Page 22 of 30
PE20.8-9 | Urine and KUB Interpretation — SDL Guide
Learning Objectives
- State the clinical indications for urine examination and plain X-ray KUB in paediatric patients
- Perform urine collection correctly and interpret physical, dipstick, and microscopic urinalysis findings including casts, cells, and crystals
- Apply cast-type interpretation to distinguish glomerulonephritis, pyelonephritis, and ATN
- Systematically interpret a plain X-ray KUB for renal outlines, radio-opaque calculi, bladder, and incidental calcification
- Integrate urinalysis and KUB findings into clinical reasoning for common paediatric renal presentations
INSTRUCTIONS
Urinalysis and the plain X-ray KUB are the two most fundamental investigative skills in paediatric nephrology and urology. Urinalysis is the window into glomerular, tubular, and lower urinary tract pathology, providing real-time cellular and chemical data unavailable from any blood test. The KUB provides structural anatomical information about the urinary tract. Together, these two skills — both in PE20.8 and PE20.9 — are the starting point for evaluating every child with renal disease, urinary tract infection, haematuria, oedema, or suspected urinary obstruction. This module develops both skills systematically through the PE-skills arc.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 18 — Kidney Diseases (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 543 — Laboratory Data (textbook)
- Sutton's Textbook of Radiology, 7th ed. — Plain Film Urinary Tract (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are reviewing a 7-year-old with periorbital puffiness and haematuria in the outpatient department. His urine dipstick shows 3+ blood, 2+ protein, and 1+ leucocyte esterase. The nurse hands you the microscopy report: 'Numerous RBCs, 2–3 WBCs/HPF, and RBC casts present.' His plain X-ray KUB is unremarkable. What does this urine tell you? What would a plain film showing a calcified mass in the left suprarenal region tell you? And how do these two investigations together direct your clinical decision-making?
WHY THIS MATTERS
Urinalysis is cheap, fast, non-invasive, and extraordinarily informative — yet it is frequently performed incorrectly, reported without interpretation, or not requested when it should be. An RBC cast on microscopy establishes glomerulonephritis with near certainty; its absence redirects the diagnostic workup towards infection, calculus, or trauma. A positive dipstick for leucocyte esterase and nitrite in a