Page 18 of 31
PE22.6 | Pediatric Hypertension — SDL Guide (Part 2)
Investigation of Paediatric Hypertension
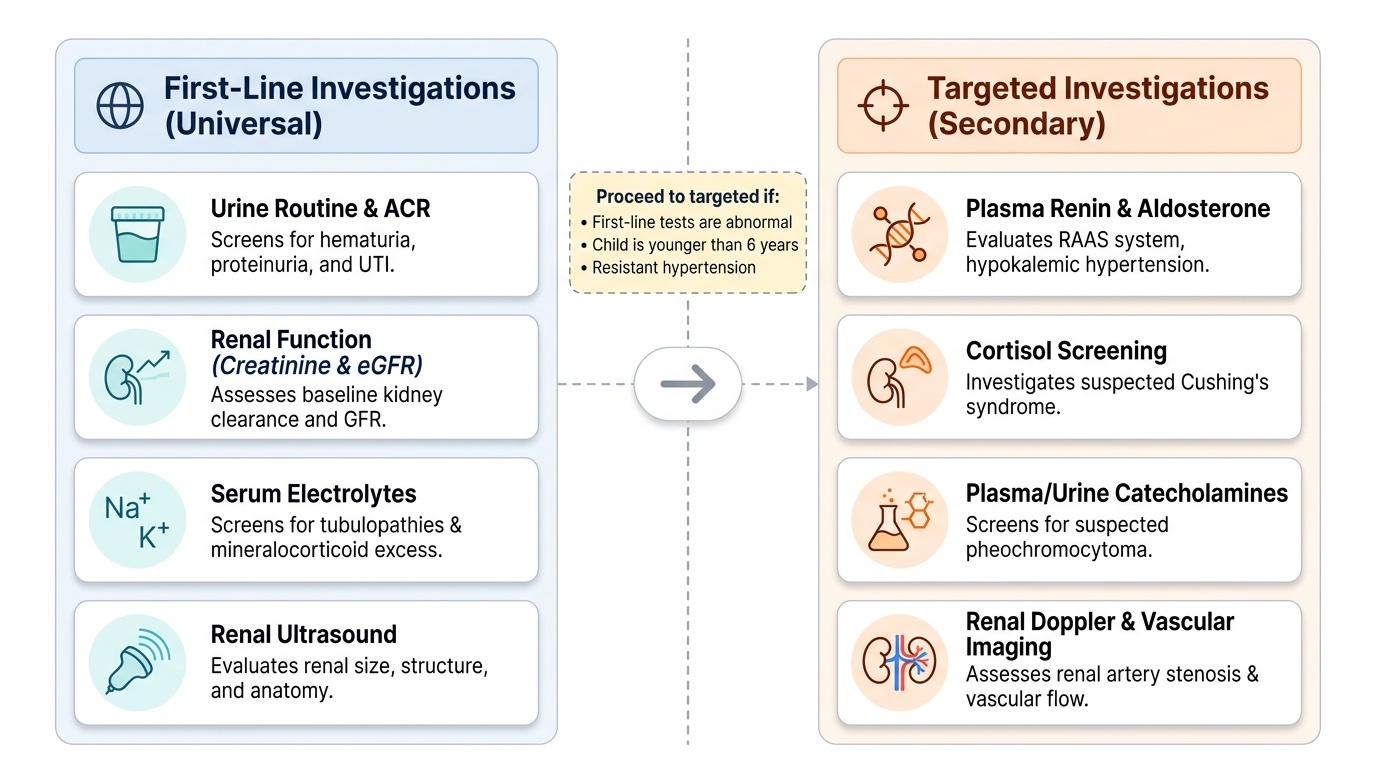
The investigative strategy for paediatric hypertension is guided by the child's age, the severity of hypertension, the clinical findings, and the likelihood of secondary cause. A systematic, step-wise approach avoids both under-investigation — which means missing a correctable secondary cause — and over-investigation, which subjects an obese adolescent with likely primary hypertension to unnecessary invasive tests. In any child younger than six years with confirmed hypertension, the probability of a secondary cause is high enough that a comprehensive secondary workup is mandatory from the outset. In adolescents with obesity and a positive family history, a more targeted initial screen is appropriate, proceeding to deeper investigation only if first-line tests are abnormal or hypertension fails to respond to lifestyle management. The workup is conceptually divided into two tiers: a universal first-line panel performed in every child with confirmed hypertension, and a targeted secondary workup ordered according to the suspected aetiology suggested by first-line findings and clinical clues.
Provided image
First-line investigations for all children with confirmed hypertension: These baseline tests are done to assess end-organ damage and screen for the most common secondary causes.
