Page 11 of 31
PE22.4 | Acute Rheumatic Fever — SDL Guide
Learning Objectives
- Describe the aetiology and pathogenesis of acute rheumatic fever following Group A streptococcal pharyngitis
- Apply the 2015 revised Jones Criteria for diagnosis of ARF in high-risk populations including India
- Recognise the clinical features of carditis, migratory polyarthritis, Sydenham chorea, erythema marginatum, and subcutaneous nodules
- Outline the management of ARF including eradication therapy, anti-inflammatory treatment, and cardiac failure management
- Prescribe and counsel on secondary prophylaxis with benzathine penicillin G, including dose, frequency, and duration by severity
INSTRUCTIONS
Acute rheumatic fever is preventable and treatable, yet it remains the leading cause of acquired heart disease in children and young adults in India and other low- and middle-income countries. A single missed Group A streptococcal throat infection, not treated with penicillin, can trigger an autoimmune cascade that scars the mitral valve and leads to heart failure by age 30. Understanding the 2015 Jones criteria, recognising subclinical carditis, and prescribing the correct secondary prophylaxis regimen are skills that will directly prevent rheumatic heart disease in your community-level practice.
References
- Ghai Essential Pediatrics, 9th edition, Ch 14 — Acute Rheumatic Fever (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 464 — Acute Rheumatic Fever (textbook)
- IAP Guidelines on Rheumatic Fever and Rheumatic Heart Disease; AHA 2015 Jones Criteria Revision (guidelines)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-year-old boy is brought to you with a 3-week history of fever and joint pains that started in the right knee, then shifted to the left ankle, and are now affecting both wrists. He had a sore throat 4 weeks ago that was not treated. On examination: temperature 38.6°C, heart rate 110/min. There is a grade 3/6 apical pansystolic murmur radiating to the axilla. The ESR is 88 mm/h, CRP elevated, and ASO titre 320 Todd units. His joints are hot, swollen, and exquisitely tender — but he can still walk. What syndrome does this represent? What additional features would you look for on full examination? What investigations confirm the diagnosis? And most critically — what do you prescribe today, and what will this child need every 3–4 weeks for the next decade?
WHY THIS MATTERS
Acute rheumatic fever (ARF) is an inflammatory disease that follows Group A streptococcal (GAS) pharyngitis and is caused by an aberrant autoimmune response in genetically susceptible individuals. It is a disease of poverty, overcrowding, and limited access to healthcare — conditions that are widespread across India. ARF is the single most important cause of acquired heart disease in children and young adults in India and globally in low- and middle-income countries, with an estimated 15–19 million people living with rheumatic heart disease (RHD) worldwide. The tragedy is that ARF is preventable: treat GAS pharyngitis with penicillin and ARF does not occur; give secondary prophylaxis reliably and recurrences do not cause progressive valve damage. The 2015 revised Jones Criteria specifically accommodate high-risk populations like India, with lower diagnostic thresholds to ensure earlier detection and treatment.
RECALL
Before proceeding, consolidate these foundational concepts:
- Group A Streptococcus (GAS) = Streptococcus pyogenes: Gram-positive, beta-haemolytic cocci in chains; key virulence factor = M protein (antiphagocytic; molecular mimicry antigen); causes pharyngitis and impetigo but NOT impetigo-associated ARF (ARF follows only pharyngitis).
- ASO (antistreptolysin O) titre: rises 3–4 weeks after GAS pharyngitis; significant titre >200 Todd units in children; confirms recent streptococcal infection — an essential part of the Jones criteria's 'evidence of preceding GAS' requirement.
- Molecular mimicry (PY/Immunology): antibodies produced against a foreign antigen (here, GAS M protein) cross-react with structurally similar host proteins (here, cardiac myosin, valve endothelium), causing autoimmune tissue damage. This is the central mechanism of ARF carditis.
- Mitral valve anatomy (AN): the mitral valve sits between the left atrium and left ventricle; mitral regurgitation produces an apical pansystolic murmur radiating to the axilla. In rheumatic valve disease, the mitral valve is most commonly affected.
