Page 14 of 31
PE22.5 | Infective Endocarditis — SDL Guide
Learning Objectives
- Describe the pathogenesis and aetiology of infective endocarditis in children, including common organisms by clinical context
- Recognise the clinical features of infective endocarditis including peripheral stigmata and embolic complications
- Apply the modified Duke Criteria for diagnosis of infective endocarditis
- Outline the principles of management including empirical and organism-directed antibiotic therapy, surgical indications, and duration of treatment
- Prescribe antibiotic prophylaxis for high-risk CHD patients undergoing dental procedures
INSTRUCTIONS
Infective endocarditis in children is uncommon but life-threatening — and its presentation is often insidious, mimicking many other febrile illnesses. In a country where unrepaired CHD is prevalent and dental hygiene is variable, a final-year student must know how to recognise the combination of unexplained fever, new cardiac murmur, and embolic signs that should trigger the diagnostic workup. More importantly, understanding which children with CHD need antibiotic prophylaxis before dental procedures — and being able to prescribe it correctly — is a direct preventive action within your scope of practice from day one as a doctor.
References
- Ghai Essential Pediatrics, 9th edition, Ch 14 — Infective Endocarditis (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 465 — Infective Endocarditis (textbook)
- AHA 2015 Scientific Statement on Infective Endocarditis; ESC 2015 Guidelines on Infective Endocarditis (guidelines)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 10-year-old boy with a known repaired Tetralogy of Fallot attends a dental extraction 3 weeks ago without antibiotic prophylaxis. He now presents with 10 days of unexplained fever (38.8°C), progressive fatigue, and weight loss. On examination: new grade 3/6 aortic regurgitation murmur not present at his last cardiac review 6 months ago; splenomegaly; and you notice small, painful, reddish-purple nodules on the pads of his fingertips. The nurse asks you to request blood cultures. How many sets do you take and from which sites? How do you interpret the Duke Criteria? What antibiotic regimen do you start — and for how long? Could this admission have been prevented?
WHY THIS MATTERS
Infective endocarditis (IE) is a microbial infection of the endocardial surface of the heart, most commonly involving the cardiac valves. While IE affects adults and children, children with congenital heart disease (CHD) are at substantially elevated risk — particularly those with residual haemodynamic defects after surgical repair, prosthetic valves or conduits, or unrepaired cyanotic CHD. In India, rheumatic heart disease adds another major predisposing category. IE is a condition where delay in diagnosis is fatal — vegetations fragment and embolise to the brain (stroke), kidneys (renal infarction), and other organs, and valve destruction progresses rapidly with aggressive organisms. Understanding the clinical picture, the diagnostic criteria, and the specific blood culture technique required for diagnosis is a core clinical competency. IE is largely preventable with antibiotic prophylaxis in the highest-risk CHD patients, and prescribing that prophylaxis correctly is a straightforward, high-impact action.
RECALL
Before proceeding, consolidate these prior concepts:
- Cardiac anatomy (AN): valves — mitral (left AV), tricuspid (right AV), aortic (left ventricular outflow), pulmonary (right ventricular outflow). Sites of turbulent blood flow in CHD (VSD jets, stenotic outflow tracts) create endothelial damage where bacteria lodge.
- Streptococcus viridans (Microbiology): alpha-haemolytic oral streptococcus; normal flora of the mouth; enters bloodstream during dental procedures; most common cause of subacute IE on pre-damaged valves.
- Staphylococcus aureus (Microbiology): coagulase-positive; causes acute, fulminant endocarditis; associated with skin infections, IV catheters, post-cardiac surgery; MRSA strains require vancomycin.
- Bacteraemia: transient bacteraemia occurs with dental procedures (tooth extraction, scaling), upper GI endoscopy, bronchoscopy; in high-risk CHD, these procedures carry IE risk without prophylaxis.
- Group A Streptococcal carditis (from ARF module): rheumatic valve disease creates structurally abnormal valves — a major risk factor for superimposed IE.