febrile infant can save hours of diagnostic delay. The KUB X-ray — often regarded as an archaic investigation — retains specific value for radio-opaque renal and ureteric calculi, bladder stones, and the critical differentiation of renal mass calcification patterns (absent in Wilms, present in ~85% of neuroblastoma). Mastering both investigations is a clinical core competency for paediatric and internal medicine practice.
RECALL
Before proceeding, recall the following from prior learning:
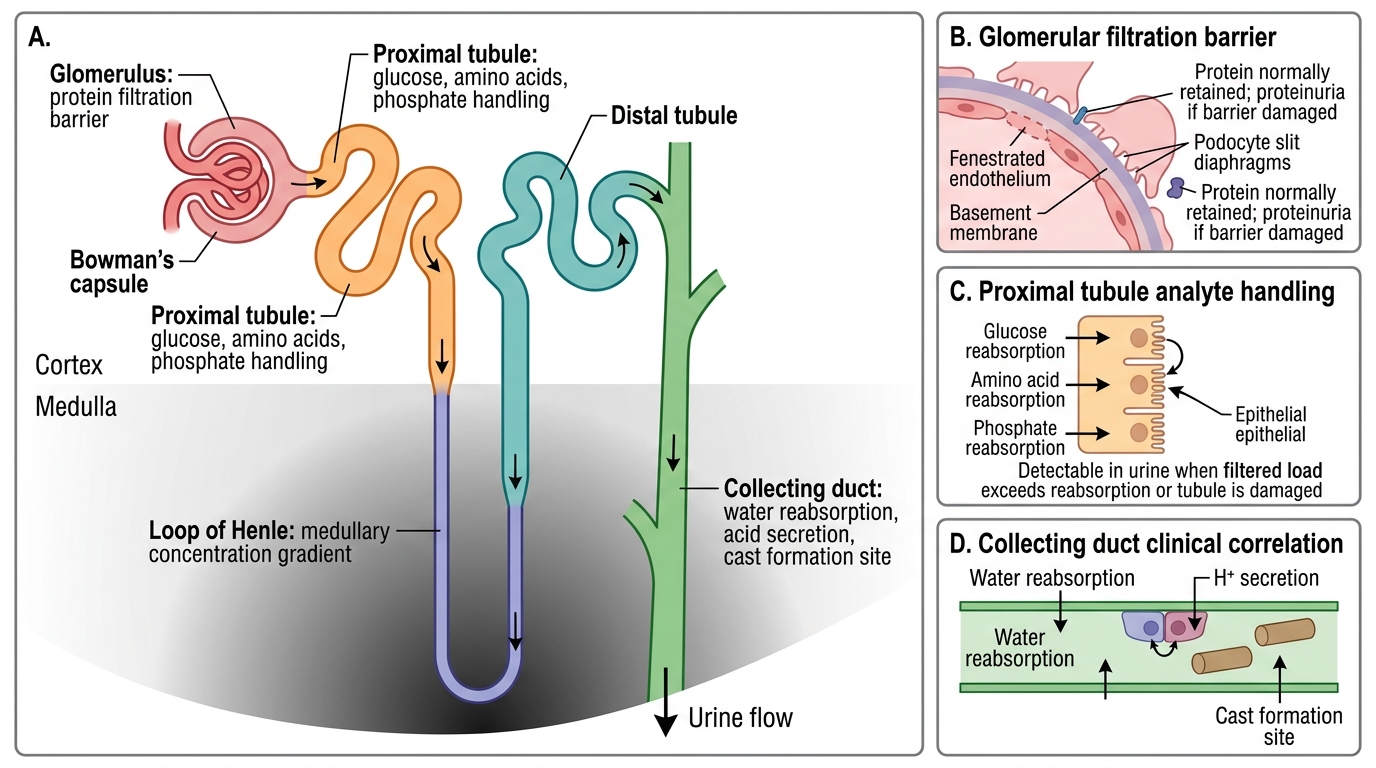
- Nephron structure: glomerulus (filtration), proximal tubule (reabsorption, secretion), loop of Henle (concentration), distal tubule (fine-tuning), collecting duct (water and acid-base). Each segment contributes a different analyte to the urine.
- Urine dipstick analytes: protein, glucose, ketones, pH, specific gravity, blood (haemoglobin/myoglobin/RBCs), leucocyte esterase (WBCs), nitrites (gram-negative bacteria), bilirubin, urobilinogen.
- X-ray physics basics: dense structures (calcium, bone) appear white/opaque on plain film; soft tissue appears grey; gas appears black. Radio-opaque calculi are calcium-containing (visible); uric acid calculi are radiolucent (invisible).
- Haematuria distinction: glomerular haematuria (RBC casts, dysmorphic RBCs, proteinuria) vs non-glomerular haematuria (isomorphic RBCs, no casts, associated with UTI/calculus/trauma).
Clinical Indications for Urine Examination and KUB
Recognising when to request urinalysis and when to request a plain X-ray KUB is the first clinical skill to develop — and it is also the most commonly neglected one. Both investigations are targeted diagnostic tools, not routine screening tests to be requested for every febrile or unwell child, and their clinical value depends entirely on correct patient selection coupled with systematic interpretation of results in clinical context. A urinalysis result from the wrong collection method, or a KUB requested for a radiolucent calculus, can mislead rather than inform. The following indications represent situations where each test has clear diagnostic utility and where omitting it would represent a clinical gap.
Provided image
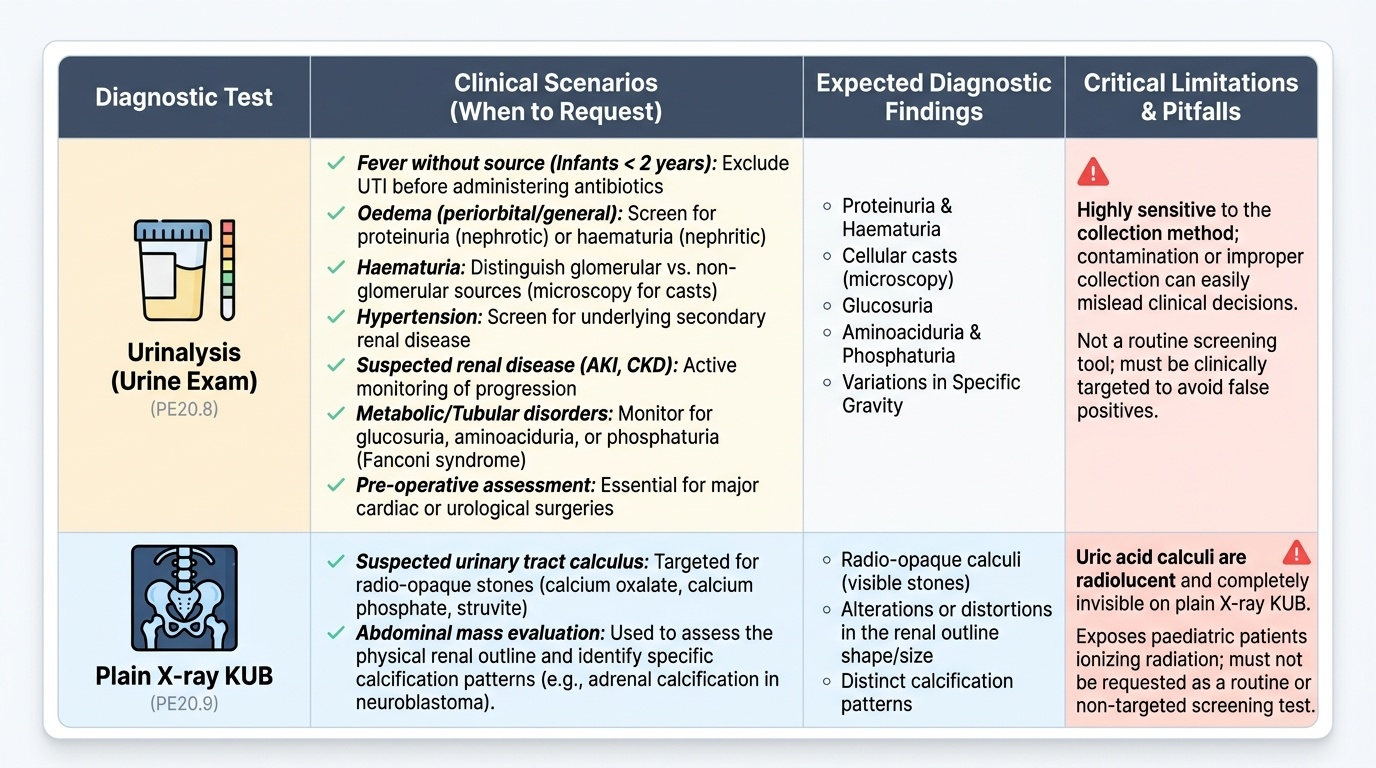
Indications for urine examination (PE20.8):
Urinalysis is indicated across a broad range of paediatric clinical scenarios, and a systematic approach to its interpretation yields high diagnostic value in each:
- Fever without a source in infants <2 years: UTI must be excluded; urine is mandatory before any antibiotic is prescribed