Clinical Presentation of Acute Rheumatic Fever
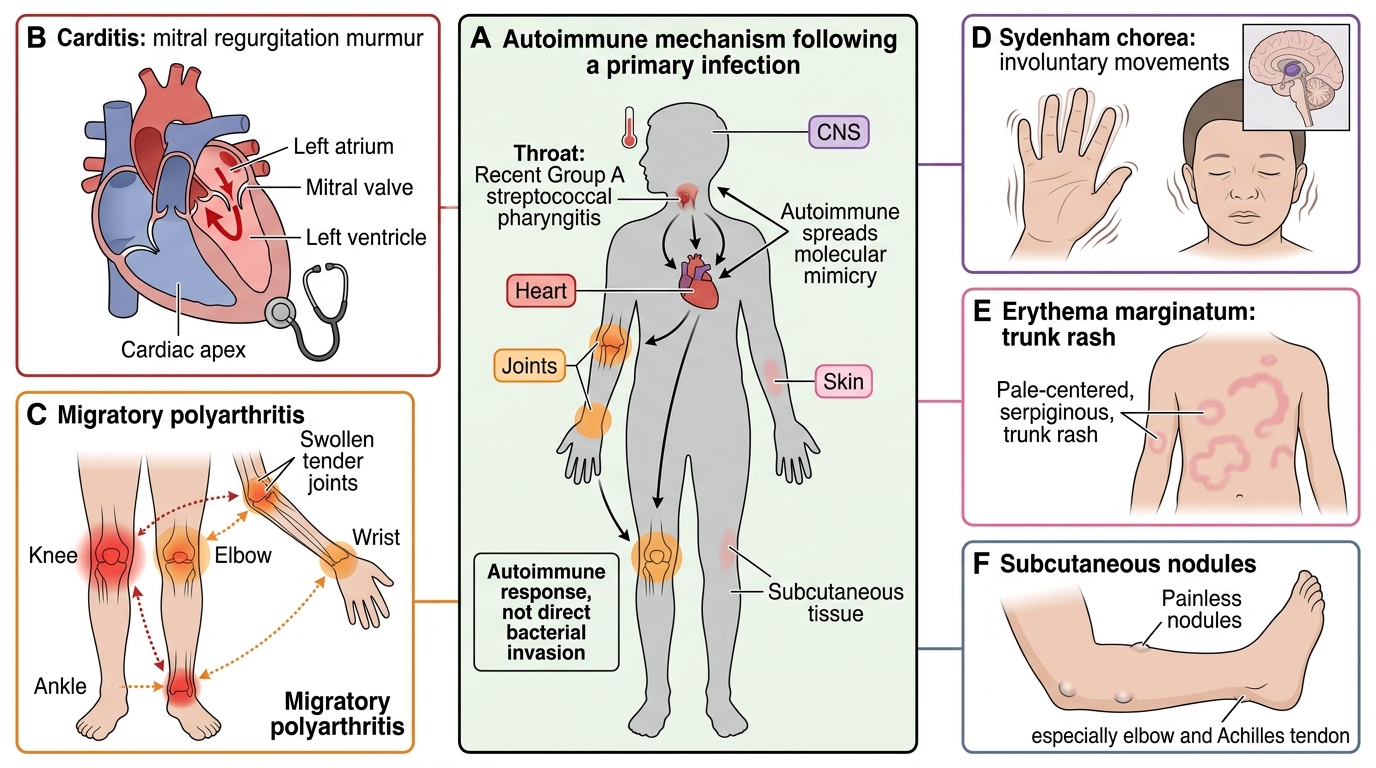
Acute rheumatic fever presents 2–4 weeks after Group A streptococcal pharyngitis in a child typically aged 5–15 years, the age of peak streptococcal pharyngeal colonisation. The clinical features are those of a multi-system inflammatory disease affecting the heart, joints, skin, and central nervous system, and they are best understood through the Jones Criteria, which were specifically designed to capture the combination of features that characterises ARF rather than mimicking conditions. The cardinal presentation in India is a school-age child with fever, a migratory polyarthritis that is disproportionately painful relative to its physical appearance, and a newly audible cardiac murmur — this triad demands immediate consideration of ARF and its implications for the heart.