Clinical Presentation of Infective Endocarditis
Infective endocarditis presents as a combination of systemic features of infection (fever, constitutional symptoms), direct cardiac manifestations (new or changing murmur, cardiac failure), and the distinctive peripheral features that result from either immune complex deposition or septic embolism. The clinical picture varies dramatically depending on the causative organism — subacute IE from Streptococcus viridans produces a smouldering, weeks-long febrile illness with gradual development of peripheral stigmata, while acute IE from Staphylococcus aureus produces a rapid, toxic, life-threatening presentation within days. Recognising both ends of this spectrum — and understanding that a child with unexplained fever and a cardiac murmur for more than a week must have blood cultures before antibiotics are started — is the clinical entry point this section provides.
Constitutional features:
• Fever — present in virtually all cases; may be high-grade and swinging (acute, Staph aureus) or low-grade and persistent (subacute, Streptococcus viridans)
• Weight loss, anorexia, fatigue, malaise
• Night sweats, myalgia, arthralgia
Cardiac features:
• New murmur or change in character of a pre-existing murmur — the single most important clinical finding; reflects valvular regurgitation from vegetation or valve leaflet destruction
• Signs of cardiac failure (tachycardia, gallop, hepatomegaly) if valve destruction is severe
• Pericardial friction rub if pericarditis from myocardial abscess extending to pericardium
Peripheral stigmata of IE (result of immune complex deposition or septic embolism):
• Osler nodes: painful, tender, reddish-purple nodules on the pads of fingers and toes — caused by immune complex deposition (NOT septic emboli); last days; characteristic of subacute IE
• Janeway lesions: non-tender, flat haemorrhagic macules on palms and soles — caused by septic emboli; characteristic of acute IE (Staph aureus)
• Splinter haemorrhages: linear reddish-brown streaks under the fingernails (mid-nail); non-specific but part of the peripheral picture
• Roth spots: oval retinal haemorrhages with pale centres on fundoscopy; caused by immune complexes in retinal vessels; examined by ophthalmoscopy
• Clubbing: digital clubbing occurs in prolonged (months) subacute IE; also seen in CHD
• Petechiae: conjunctival petechiae, petechiae on the soft palate and buccal mucosa
Embolic phenomena (major Duke minor criterion — vascular phenomena):