- Urine routine microscopy and culture: haematuria and proteinuria suggest glomerulonephritis or chronic kidney disease; pyuria suggests a urinary tract infection
- Urine albumin-to-creatinine ratio (ACR) or 24-hour urine protein: quantify proteinuria
- Serum creatinine and eGFR: assess renal function
- Serum electrolytes (Na⁺, K⁺): hypokalaemia suggests hyperaldosteronism or excess mineralocorticoid; hypernatraemia or hyponatraemia may point to specific tubulopathies
- Fasting blood glucose: obesity-related primary hypertension is associated with insulin resistance
- Lipid profile: cardiometabolic risk stratification
- Renal ultrasound with Doppler: assess renal size, cortical echogenicity, corticomedullary differentiation, collecting-system dilatation; identify structural anomalies; Doppler assesses renal artery flow
- Echocardiography: assess for left-ventricular hypertrophy (LVH), which is both the most important hypertensive target-organ finding in children and an indication for antihypertensive therapy; also assess for coarctation
- ECG: may show LVH voltage criteria
- Fundoscopy: hypertensive retinopathy
- Chest X-ray: cardiomegaly, rib notching (coarctation)
Targeted secondary workup — ordered when first-line suggests a specific cause:
- Plasma renin activity and aldosterone (renovascular hypertension, hyperaldosteronism — note: low renin with high aldosterone = primary hyperaldosteronism)
- 24-hour urine catecholamines or plasma metanephrines (phaeochromocytoma)
- 24-hour urine cortisol or low-dose dexamethasone suppression test (Cushing's)
- Serum 17-hydroxyprogesterone (congenital adrenal hyperplasia)
- Thyroid function tests (hyperthyroidism)
- Antinuclear antibody (ANA), anti-dsDNA, complement C3/C4 (lupus nephritis)
- Anti-streptolysin O (ASO) titre, complement (post-streptococcal glomerulonephritis)
- CT angiography or MR angiography of renal arteries (renovascular — when Doppler is inconclusive)
- DMSA scan (cortical scars from reflux nephropathy)
CLINICAL PEARL
In children under 6 years with any degree of hypertension, always work up for secondary causes before labelling as primary hypertension. The most common mistake is attributing hypertension to 'anxiety' or 'white-coat effect' in a child with persistent proteinuria — this combination virtually always indicates renal parenchymal disease. Also remember: a difference of >10–20 mmHg between upper and lower limb blood pressures (or radio-femoral delay) is diagnostic of coarctation of the aorta until proven otherwise — do not miss this eminently correctable surgical cause. Lastly, correct cuff size is non-negotiable: an adult cuff on a child's arm is the leading cause of falsely elevated BP readings in paediatric practice.
SELF-CHECK
A 7-year-old child has blood pressure 138/90 mmHg on three separate occasions. His 95th percentile for age, sex, and height is 112/74 mmHg, and the 99th percentile is 120/80 mmHg. Which stage of hypertension does this represent?
A. Elevated blood pressure (90th–95th percentile)
B. Stage 1 hypertension (95th–99th + 5 mmHg)
C. Stage 2 hypertension (>99th percentile + 5 mmHg)
D. Hypertensive emergency requiring immediate IV therapy
Reveal Answer
Answer: C. Stage 2 hypertension (>99th percentile + 5 mmHg)
This child's BP of 138/90 mmHg is well above his 99th percentile (120/80 mmHg) plus the additional 5 mmHg threshold — it is therefore Stage 2 hypertension. Stage 1 is defined as 95th–99th percentile + 5 mmHg; Stage 2 is above the 99th percentile + 5 mmHg. While the BP is significantly elevated, this would be a hypertensive emergency only if associated with acute end-organ damage (encephalopathy, acute LVF, acute renal failure) — not just on the number alone. This child needs urgent workup for secondary causes.