1. Carditis (most important major criterion — the only criterion with lasting sequelae):
Pancarditis involves pericardium (pericardial rub, chest pain), myocardium (tachycardia, impaired contractility, gallop), and most critically endocardium (valvulitis — most common manifestation). The mitral valve is most commonly affected (mitral regurgitation → apical pansystolic murmur radiating to axilla); the aortic valve is secondarily affected (aortic regurgitation → early diastolic murmur at left sternal border). The tricuspid and pulmonary valves are rarely affected. Valvulitis causes commissural fusion and leaflet thickening over time (rheumatic valve disease). The 2015 revised criteria allow subclinical carditis (echo-proven valvulitis without audible murmur) as a major criterion in high-risk populations — this is critical because subclinical carditis is common in India (up to 15–20% of ARF episodes).
2. Polyarthritis (most common major criterion):
A migratory polyarthritis affecting large joints (knees, ankles, elbows, wrists) in an asymmetric, additive-then-migratory pattern. Each joint is hot, swollen, exquisitely tender — the pain is characteristically disproportionate to the clinical signs (the child may refuse to walk). Crucially, arthritis in ARF resolves completely without joint damage, typically within 4 weeks, and responds dramatically to aspirin within 24–48 hours ('satisfying' aspirin response). In high-risk populations (Jones 2015 revision): monoarthritis alone qualifies as a major criterion because monoarthritis followed by dramatic aspirin response in a high-prevalence setting has a high positive predictive value.
3. Sydenham chorea (isolated major criterion — can occur months after the other features):
Sydenham chorea is an involuntary, purposeless, non-rhythmic movement disorder affecting the face, tongue, and limbs — the child cannot keep the tongue protruded steadily ('jack-in-the-box tongue'), handwriting deteriorates, and voluntary movements become clumsy. It is a late manifestation, appearing up to 6 months after the preceding streptococcal infection, and may occur in isolation without other features of ARF. It is self-limiting (weeks to months) but may recur with subsequent streptococcal infections.
4. Erythema marginatum (uncommon; <10% of cases):
A faint, evanescent, pink rash with pale centres and raised serpiginous red margins, occurring on the trunk and proximal limbs (never the face). It is transient — may be visible only after warming the skin or applying heat. Non-pruritic.
5. Subcutaneous nodules (rare; <5% of cases; occur with severe carditis):
Firm, non-tender nodules over bony prominences and tendons (occiput, vertebral spines, olecranon, patella, metatarsal heads). Freely mobile. They appear with severe carditis and are associated with a higher risk of RHD.
Major Jones Criteria in Acute Rheumatic Fever
Aetiology and Pathogenesis
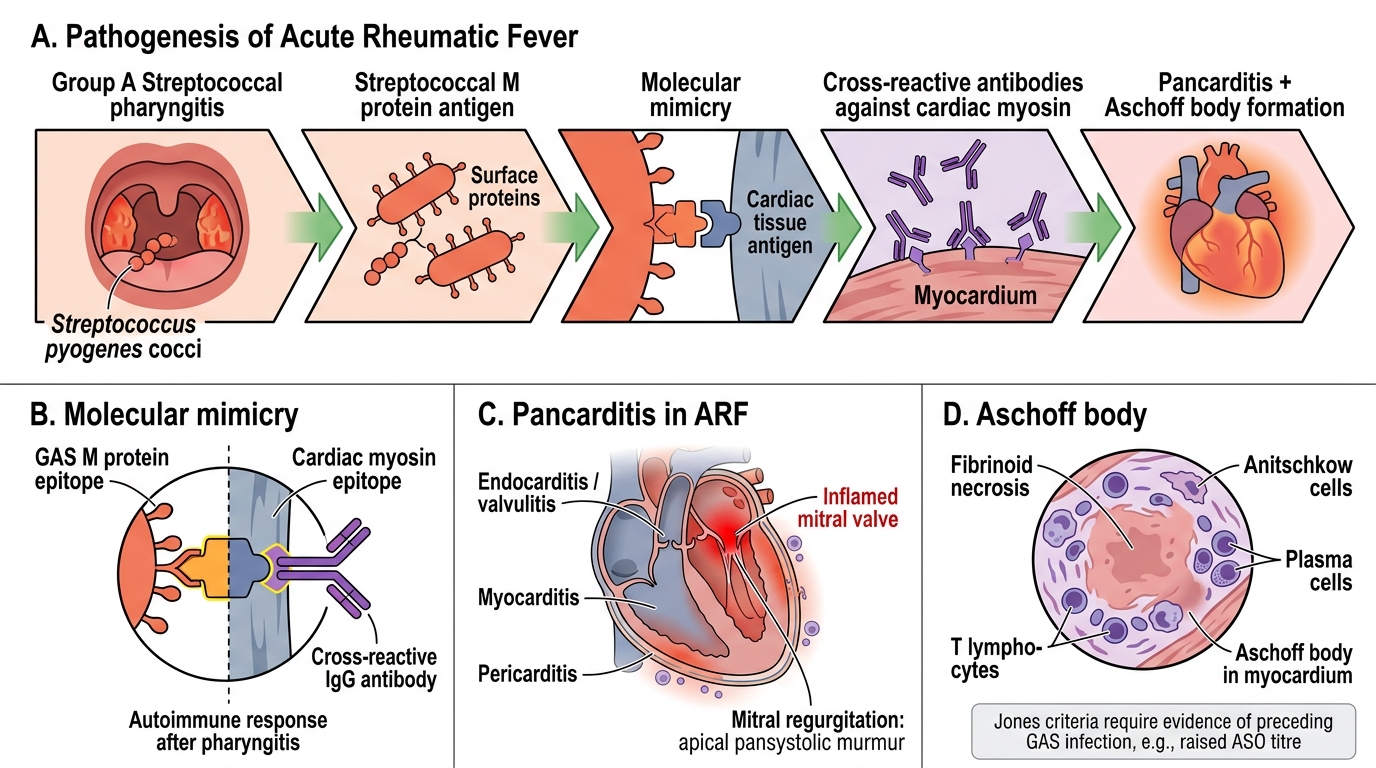