- Oedema (periorbital or generalised): screen for proteinuria (nephrotic syndrome) or haematuria with proteinuria (nephritic syndrome)
- Haematuria (macroscopic or microscopic, detected on dipstick): distinguish glomerular from non-glomerular source by microscopy for casts
- Hypertension in a child: all children with hypertension require urinalysis (renal disease is the most common secondary cause in paediatrics)
- Suspected renal disease (AKI, CKD, renal tubular disorders): monitoring proteinuria, specific gravity, and casts over time
- Monitoring of diabetes mellitus, Wilson disease, or proximal tubular disorders: glucosuria, aminoaciduria, phosphaturia (Fanconi syndrome)
- Pre-operative assessment: in children undergoing any major surgery, particularly cardiac or urological procedures
Indications for plain X-ray KUB (Kidneys-Ureters-Bladder) (PE20.9):
The KUB X-ray provides structural anatomical information about the urinary tract and is selected when structural or calcific pathology is suspected:
- Suspected urinary tract calculus: radio-opaque calculi (calcium oxalate, calcium phosphate, struvite/staghorn) are visible; uric acid calculi are radiolucent and not seen
- Evaluation of an abdominal mass in a child: renal outline assessment, calcification pattern (adrenal calcification in neuroblastoma; Wilms rarely calcifies)
- Urinary tract obstruction: bladder distension, ureteric dilatation (indirect signs)
- Assessment of scoliosis or spinal anomalies associated with urological disease
- Monitoring known calculi for change in size, position, or number without radiation of CT
It is important to appreciate that the KUB is a limited investigation — it does not assess kidney function, detect radiolucent calculi, or evaluate soft-tissue structures reliably. Ultrasound and CT urogram have superior sensitivity for most urological indications, but KUB remains a quick, low-radiation initial film when calculus disease is suspected.
Anatomy and Governing Principles of Urine Formation and Renal Imaging
Understanding the anatomical and physiological basis of each urine analyte makes dipstick and microscopy interpretation rational rather than rote. Each component of the urine reflects the function of a specific nephron segment; an abnormality in a given analyte points to disruption at a predictable anatomical level. Similarly, the appearance of the kidney on a plain X-ray depends on the physics of X-ray attenuation and the density of the structures within the urinary tract.