• Stroke (cerebral embolism) — most feared; focal neurological deficit, seizures, altered consciousness
• Splenic infarction — left upper quadrant pain
• Renal infarction — flank pain, haematuria
• Pulmonary embolism (right-sided IE — tricuspid valve, associated with IV catheters/drug use)
• Splenomegaly — subacute IE; due to reticuloendothelial system hyperactivation
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
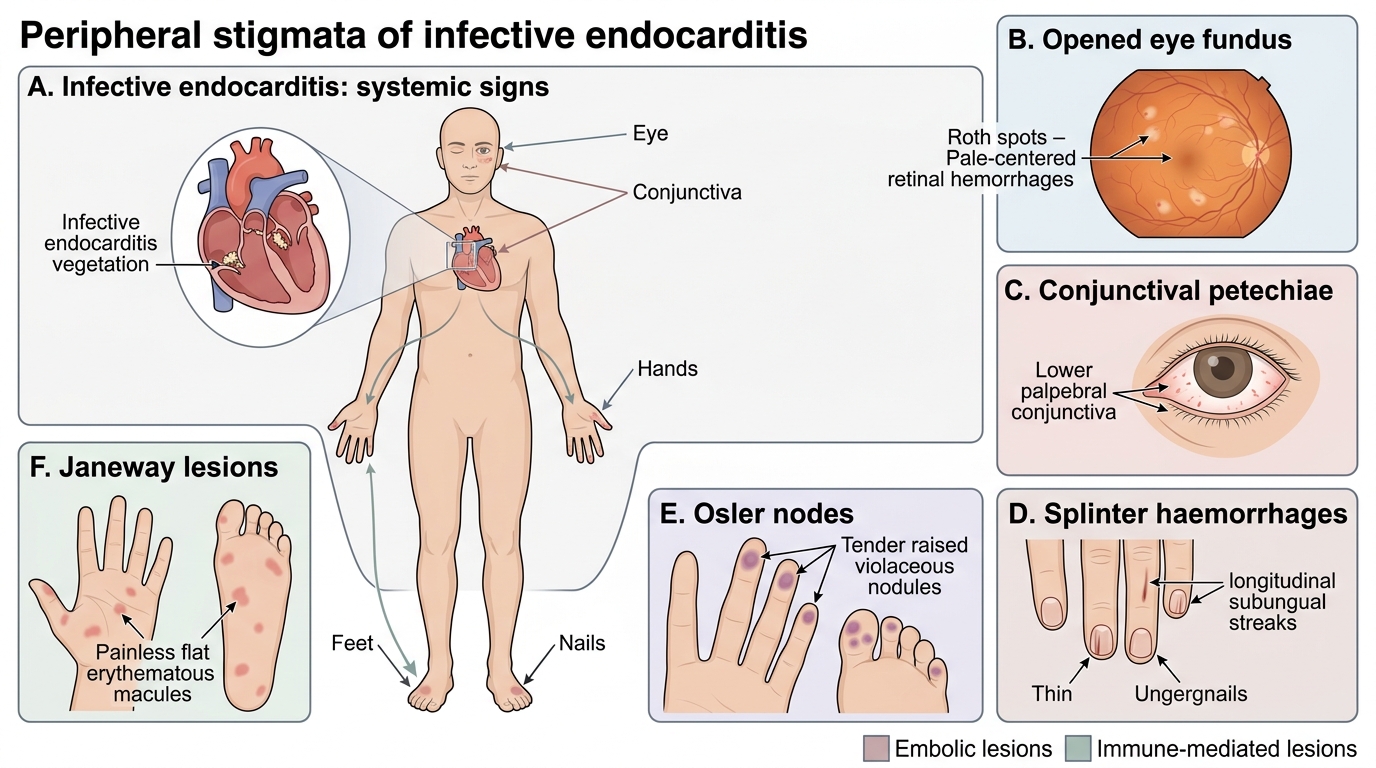
Peripheral Stigmata of Infective Endocarditis
Pathogenesis and Aetiology
The pathogenesis of infective endocarditis follows a predictable sequence beginning with endothelial damage and culminating in the formation of a platelet-fibrin-bacteria complex — the vegetation — on the endocardial surface. Understanding this sequence is essential because it explains both the predisposing conditions that increase IE risk and the targets for prophylaxis and treatment. The type of bacterium determines whether the disease is acute (days) or subacute (weeks), and the anatomical site of vegetation formation is determined by the haemodynamic context — where turbulent blood flow impinges on the endothelium, that is where bacteria lodge. This means that in a child with a VSD, the vegetation forms on the right ventricular wall at the site of the high-velocity jet impact, not randomly on any valve surface.
Pathogenesis sequence:
- Endothelial damage: turbulent blood flow (across a stenotic valve, a VSD jet, a prosthetic valve) injures the endothelial lining, exposing sub-endothelial collagen and tissue factor.
- Platelet-fibrin nidus: platelets and fibrin deposit on the denuded endothelial surface, forming a non-bacterial thrombotic endocarditis (NBTE) — a sterile nidus ready for bacterial seeding.
- Bacteraemia: transient bacteraemia from a portal of entry (dental procedure, IV catheter, skin infection, gut) seeds the bloodstream with organisms that have surface proteins (e.g. streptococcal dextran, staphylococcal fibronectin-binding proteins) that adhere to the platelet-fibrin matrix.
- Vegetation formation: bacteria proliferate within the platelet-fibrin matrix, forming an ever-enlarging, relatively avascular vegetation that is protected from host defences and antibiotic penetration — explaining the requirement for prolonged IV therapy.
- Consequences: local valve destruction (regurgitation, perforation), extension to annulus or myocardium (abscess), and fragmentation of vegetation → embolism to brain, kidneys, spleen, lungs (right-sided).
