Page 20 of 30
PE20.7 | Wilms Tumor — SDL Guide (Part 2)
Management and Complications
Management of Wilms tumor is one of the most successful examples of multimodal paediatric oncology and is guided by the NWTS/COG staging system. The three pillars — surgery, chemotherapy, and radiation — are applied in combinations that scale with tumour stage, histology, and laterality. The goal is maximal cure with minimal long-term toxicity, since these children will live for decades after treatment.
Surgery — radical nephrectomy:
The mainstay of Wilms treatment (in COG protocol) is upfront radical nephrectomy with lymph node sampling performed by an experienced paediatric surgeon. The contralateral kidney is inspected intraoperatively for synchronous disease. Surgical principles include: do not incise the tumour capsule (rupture = Stage III upstaging), ligate the renal vein before the artery (reduces tumour embolism), and perform complete lymph node dissection. The abdominal wound is explored through a transabdominal (not flank) incision for best exposure.
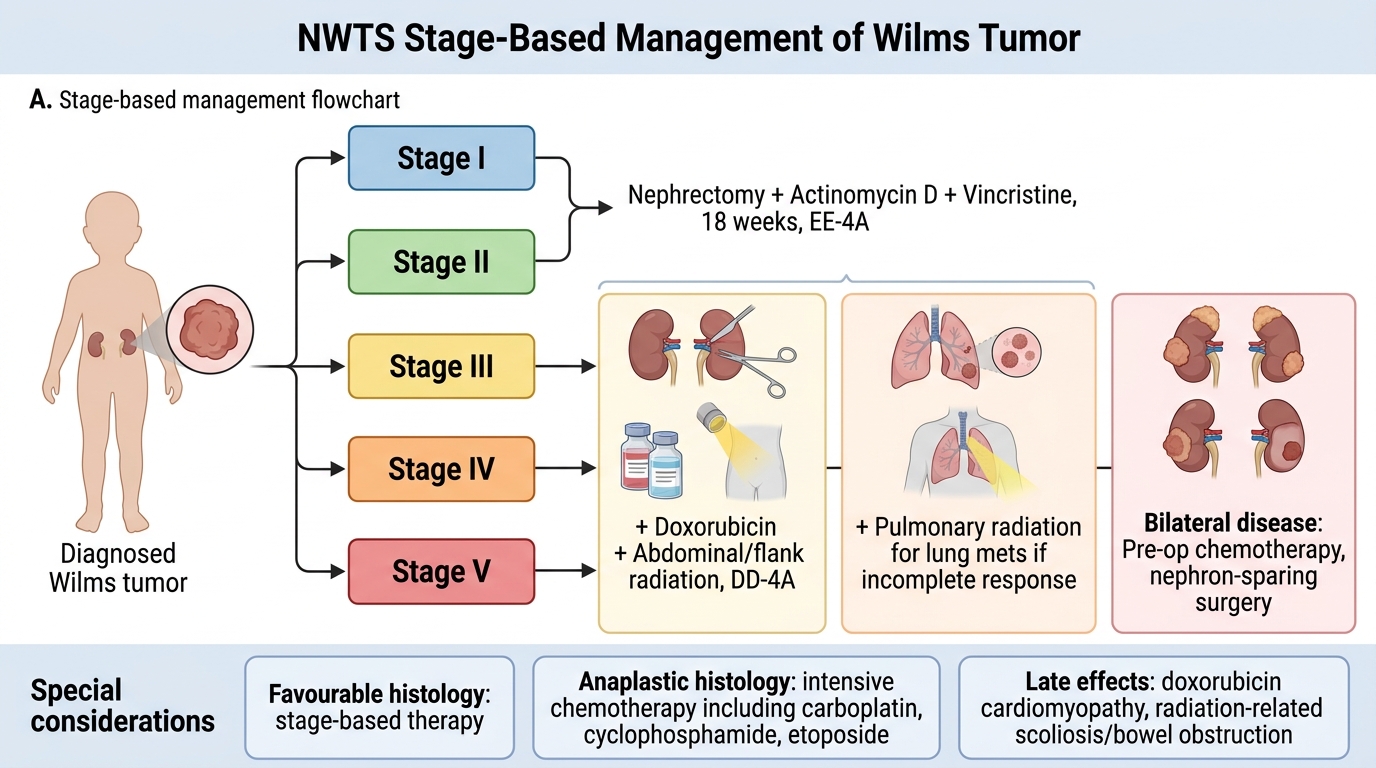
Wilms Tumor Management by NWTS Stage
Chemotherapy by stage:
• Stage I and II (favourable histology): actinomycin D + vincristine for 18 weeks (EE-4A regimen). Cure rate ~95%.