Acute rheumatic fever is the consequence of an autoimmune response to Group A streptococcal (GAS) pharyngitis in a genetically susceptible individual. The key insight is that ARF is not caused by direct bacterial invasion of the heart or joints — the GAS infection itself is confined to the throat — but by a cross-reactive immune response where antibodies and T cells generated against streptococcal antigens mistakenly attack structurally similar host proteins. This principle of molecular mimicry explains both the pathology and the fundamental logic of prevention: eradicate GAS from the throat before the immune response matures, and ARF cannot occur. Three conditions are required for ARF to develop, and understanding each informs a different aspect of prevention and treatment strategy.
Aetiology — required conditions for ARF:
- Group A Streptococcal pharyngitis: Only pharyngitis (NOT skin infection/impetigo) triggers ARF. This is because the pharyngeal immune response — with its abundant lymphoid tissue — generates the systemic autoimmune cascade. M protein, present on the streptococcal cell surface, is the primary virulence factor and molecular mimicry antigen.
- Genetic susceptibility: Only ~3% of individuals with untreated GAS pharyngitis develop ARF, indicating that host genetics play a crucial modifying role. HLA class II alleles (DR2, DR4, DR7) are associated with susceptibility.
- Immune dysregulation: B cells produce antibodies against GAS M protein; these cross-react with cardiac myosin (myocarditis), cardiac valve endothelium (valvulitis), brain basal ganglia (chorea), and joint synovium (arthritis). Molecular mimicry is the central mechanism.
Pathology of carditis:
- Aschoff body: the pathognomonic granulomatous lesion of rheumatic carditis — a central area of fibrinoid necrosis surrounded by histiocytes (Anitschkow myocytes with characteristic 'caterpillar' nuclei), giant cells, and lymphocytes. Found in the myocardium and pericardium.
- Valvulitis: the endocardial lining of valves becomes inflamed; small verrucae (warty vegetations) form along the line of valve closure, particularly the mitral valve. Repeated episodes cause progressive leaflet thickening, fusion of commissures, and shortening of chordae tendineae → mitral stenosis over years.
- Pericarditis: fibrinous pericarditis causes chest pain and pericardial friction rub; usually resolves without constriction.
Natural history:
Each GAS throat infection in a child with a prior history of ARF triggers a new episode of carditis, progressively damaging the valve with each episode. This is why secondary prophylaxis — preventing recurrent GAS infections — is the cornerstone of preventing RHD progression. The risk of carditis in recurrent ARF episodes is higher than in the first episode.
Acute Rheumatic Fever Pathogenesis
SELF-CHECK
A 10-year-old girl has fever (38.4°C), migratory arthritis of the knees and ankles, and a new apical pansystolic murmur. Her ASO titre is 280 Todd units. The ESR is 72 mm/h. Which combination of Jones criteria features does she fulfil?
