Page 8 of 20
PE21.3 | Kawasaki Disease — SDL Guide (Part 2)
Management of Kawasaki Disease
The management of Kawasaki disease is one of the most time-critical interventions in paediatric medicine. The core treatment is a combination of IVIG and aspirin, given as soon as the diagnosis is made, with the goal of suppressing the vasculitic inflammation before irreversible coronary damage occurs. Alongside pharmacological treatment, echocardiographic monitoring determines the duration and intensity of anticoagulation and long-term cardiac surveillance.
Primary treatment — IVIG:
IVIG 2 g/kg as a single intravenous infusion over 10–12 hours is the definitive treatment. This is the evidence-based dose that produces the greatest reduction in coronary artery aneurysm risk. It must be given within 10 days of fever onset. The mechanism includes Fc-receptor blockade, regulatory T-cell induction, and suppression of pro-inflammatory cytokine production. IVIG is given in hospital under monitoring for infusion reactions (hypotension, flushing, fever — managed by slowing the infusion rate).
Aspirin — two phases:
• Acute (anti-inflammatory) phase: aspirin 30–50 mg/kg/day in 4 divided doses — given during the febrile phase. Note: this is a uniquely high dose of aspirin in paediatrics (normally avoided due to Reye syndrome risk); it is justified here because the anti-inflammatory benefit outweighs the risk in this specific disease context.
• Maintenance (antiplatelet) phase: once the child has been afebrile for 48–72 hours, reduce to aspirin 3–5 mg/kg/day once daily — continued for 6–8 weeks (until echo confirms no coronary changes) or indefinitely if aneurysms are present.
IVIG resistance (persistent fever ≥36 hours after end of first IVIG infusion): occurs in ~10–20% of cases. Options:
1. Second dose of IVIG 2 g/kg
2. Infliximab (anti-TNF-α) 5 mg/kg IV — gaining evidence as effective as second IVIG, fewer side effects in some series
3. Pulse methylprednisolone 30 mg/kg IV × 3 days — used in combination with IVIG in high-risk cases (high Kobayashi score) in Japan; controversial in other settings
4. Cyclosporine or anakinra (IL-1 receptor antagonist) — for refractory disease
Coronary artery aneurysm management by Z-score classification:
| Classification | Z-score | Management |
|---|---|---|
| Normal | <2.5 | Aspirin 6–8 weeks, then stop; echo at 2 and 6 weeks |
| Small dilation | 2.5–5.0 | Low-dose aspirin until normalised; echo every 3–6 months |
| Medium aneurysm | 5.0–10 | Low-dose aspirin + anticoagulation (warfarin or LMWH); echo every 3 months |
| Giant aneurysm | ≥10 or ≥8 mm | Warfarin + aspirin; cardiology follow-up lifelong; coronary CT/MRI; exercise restriction |
Echocardiographic follow-up: at diagnosis; 2 weeks; 6–8 weeks. If normal at all three time points → resolution confirmed. Abnormal findings → graded follow-up per classification above.
Immunisation note: Live vaccines (MMR, varicella) should be deferred for 11 months after IVIG administration because high-dose IVIG may blunt the immune response to live vaccines.
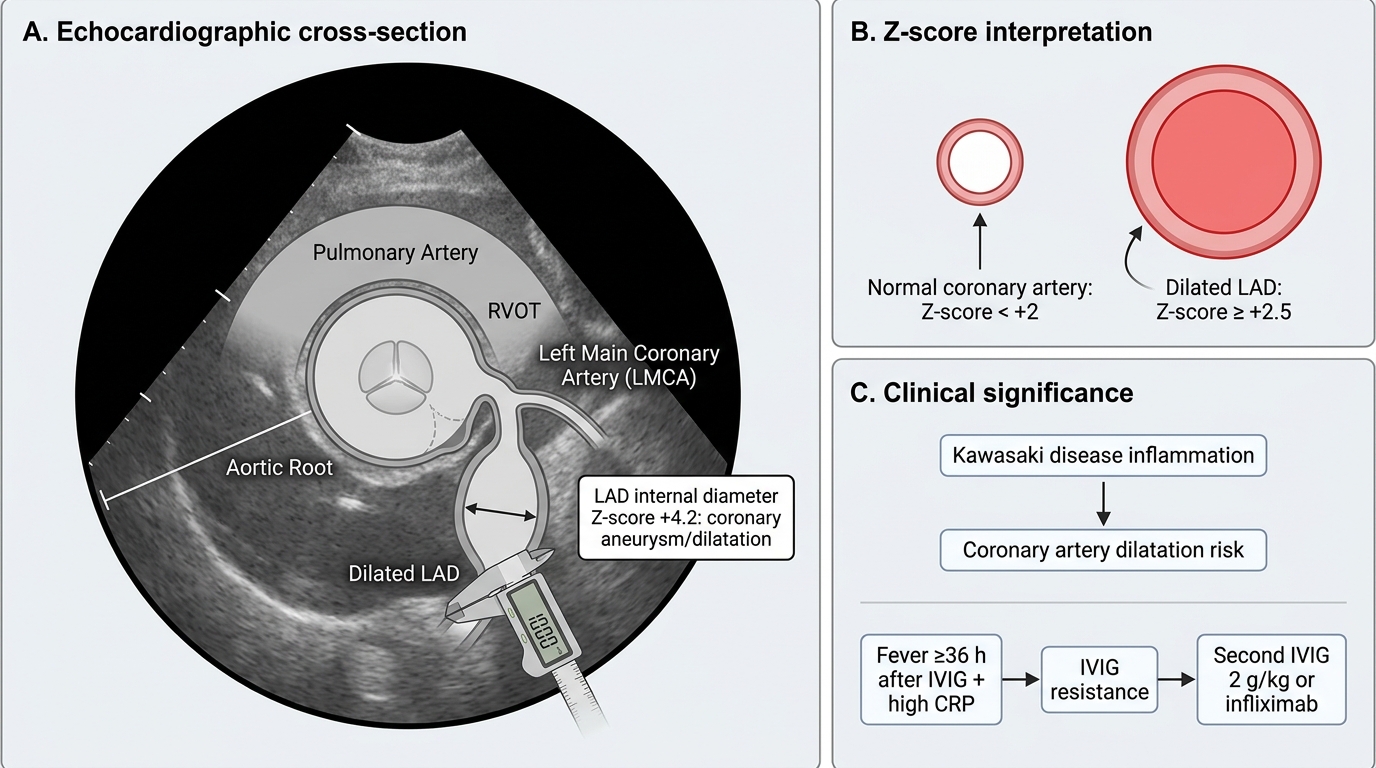
Dilated LAD Coronary Artery in Kawasaki Disease
SELF-CHECK
A 4-year-old boy with confirmed Kawasaki disease received IVIG 2 g/kg on day 8 of illness. He remained febrile for 48 hours after the infusion ended. His repeat CRP is 98 mg/L. What does this indicate and what is the next management step?