Organisms by clinical context:
| Clinical context | Common organisms |
|---|---|
| Pre-existing CHD or rheumatic heart disease | Streptococcus viridans (most common); Streptococcus bovis |
| Post-cardiac surgery / prosthetic valve | Staphylococcus aureus, Staphylococcus epidermidis (coagulase-negative), Candida |
| IV catheters / PICU / neonates | Staphylococcus aureus, coagulase-negative staphylococci, Candida |
| Culture-negative IE | HACEK organisms, Coxiella burnetii (Q fever), Bartonella |
| Community-acquired, normal valve | Staphylococcus aureus (acute, destructive) |
Risk factors for IE in children:
• Structural CHD (highest risk: cyanotic CHD with residual shunts, prosthetic valves/conduits, previous IE)
• Rheumatic heart disease (damaged mitral/aortic valves)
• Indwelling vascular catheters (central venous lines, ports) — most common risk factor in neonates and PICU patients
• Dental procedures without prophylaxis in high-risk CHD
• IV drug use (uncommon in children; causes right-sided/tricuspid IE)
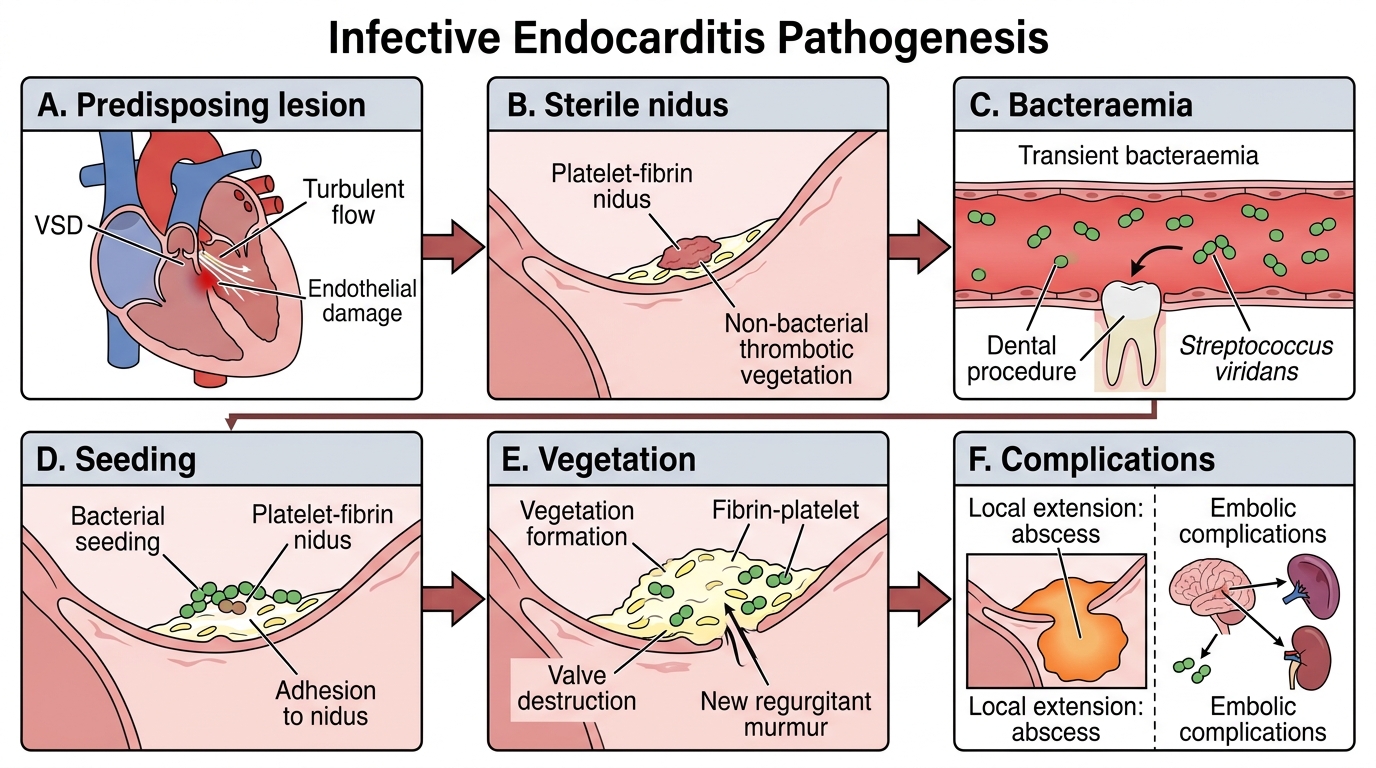
Pathogenesis of Infective Endocarditis
SELF-CHECK
A 12-year-old with unrepaired VSD has had 2 weeks of fever, weight loss, and a new aortic regurgitation murmur. His dentist did not give prophylaxis 3 weeks ago. Which organism is MOST likely responsible?