A. Two major criteria only (arthritis + carditis) — no minor criteria
B. Two major criteria (arthritis + carditis) + two minor criteria (fever + elevated ESR) + evidence of preceding GAS (raised ASO)
C. One major criterion (carditis) + one minor criterion (fever) — not enough for diagnosis
D. Two major criteria alone are sufficient without evidence of preceding GAS
Reveal Answer
Answer: B. Two major criteria (arthritis + carditis) + two minor criteria (fever + elevated ESR) + evidence of preceding GAS (raised ASO)
Jones 2015 criteria for diagnosis of ARF: 2 major OR 1 major + 2 minor criteria, PLUS evidence of preceding GAS infection (raised ASO titre, positive throat culture, or rapid antigen test). She has 2 major (carditis + polyarthritis) + 2 minor (fever ≥38°C and elevated ESR ≥60 mm/h for high-risk populations) + evidence of preceding GAS (ASO 280 Todd units). This is a clear ARF diagnosis. Option D is incorrect — evidence of preceding GAS infection is mandatory regardless of the major criteria count.
Diagnosis — 2015 Jones Criteria
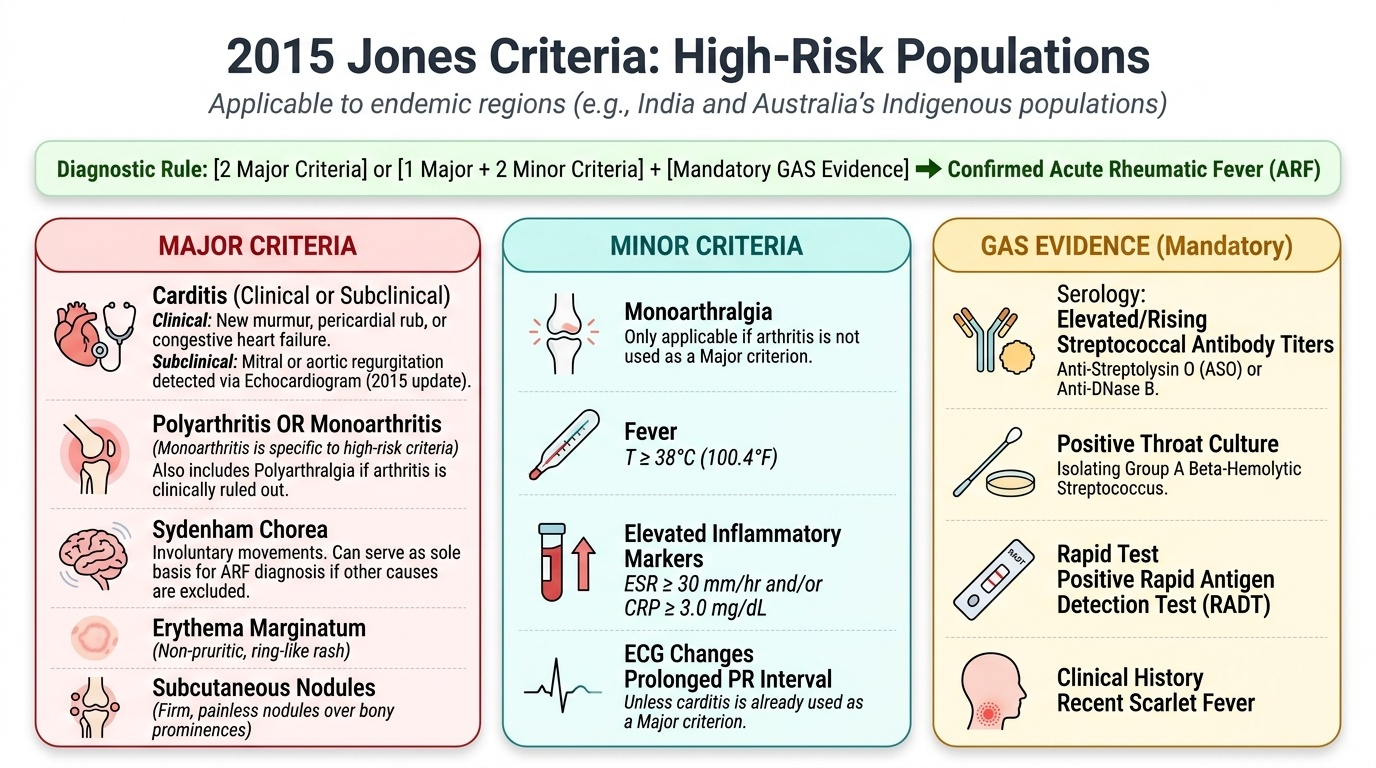
The Jones Criteria, originally proposed in 1944 and most recently revised in 2015 by the American Heart Association, provide the diagnostic framework for ARF. The 2015 revision is particularly important for India and other high-risk populations because it introduced two-tier criteria — a more sensitive set for high-risk populations (where ARF is endemic, such as Australia's Indigenous communities and India) and the original stricter criteria for low-risk populations. India is classified as a high-risk population, so the high-risk criteria apply. The diagnosis requires fulfilling the criteria AND demonstrating evidence of a preceding GAS infection — the criteria alone, without microbiological or serological evidence of recent streptococcal infection, do not constitute a diagnosis of ARF.