Physiological basis of key urine analytes:
The glomerular filtration barrier (podocytes + basement membrane + endothelium) normally prevents passage of proteins larger than albumin (~65 kDa). Disruption of the filtration barrier — by immune complex deposition, podocyte effacement, or mesangial injury — allows protein to cross into the filtrate, producing proteinuria. The proximal tubule reabsorbs filtered glucose at normal plasma concentrations (Tm for glucose ~180 mg/dL); when plasma glucose exceeds this threshold (diabetes), or when tubular function is impaired (Fanconi syndrome), glucosuria appears even at normal plasma glucose. The loop of Henle and collecting duct generate concentrated, acidic urine by counter-current multiplication — impairment causes isosthenuria (fixed specific gravity ≈1.010, loss of concentrating ability) and inability to acidify urine.
Basis of casts:
Casts form in the distal tubule and collecting duct lumen when a protein scaffold — primarily Tamm-Horsfall protein (uromodulin) secreted by tubular cells — gels in conditions of high protein concentration, low flow, and acid pH. Cells (RBCs, WBCs, tubular epithelial cells) or cellular debris become trapped in this protein matrix, forming the cast. The type of cell or material enmeshed identifies the site and nature of injury. Casts are washed out by high urine flow, so they may be absent if the child is well-hydrated; fresh urine specimens are essential.
KUB anatomy and X-ray physics:
On a correctly exposed plain AP KUB radiograph, the renal silhouettes are visible as oval soft-tissue densities on either side of the spine, with the right kidney slightly lower than the left. The upper pole of the right kidney overlies the 12th rib; the kidney measures approximately 1 vertebral body length per year of age (rough paediatric guide). The ureters are not normally visible but can be traced by following the line from the renal pelvis over the transverse processes, across the pelvic brim, and to the bladder. The bladder appears as a rounded soft-tissue density in the pelvis, best seen when full. Calcium-containing calculi appear as radio-opaque white densities along the expected course of the urinary tract.
Nephron Segments and Urinalysis Analytes
Technique: Collecting Urine and Performing Urinalysis
The quality of urine examination results depends critically on the method of urine collection and the speed of processing from collection to analysis. Pre-analytical errors — including the wrong collection technique for the patient's age, delayed processing beyond 1–2 hours at room temperature, use of inappropriate containers, and perineal contamination — are the single most common cause of spurious urinalysis results in paediatric practice and directly lead to unnecessary antibiotic prescriptions, unnecessary hospital admissions, and delayed diagnosis of genuine urinary tract infection. This is not an abstract quality concern: studies consistently show that bag specimens in infants have a 30–50% contamination rate, meaning that almost half of all 'positive' bag urinalysis results in febrile infants are false positives. Every final-year student must therefore know the correct collection method for each age group and the standard dipstick and microscopy procedure.