Management of Paediatric Hypertension
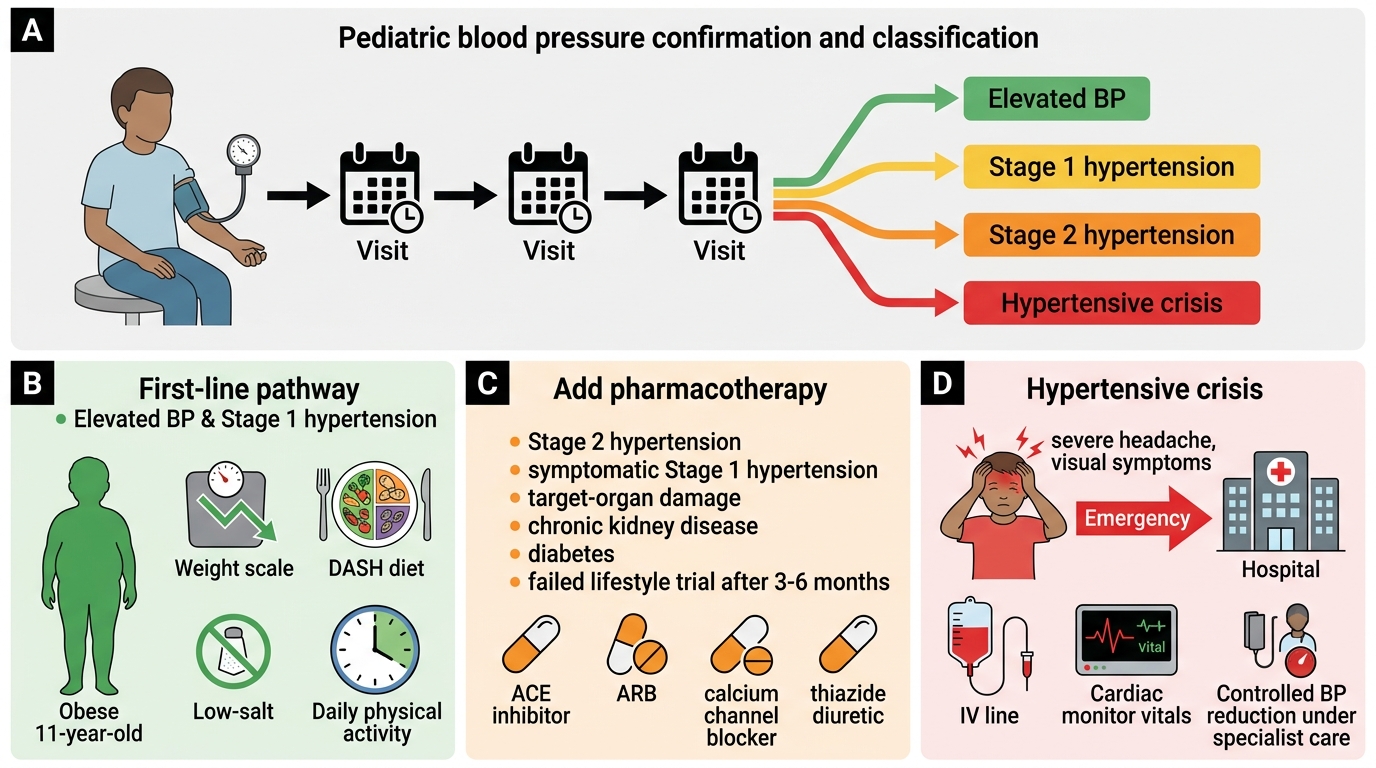
Management of paediatric hypertension is guided by the stage of hypertension, the presence of symptoms, the identification of a secondary cause, and the presence of target-organ damage. The fundamental principle is: treat the cause when found, and apply lifestyle intervention as the foundation of all management. Unlike adult hypertension, where pharmacotherapy is often started promptly, paediatric management is strongly guided by the likely aetiology — an obese teenager with primary hypertension and no target-organ damage has a very different treatment pathway from a 7-year-old with stage 2 hypertension and nephrotic syndrome. The management framework therefore requires the clinician to integrate BP stage, age, aetiology, the presence of end-organ damage, and the available evidence base for safety of antihypertensive drugs in children, where pharmacokinetic data are often more limited than in adults.
Non-pharmacological management (lifestyle modification): For elevated BP and Stage 1 hypertension without target-organ damage or secondary cause, lifestyle modification is the first-line intervention for 3–6 months before considering pharmacotherapy.
- Weight management: achieving a healthy weight (BMI <85th percentile) is the single most effective intervention in overweight and obese children with primary hypertension
- Dietary modification: DASH (Dietary Approaches to Stop Hypertension) diet — increased fruits, vegetables, whole grains, low-fat dairy; reduced saturated fats and sodium. Sodium restriction to <1,500 mg/day is recommended
- Physical activity: ≥60 minutes of moderate-to-vigorous physical activity daily — aerobic exercise reduces BP by 4–5 mmHg
- Avoidance of triggers: cessation of medications contributing to hypertension (NSAIDs, stimulants, OCP); reduction of screen time; stress management
Pharmacological management: Antihypertensive drug therapy is indicated in:
- Stage 2 hypertension at any age
- Stage 1 hypertension with symptomatic episodes, hypertensive emergency, target-organ damage (LVH, proteinuria), secondary aetiology, or failed lifestyle modification after 3–6 months
- Diabetes mellitus with any hypertension (proteinuria risk)
First-line agents commonly used in children (chosen based on aetiology and safety profile):
- ACE inhibitors (enalapril, lisinopril) — preferred when proteinuria is present (nephroprotective); weight-based dosing; contraindicated in pregnancy, bilateral renal artery stenosis, and hyperkalaemia
- ARBs (losartan, irbesartan) — alternative to ACEi with better tolerability (no cough); similar indications
- Calcium channel blockers — CCBs (amlodipine) — useful in children with renal disease, not dependent on renin; good safety profile in children; preferred in renovascular hypertension (ACEi can worsen renal function in bilateral RAS)
- Beta-blockers (atenolol, metoprolol) — used for high sympathetic tone or associated cardiac indications; may mask hypoglycaemia signs in insulin-dependent diabetes
- Diuretics (hydrochlorothiazide, chlorthalidone) — volume-dependent hypertension; useful in chronic kidney disease
All paediatric antihypertensives are dosed by weight (mg/kg) — never use adult fixed doses.
