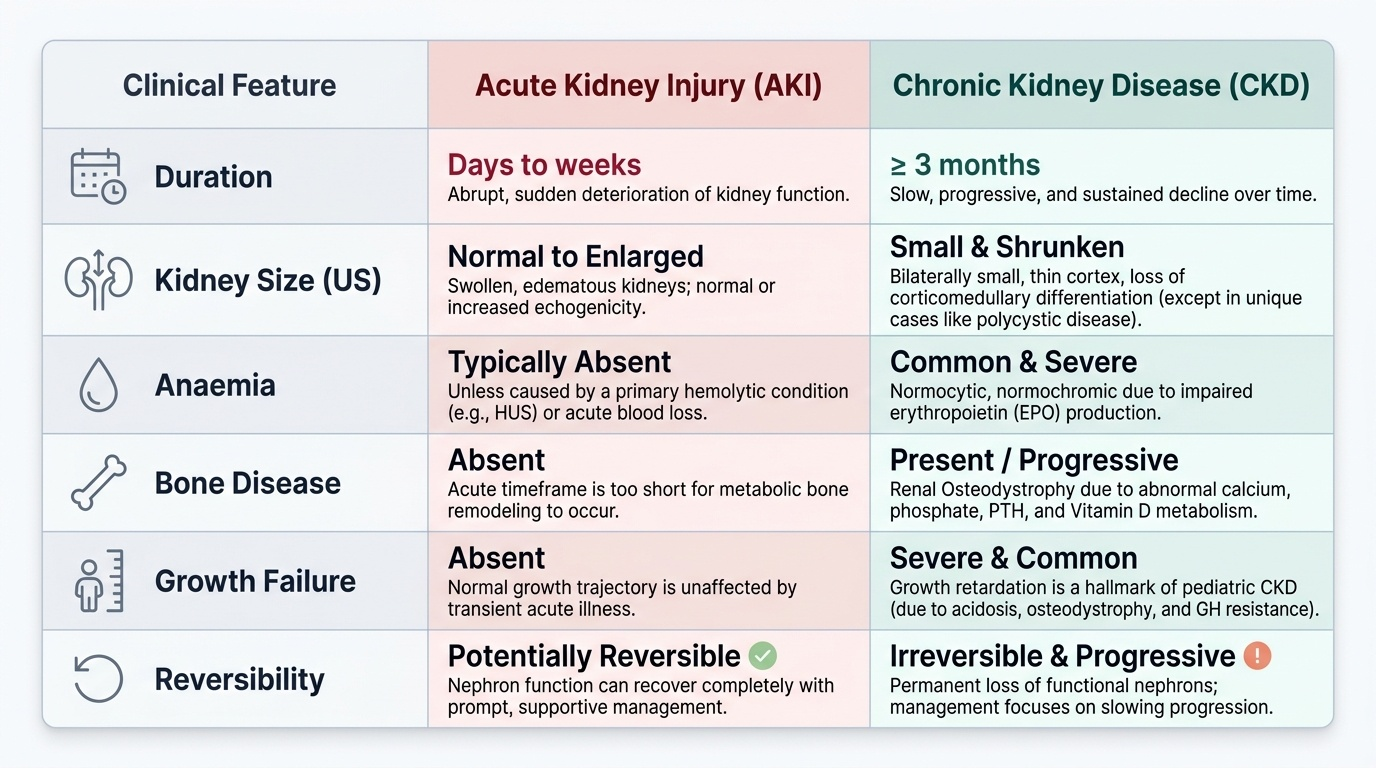
Self-Assessment: CKD in Children
Before moving to the cluster assessments, consolidate your understanding of paediatric CKD with these integrative self-test prompts. Active recall at this stage is far more effective for long-term retention than re-reading the content — the retrieval effort itself strengthens the memory trace even when your answer is incomplete. These prompts specifically target the distinctions between AKI and CKD, and between the paediatric and adult CKD patterns, which are the most commonly examined comparisons in final-year written and clinical examinations across Indian medical schools. Try to answer each prompt fully, stating both the mechanism and the clinical implication, before checking your notes. These questions are specifically pitched at the level of integrated clinical reasoning you will need on paediatric nephrology ward rounds and in final-year professional examinations.
Provided image
- Name the three major aetiological categories of paediatric CKD and give the leading cause in each. Why is CAKUT so much more common in children than in adults?
- What is the KDIGO definition of CKD? Calculate the KDIGO stage for a child with eGFR 22 mL/min/1.73m² and UPCR 65 mg/mmol.
- Explain the pathogenesis of renal osteodystrophy in CKD: which hormones are disturbed, in which direction, and what is the skeletal consequence?
- What is the target haemoglobin in a child with CKD treated with ESA, and why should it not be pushed above 13 g/dL?
- What is the mechanism of growth failure in paediatric CKD, and what is the pharmacological intervention that addresses it?
- At what eGFR threshold should renal transplantation planning begin for a child with progressive CKD?
SELF-CHECK
In a child with CKD from FSGS, phosphate is 6.5 mg/dL, calcium 7.6 mg/dL, and PTH 480 pg/mL. Which treatment combination is MOST appropriate to address the mineral bone disorder?
A. Calcium supplements alone to correct the hypocalcaemia and suppress PTH
B. Phosphate binders with meals (e.g. calcium carbonate or sevelamer) plus active vitamin D (alfacalcidol or calcitriol)
C. Native vitamin D (cholecalciferol) alone to restore vitamin D stores and lower PTH
D. Cinacalcet to directly suppress the parathyroid gland without addressing phosphate or vitamin D
Reveal Answer
Answer: B. Phosphate binders with meals (e.g. calcium carbonate or sevelamer) plus active vitamin D (alfacalcidol or calcitriol)
Renal osteodystrophy in CKD involves both phosphate retention (causing hypocalcaemia and secondary hyperparathyroidism) and absent renal 1α-hydroxylase (preventing conversion of 25(OH)D to active 1,25(OH)2D3). The correct approach therefore targets both: (1) phosphate binders with meals to reduce phosphate absorption and lower serum phosphate (this alone will partially correct hypocalcaemia and PTH), and (2) active vitamin D (alfacalcidol/calcitriol — already the 1-alpha hydroxylated form) to replace the missing renal activation step. Native cholecalciferol CANNOT be converted to active vitamin D if the kidney is failing — it is not the correct form. Calcium supplements alone risk metastatic calcification if phosphate remains high. Cinacalcet is generally reserved for refractory secondary hyperparathyroidism after binders + active vitamin D have been optimised.