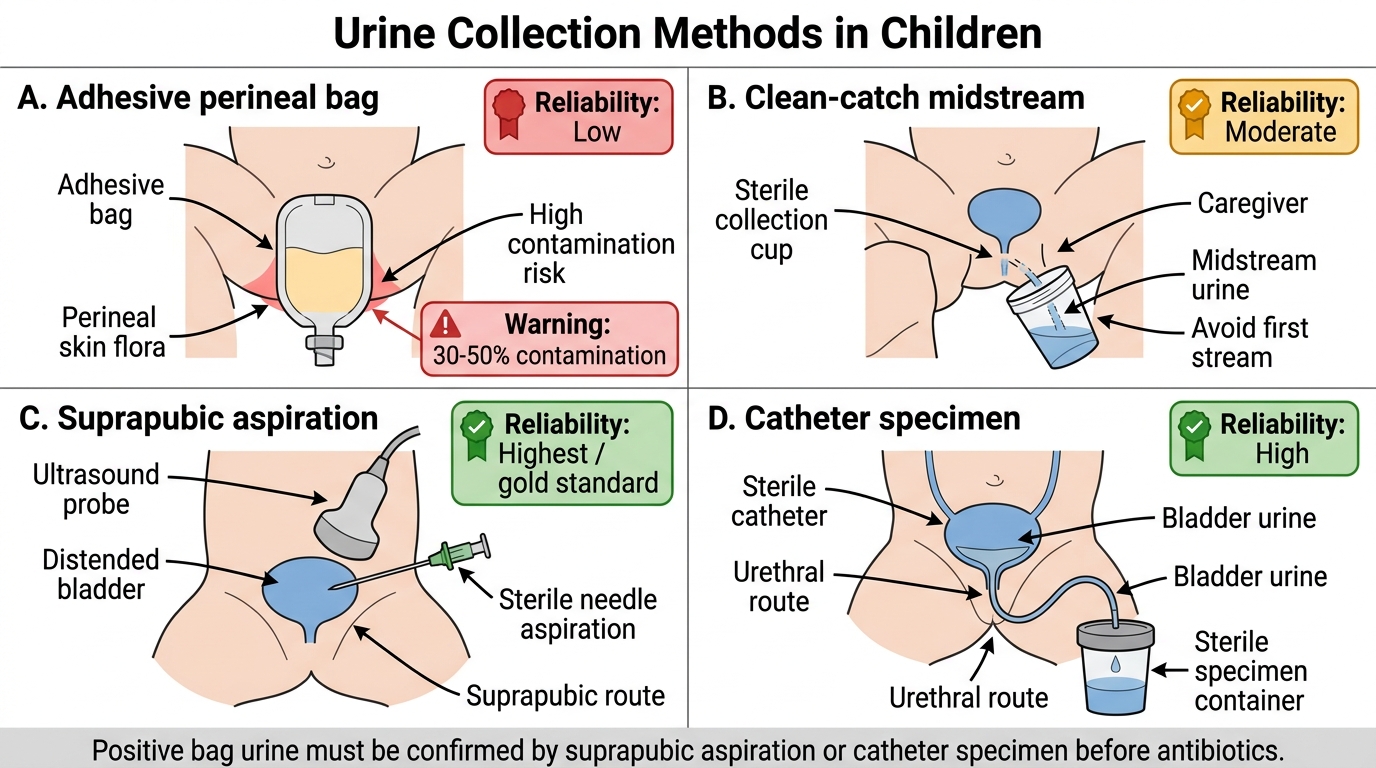
Urine collection methods by age:
- Infants and non-toilet-trained children: three options, in order of increasing reliability:
- Clean-catch (urine collection bag): an adhesive bag applied to the cleaned perineum; high contamination rate (~30–50%) — a positive dipstick from a bag specimen must ALWAYS be confirmed by a more reliable method before antibiotics are started
- Clean-catch midstream urine (MSSU): the preferred method in toilet-trained children; perineum/foreskin cleaned with water (NOT antiseptic), first stream discarded, midstream collected in sterile container
- Suprapubic aspiration (SPA): the gold standard for infants; under ultrasound guidance, a needle is passed directly into the bladder suprapubically; any growth is significant; used when clinical urgency demands immediate reliable results
- Catheter specimen (CSU): via sterile in-out urethral catheterisation; reliable; used in ill infants or those in whom SPA is not feasible
- Toilet-trained children (>2 years): clean-catch midstream is standard; must be processed within 1–2 hours at room temperature or stored at 4°C (up to 24 hours)
Dipstick technique:
Dip the strip completely into fresh well-mixed urine, remove, and read each analyte against the colour chart at the specified time interval (typically 60 seconds total). Do not exceed the stated time interval (false colour changes). Do not use dipsticks that have been exposed to light, moisture, or expired. Report each analyte by grade: negative, trace, 1+, 2+, 3+.
Microscopy preparation:
Spin 10 mL urine at 400g for 5 minutes; decant 9 mL supernatant; resuspend the pellet in 1 mL; place a drop under a coverslip. Examine under low power (10×) for casts and cells, then high power (40×) for cell morphology and organisms. Report cells per high-power field (HPF). Gram stain the sediment if bacterial infection is suspected.
Urine Collection Methods in Children
SELF-CHECK
A 9-month-old febrile girl has a urine specimen collected via an adhesive perineal bag showing leucocyte esterase 2+ and nitrite positive. What is the MOST appropriate next step before starting antibiotics?
A. Start antibiotics immediately based on the positive dipstick — bag urine is reliable in infants
B. Confirm the result with a suprapubic aspiration or catheter specimen before prescribing antibiotics
C. Repeat the bag specimen urine at 24 hours to confirm persistent positivity
D. Send the bag specimen for culture only — culture is more reliable than dipstick
Reveal Answer
Answer: B. Confirm the result with a suprapubic aspiration or catheter specimen before prescribing antibiotics
Urine collected via an adhesive perineal bag has a contamination rate of 30–50% in infants — the perineal skin bacteria (E. coli, mixed flora) contaminate the specimen even with careful cleaning. A positive bag urine result should never be used alone to justify antibiotic treatment; it must be confirmed by suprapubic aspiration (gold standard for infants) or catheter specimen. Starting antibiotics on a contaminated bag specimen leads to unnecessary treatment and masks culture results. This is a well-established principle in paediatric urology and nephrology guidelines (NICE CG54).