Hypertensive emergency management: Goal is controlled, gradual reduction of BP — rapid reduction risks cerebral ischaemia (due to loss of autoregulation in chronic hypertension).
- Target: reduce mean arterial pressure by no more than 25% in the first 8 hours, then normalise over 24–48 hours
- IV labetalol (alpha and beta blocker) — first-line IV agent in most paediatric hypertensive emergencies; bolus or infusion
- IV sodium nitroprusside — for immediate action when IV labetalol is insufficient; short-acting, titratable; risk of cyanide toxicity with prolonged use
- Oral nifedipine (immediate-release) — used in less-emergent scenarios; note: sublingual nifedipine is no longer recommended due to unpredictable absorption and risk of precipitous BP drop
- IV hydralazine — older agent, still used; unpredictable response
- Identify and treat the underlying cause urgently
- Neurology and nephrology input for encephalopathy and renal failure
Secondary hypertension management: Definitive treatment of the underlying cause may normalise BP. Coarctation → surgical repair or balloon angioplasty; renal artery stenosis → angioplasty ± stenting; phaeochromocytoma → surgical excision after alpha-blockade; CAH → steroid replacement; GN → immunosuppression per protocol. Persistent hypertension after correction still requires antihypertensive therapy.
Step-wise Management of Paediatric Hypertension
SELF-CHECK
An 11-year-old obese girl has Stage 1 hypertension confirmed on three occasions, without symptoms, proteinuria, or target-organ damage. Secondary causes have been excluded. What is the most appropriate initial management?
A. Start ACE inhibitor immediately given confirmed hypertension
B. Lifestyle modification for 3–6 months — weight reduction, DASH diet, physical activity
C. Initiate amlodipine because calcium channel blockers are the safest class in childhood
D. Refer for renal biopsy to exclude parenchymal disease before any treatment
Reveal Answer
Answer: B. Lifestyle modification for 3–6 months — weight reduction, DASH diet, physical activity
For Stage 1 hypertension without symptoms, target-organ damage, or secondary cause in a child with obesity, lifestyle modification is the first-line intervention and should be attempted for 3–6 months before considering pharmacotherapy. This includes weight management (most effective single intervention), DASH diet with sodium restriction, and at least 60 minutes of moderate-to-vigorous physical activity daily. Pharmacotherapy is added if lifestyle modification fails, or immediately for Stage 2 hypertension, symptomatic cases, or when target-organ damage is present.
Self-Assessment
Use the following questions to consolidate your learning. Think through each carefully before revealing the answer — the aim is to apply the complete clinical framework you have built.
Question 1: A 4-year-old boy presents with BP 150/100 mmHg on three occasions. He has haematuria and mild oedema. What is the most likely diagnosis and what first-line investigation would you order?
Think: Young child, confirmed hypertension, haematuria + oedema — this is almost certainly secondary, most likely renal parenchymal disease (post-infectious glomerulonephritis or chronic kidney disease). First-line investigation: urine routine + microscopy, urine culture, serum creatinine, renal ultrasound, ASO titre and complement levels (to evaluate for post-streptococcal GN).
Question 2: How would you confirm that BP 115/75 mmHg in a 10-year-old girl represents 'elevated BP' rather than 'normal'?
Think: You cannot determine this without knowing her height. Look up the percentile table for age 10, female sex, and her specific height centile. If 115/75 falls between the 90th and 95th percentile for her parameters — or is ≥120/80 mmHg (whichever is lower) — it is elevated BP. Repeat on two more occasions.
Question 3: Why is reducing a child's BP from 180/120 to 120/80 mmHg over 30 minutes dangerous even though both values are 'normal' in different contexts?
Think: Chronic hypertension shifts the cerebral autoregulation curve to the right. Rapid reduction in BP — even to a 'normal' level — can drop the perfusion pressure below the lower limit of autoregulation, causing cerebral ischaemia. The safe protocol is to reduce MAP by no more than 25% in the first 8 hours, then normalise over 24–48 hours with IV agents and careful titration.