• Stage III and IV (favourable histology): actinomycin D + vincristine + doxorubicin (regimen DD-4A); plus radiation.
• Anaplastic (unfavourable histology): more intensive regimens including carboplatin, cyclophosphamide, etoposide.
Radiation therapy:
• Stage III: whole-abdomen (flank) radiation for peritoneal spill; reduces local recurrence
• Stage IV (lung metastases): whole-lung radiation if metastases do not achieve complete response with chemotherapy
Bilateral Wilms (Stage V) — nephron-sparing surgery:
Bilateral Wilms requires a different approach to preserve renal function. Pre-operative chemotherapy (to shrink both tumours) is given first; then bilateral nephron-sparing (partial nephrectomy) is attempted to avoid bilateral nephrectomy and lifelong dialysis. Surgical planning is complex and requires an experienced centre.
Late effects of treatment:
Because most children are cured, long-term follow-up focuses on treatment-related late effects:
• Doxorubicin: cardiomyopathy (dose-dependent); lifelong cardiac surveillance
• Abdominal radiation: risk of scoliosis (lateral asymmetry), bowel obstruction, secondary malignancies in the radiation field, impaired organ growth
• Renal function: with a single remaining kidney, annual BP and urine protein monitoring; risk of late CKD
• Second malignancies: particularly in the radiation field (bone, soft tissue sarcomas)
SELF-CHECK
A 4-year-old with Stage III Wilms tumor (peritoneal rupture at surgery) has favourable histology. What is the CORRECT treatment plan in addition to surgery?
A. Actinomycin D + vincristine alone (EE-4A regimen) — no radiation needed for Stage III
B. Actinomycin D + vincristine + doxorubicin (DD-4A regimen) plus whole-abdomen radiation
C. Surgery alone is curative for Stage III if margins are negative; chemotherapy only if recurrence occurs
D. Pre-operative chemotherapy with SIOP protocol followed by nephrectomy; no post-operative radiation
Reveal Answer
Answer: B. Actinomycin D + vincristine + doxorubicin (DD-4A regimen) plus whole-abdomen radiation
Stage III Wilms tumor is defined by residual non-haematogenous abdominal tumour — including peritoneal rupture at surgery — which upstages the disease from what might otherwise have been Stage I or II. In the COG/NWTS protocol, Stage III favourable-histology Wilms requires the three-drug regimen (actinomycin D + vincristine + doxorubicin = DD-4A) plus whole-abdomen radiation to sterilise any peritoneal deposits. Omitting doxorubicin or radiation in Stage III significantly increases the risk of local relapse. The EE-4A regimen (actinomycin D + vincristine only) is reserved for Stage I–II favourable histology.
Self-Assessment: Wilms Tumor
Before proceeding to the cluster assessments, use these integrative prompts to consolidate your understanding of Wilms tumor. Wilms tumor is high-yield for written examinations, clinical examinations, and OSCE stations because it tests multiple competency domains simultaneously: clinical reasoning (presentation + physical examination), oncology basics (staging + treatment), genetics (WT1 + syndromes), and the Wilms-vs-neuroblastoma differential that is a perennial question in both written papers and viva examinations. Generate full-sentence answers that include the underlying mechanism or clinical reasoning before checking your notes — this active recall approach is far more effective for long-term retention than re-reading, and the cognitive effort of active retrieval itself reliably consolidates long-term memory traces, even when the initial recalled answer is imperfect, partial, or incomplete.
Provided image
- What is the key physical examination rule for a child with a suspected abdominal mass, and what is the consequence of violating it in Wilms tumor?
- Name the three syndromes associated with Wilms tumor, the key identifying feature of each, and the associated Wilms risk.