Provided image
Diagnosis of ARF (2015 Jones Criteria — HIGH-RISK populations, applicable to India):
Diagnosis = 2 major criteria, OR 1 major + 2 minor criteria + EVIDENCE of preceding GAS infection.
Major criteria:
1. Carditis — clinical (new murmur, pericardial rub, cardiac failure) or echocardiographic (subclinical carditis: mitral/aortic regurgitation on echo without audible murmur). Echo for subclinical carditis is a new major criterion in the 2015 revision for high-risk populations.
2. Polyarthritis — or monoarthritis in high-risk populations (Jones 2015 revision)
3. Sydenham chorea — can be the sole basis for ARF diagnosis (lone chorea) when occurring in a child without another explanation, even without elevated inflammatory markers
4. Erythema marginatum — evanescent, non-pruritic, central clearing rash on trunk/proximal limbs (not face)
5. Subcutaneous nodules — firm, painless, over bony prominences; associated with severe carditis
Minor criteria:
1. Monoarthralgia (not monoarthritis — arthralgia = pain without objective findings; only applicable if arthritis is NOT a major criterion)
2. Fever — ≥38.0°C for high-risk populations (≥38.5°C for low-risk)
3. Elevated ESR — ≥60 mm/h (high-risk) OR elevated CRP ≥3.0 mg/dL
4. Prolonged PR interval — beyond age-appropriate upper limit on ECG (cannot be counted if carditis is a major criterion)
Evidence of preceding GAS infection (all require at least ONE):
• Elevated or rising ASO titre (>200 Todd units in children)
• Positive throat culture for Group A Streptococcus
• Positive rapid antigen test for GAS
• Elevated anti-DNase B titre
Special situations:
• Lone chorea: ARF can be diagnosed on the basis of chorea alone without fulfilling other criteria, as chorea typically appears late (months after the acute infection) when ASO titres may have normalised.
• Insidious carditis: if rheumatic carditis presents slowly without other features, diagnosis requires echo-documented RHD in a high-prevalence setting + clinical judgement.
Investigations in ARF:
| Investigation | Finding in ARF | Significance |
|---|---|---|
| ASO titre | Elevated (>200 Todd units) | Evidence of preceding GAS |
| Throat culture | May be positive for GAS | Confirms active infection |
| ESR/CRP | Elevated | Minor criterion + disease activity |
| ECG | Prolonged PR interval | Minor criterion; monitor for heart block |
| Echocardiography | Mitral/aortic regurgitation | Diagnoses subclinical carditis; quantifies severity |
| Blood count | Neutrophilic leucocytosis | Non-specific acute inflammation |
CLINICAL PEARL
Sydenham chorea is its own diagnostic entity for ARF — it can be diagnosed as ARF even when fever has resolved, inflammatory markers have normalised, and ASO titre has returned to normal, because chorea manifests 3–6 months after the streptococcal infection. Do not dismiss chorea as 'unrelated' because the Jones minor criteria are not fulfilled. Any child presenting with choreiform movements should have echocardiography performed, because subclinical carditis co-exists in up to 70–80% of children with chorea — many of whom would otherwise be untreated and progress to RHD. This is one of the most clinically high-stakes points in the entire ARF framework.