A. Staphylococcus aureus
B. Streptococcus viridans
C. Candida albicans
D. Pseudomonas aeruginosa
Reveal Answer
Answer: B. Streptococcus viridans
Streptococcus viridans is the most common cause of subacute infective endocarditis in children with pre-existing structural CHD following a dental procedure. The subacute presentation (2 weeks of low-grade fever, weight loss) and the temporal link to a dental procedure without prophylaxis are classic. Staph aureus causes acute, fulminant IE (usually days, not weeks) and is more common with IV catheters or skin infections. Candida causes IE mainly in immunocompromised or post-cardiac surgery patients.
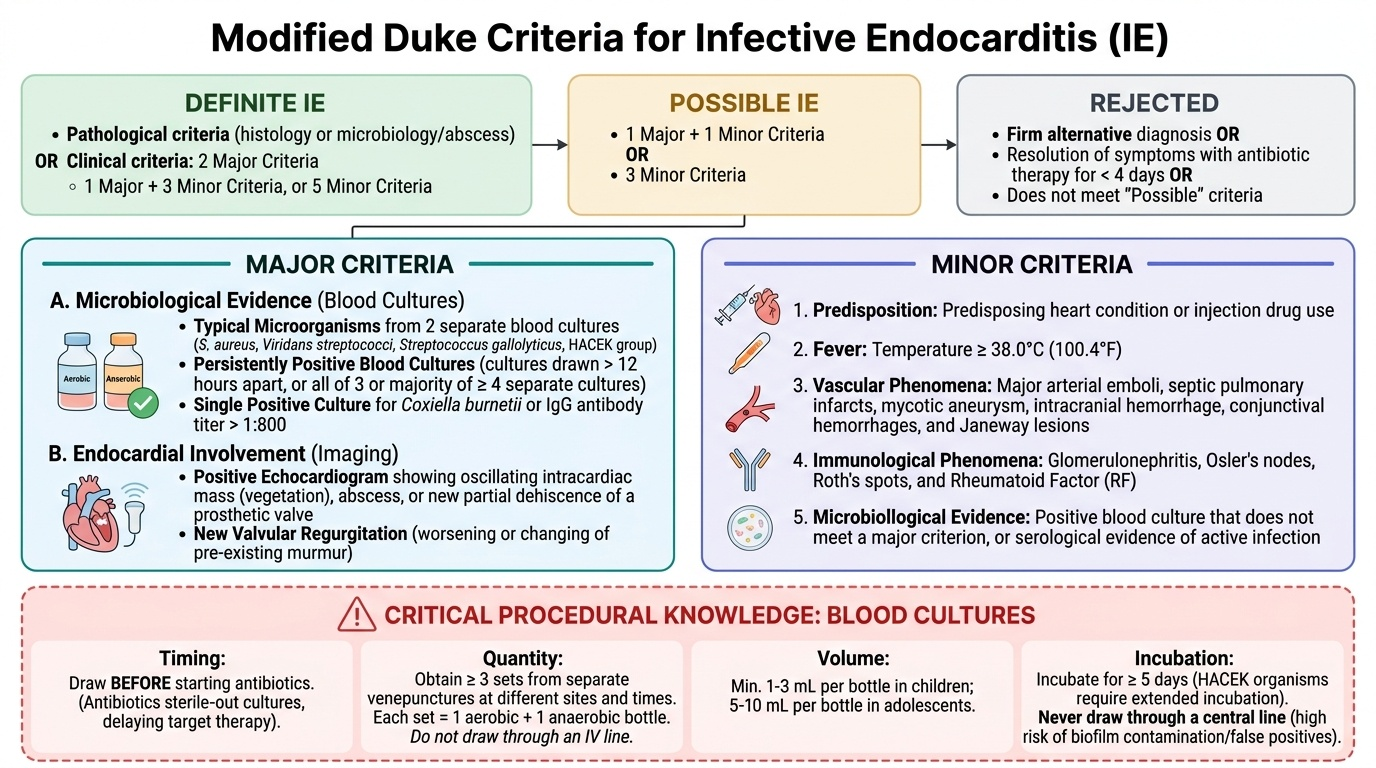
Diagnosis — Modified Duke Criteria
The diagnosis of infective endocarditis rests on a combination of clinical findings, microbiological results, and echocardiographic evidence, formalised in the modified Duke Criteria (originally proposed 1994, modified 2000). These criteria provide a structured diagnostic framework that classifies patients as definite, possible, or rejected IE based on the combination of major and minor criteria. Blood cultures — taken in the correct manner, before any antibiotic is administered — are the most important investigation in IE, and the single most common error in IE diagnosis is starting antibiotics before blood cultures are obtained. Once antibiotics are given, cultures may remain sterile for weeks, making organism identification (and therefore targeted therapy) impossible — and delaying antibiotics by 30–60 minutes to obtain cultures in a stable patient is always the right trade-off.