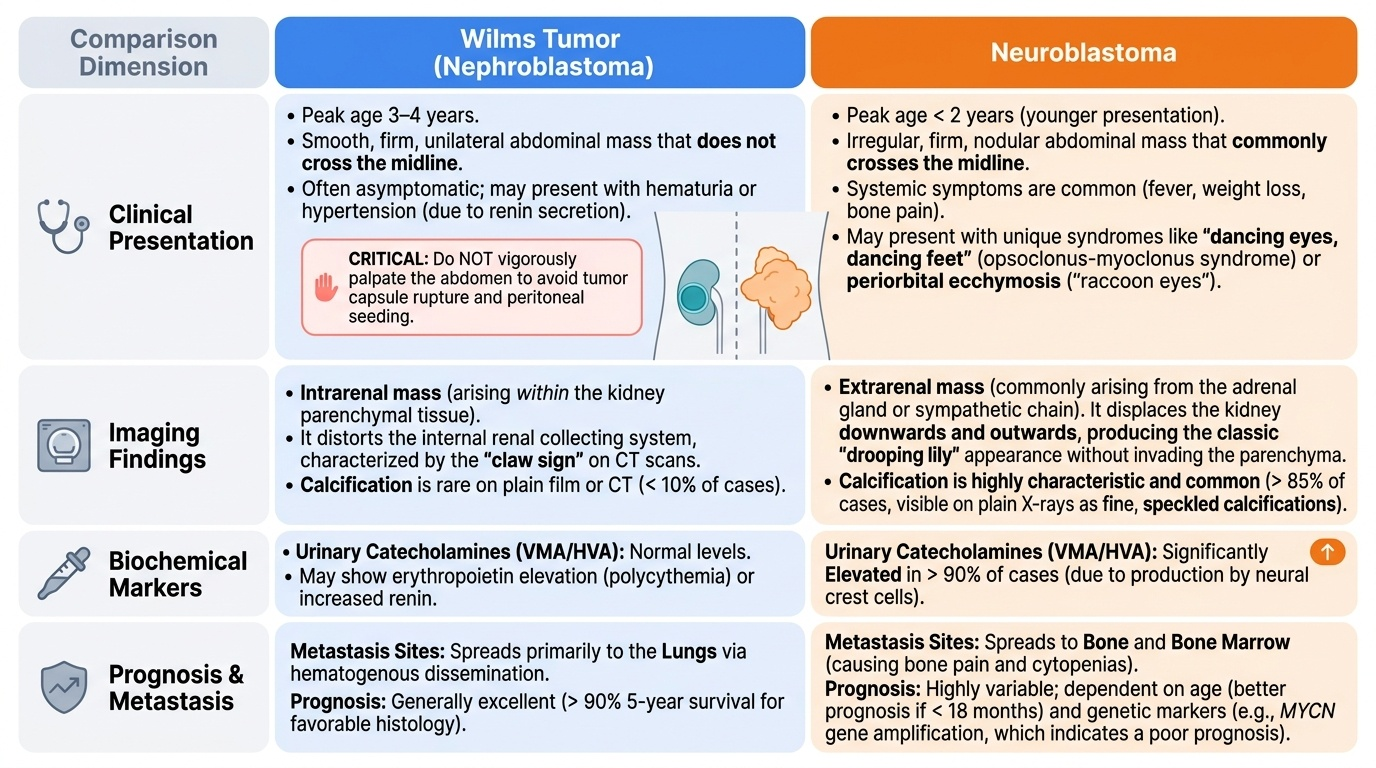
- A 3-year-old has an abdominal mass with calcification on plain X-ray and raised urinary VMA/HVA. Name the diagnosis and explain why antibodies in each distinguishing feature point away from Wilms.
- Apply the NWTS staging to this scenario: a child has a right renal mass that is completely resected, but one regional lymph node is positive on histology. What stage? What treatment?
- What are two late effects of Wilms treatment that require lifelong surveillance?
SELF-CHECK
On plain X-ray of the abdomen in a 2-year-old with a large abdominal mass, you see coarse calcification within the mass, and the mass appears to cross the midline. Which diagnosis does this MOST suggest, and what urine test confirms it?
A. Wilms tumor — confirm with urinary beta-2 microglobulin
B. Neuroblastoma — confirm with elevated urinary VMA (vanillylmandelic acid) or HVA (homovanillic acid)
C. Hepatoblastoma — confirm with elevated serum alpha-fetoprotein (AFP)
D. Renal cell carcinoma — confirm with urine cytology showing malignant cells
Reveal Answer
Answer: B. Neuroblastoma — confirm with elevated urinary VMA (vanillylmandelic acid) or HVA (homovanillic acid)
Calcification is present in ~85% of neuroblastomas on plain X-ray (stippled, amorphous, or coarse calcification within the adrenal/paravertebral mass), and crossing the midline is a classical feature of neuroblastoma arising from the adrenal or sympathetic chain. Wilms tumors rarely calcify and stay within one flank (do not cross midline). Neuroblastoma is confirmed biochemically by elevated urinary catecholamine metabolites — VMA (vanillylmandelic acid) and HVA (homovanillic acid) — in ~90% of cases. Hepatoblastoma arises from the liver and is confirmed by elevated serum AFP. Renal cell carcinoma is rare in young children.