A. Treatment failure — the diagnosis was incorrect and Kawasaki disease should be reconsidered
B. IVIG resistance — he needs a second dose of IVIG 2 g/kg or infliximab
C. Normal post-infusion fever — no further treatment needed, observe for 24 more hours
D. He should now receive corticosteroids as the sole treatment without further IVIG
Reveal Answer
Answer: B. IVIG resistance — he needs a second dose of IVIG 2 g/kg or infliximab
Persistent or recurrent fever ≥36 hours after the end of the initial IVIG infusion is defined as IVIG resistance, occurring in approximately 10–20% of cases. It does NOT mean the diagnosis was wrong — it means the inflammatory process has not been adequately suppressed by the first IVIG dose. A persistently elevated CRP confirms ongoing active inflammation. The next step is a second dose of IVIG 2 g/kg (evidence-based, first-line for resistance) or infliximab 5 mg/kg (increasingly used as equivalent or superior to second IVIG with fewer volume-loading concerns). The risk of coronary damage is highest during this ongoing inflammatory period — delay is harmful.
Self-Assessment
Test your understanding of Kawasaki disease with these clinical vignettes and questions.
Case 1: A 18-month-old infant has had fever for 8 days. He has been irritable throughout. On examination he has bilateral conjunctival injection and lip erythema only — no rash, no hand swelling, no lymphadenopathy. CRP is 160 mg/L, ESR 92 mm/hr, albumin 2.7 g/dL, platelet count 430,000/µL, WBC 18,500/µL. Urinalysis shows 12 WBC/hpf. Urine culture is negative. What is the diagnosis and should you treat?
Expected answer: Incomplete Kawasaki disease. Fever ≥5 days + 2 CREAM criteria (conjunctivitis + mucositis). CRP ≥3 mg/dL and ESR ≥40 mm/hr → proceed to supplemental labs. Supplemental criteria present: albumin ≤3 g/dL, WBC ≥15,000, sterile pyuria ≥10 WBC/hpf = 3 criteria met → TREAT with IVIG 2 g/kg + high-dose aspirin. Echo immediately. Day 8 is still within the 10-day window.
Case 2: A child with Kawasaki disease has been treated with IVIG 2 g/kg on day 6. He became afebrile after 24 hours. His echo at diagnosis showed Z-score 2.2 for all coronary arteries. Follow-up echo at 2 weeks shows Z-score 2.2 (unchanged). What aspirin dose do you use now, and for how long?
Expected answer: Echocardiogram shows no coronary dilation (Z <2.5, normal). Switch from high-dose aspirin (30–50 mg/kg/day) to low-dose antiplatelet aspirin (3–5 mg/kg/day once daily) once afebrile 48–72 hours. Continue until 6–8 weeks from diagnosis. If the 6–8 week echo is also normal → aspirin can be stopped. No long-term anticoagulation needed.
Case 3: A 5-year-old boy with giant coronary artery aneurysm (Z-score 12.4 on LAD) after Kawasaki disease. He is now 6 months post-illness and asks about resuming sports. What do you advise?
Expected answer: Giant aneurysm (Z ≥10) carries high risk of coronary thrombosis and myocardial infarction during exertion. Exercise restriction is required — avoid competitive sports and high-intensity activities. He requires lifelong cardiology follow-up, dual antiplatelet therapy (aspirin + clopidogrel) or aspirin + warfarin, and periodic coronary imaging (CT coronary angiography or MRI). Referral to a paediatric cardiologist specialised in Kawasaki disease is mandatory.