Provided image
Blood culture technique (critical procedural knowledge):
• Obtain a minimum of 3 sets of blood cultures from 3 separate venepunctures at different sites and times (not drawn through an IV line)
• Each set = one aerobic + one anaerobic bottle
• Volume: minimum 1–3 mL per bottle in children; 5–10 mL per bottle in adolescents
• Incubate for a minimum of 5 days; HACEK organisms require extended incubation
• Never draw through a central line for diagnostic blood cultures (false positives from biofilm)
Modified Duke Criteria:
MAJOR criteria:
1. Positive blood culture — either:
- Two separate blood cultures growing a typical IE organism (Streptococcus viridans, Streptococcus bovis, HACEK organisms, Staphylococcus aureus, community-acquired enterococci)
- Persistently positive blood cultures (≥2 positive cultures >12 h apart, OR all 3 or majority of ≥4 cultures positive)
- Single positive culture for Coxiella burnetii (or anti-phase 1 IgG antibody titre >1:800)
2. Evidence of endocardial involvement — either:
- Positive echocardiogram: vegetation (oscillating intracardiac mass on valve/endocardium), abscess, new partial dehiscence of prosthetic valve
- New valvular regurgitation on echocardiography
MINOR criteria:
1. Predisposing heart condition (CHD, RHD, prosthetic valve) or IV drug use
2. Fever ≥38°C
3. Vascular phenomena: arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial haemorrhage, conjunctival haemorrhages, Janeway lesions
4. Immunological phenomena: glomerulonephritis, Osler nodes, Roth spots, positive rheumatoid factor
5. Microbiological evidence not meeting major criterion (positive blood culture with non-typical organism, or serological evidence of active infection)
Diagnosis:
| Category | Criteria |
|---|---|
| Definite IE | 2 major, OR 1 major + 3 minor, OR 5 minor |
| Possible IE | 1 major + 1 minor, OR 3 minor |
| Rejected | Firm alternative diagnosis, OR resolution with antibiotics ≤4 days, OR no pathological evidence at surgery/autopsy |
Additional investigations:
• Echocardiography — transthoracic echo (TTE) first-line in children (excellent acoustic windows); transoesophageal echo (TOE) if TTE inadequate or prosthetic valve
• ESR, CRP — elevated (disease activity markers, not diagnostic)
• Complete blood count — anaemia (of chronic disease), leucocytosis (acute) or leucopenia (severe)
• Urine analysis — haematuria (renal emboli/immune complex glomerulonephritis)
• Rheumatoid factor — may be positive (immune complex deposition); minor criterion
CLINICAL PEARL
Blood cultures before antibiotics is the most important action in suspected IE — and the most commonly violated rule. Sending blood cultures after starting antibiotics renders the results uninterpretable in up to 60% of cases. The correct approach when IE is suspected in a clinically stable child is to take 3 sets of blood cultures from 3 separate venepunctures over 30–60 minutes, and THEN start antibiotics. In a haemodynamically unstable child where immediate antibiotic treatment cannot be delayed, take 2 sets within 15 minutes before starting empirical therapy. The number 3 — three separate sets, three separate venesection sites — is the minimum requirement for adequate sensitivity.