Page 10 of 42
PE23.{4,6-8} | Acute Gastroenteritis — SDL Guide
Learning Objectives
- Define diarrhoea and classify acute gastroenteritis by duration, aetiology, and stool character
- Describe the aetiology, risk factors, pathophysiology, and complications of acute gastroenteritis in children
- Assess and classify dehydration in a child with diarrhoea using the IMNCI framework
- Perform and interpret a Hanging Drop Preparation for stool examination; interpret RFT and electrolytes in the context of diarrhoea
- Explain the physiological basis of oral rehydration therapy; prescribe the correct ORS plan (A, B, or C) based on dehydration assessment
- Apply evidence-based pharmacological management including zinc supplementation and targeted antibiotic use
INSTRUCTIONS
Diarrhoeal disease kills more than 500,000 children under 5 years in developing countries every year, and India bears a disproportionate burden. Yet the majority of these deaths are preventable with a simple, inexpensive intervention — oral rehydration therapy. The science behind ORS is elegant: it exploits a sodium-glucose cotransporter that remains functional even when cholera toxin has turned off all other sodium absorption. Understanding this physiology, and being able to assess, classify, and manage dehydration at the bedside, is the core of this module — and a core of paediatric clinical competence.
References
- Ghai Essential Pediatrics, 9th edition, Ch 16 (Gastrointestinal system — Diarrhoeal diseases) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 366 (Acute gastroenteritis in children) (textbook)
- WHO/UNICEF 2004 — Clinical Management of Acute Diarrhoea (ORS and Zinc treatment) (guidelines)
- IMNCI (Integrated Management of Neonatal and Childhood Illness) module — Diarrhoea classification and treatment (guidelines)
- IAP Guidelines on Management of Acute Diarrhoea in Children (guidelines)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
An 18-month-old boy is brought to the rural primary health centre at 10 PM. His mother says he has had 10-12 watery stools since morning and is refusing to drink. On examination, his eyes appear sunken, he looks lethargic and does not cry when you examine him. When you pinch the skin of his abdomen it takes more than 2 seconds to return to its original position. His fontanelle is sunken. His urine output has been minimal for the last 6 hours.
You have no IV fluids at this facility — only packets of ORS. Is this child's condition too severe for ORS, or is there a safe way to rehydrate him orally? What does the skin pinch test tell you — and what does the WHO say you should do next?
The answers to these questions have saved hundreds of thousands of children's lives. They are also the questions this module will equip you to answer at any bedside, with or without IV access.
WHY THIS MATTERS
Diarrhoeal diseases remain among the leading causes of under-5 mortality globally and in India. The estimated 13 deaths per 1,000 live births attributable to diarrhoea in India represent a preventable tragedy — preventable because the cornerstone treatment, oral rehydration salts (ORS), costs less than ₹5 per packet. Yet ORS remains underused and misused (diluted incorrectly, stopped too early, replaced by 'anti-diarrhoeal' medications that are at best ineffective and at worst harmful). The ability to correctly classify dehydration using IMNCI criteria, prescribe the correct ORS plan, add zinc supplementation, and recognise when IV fluids and antibiotics are genuinely needed defines the competent front-line doctor in any primary or secondary care setting in India.
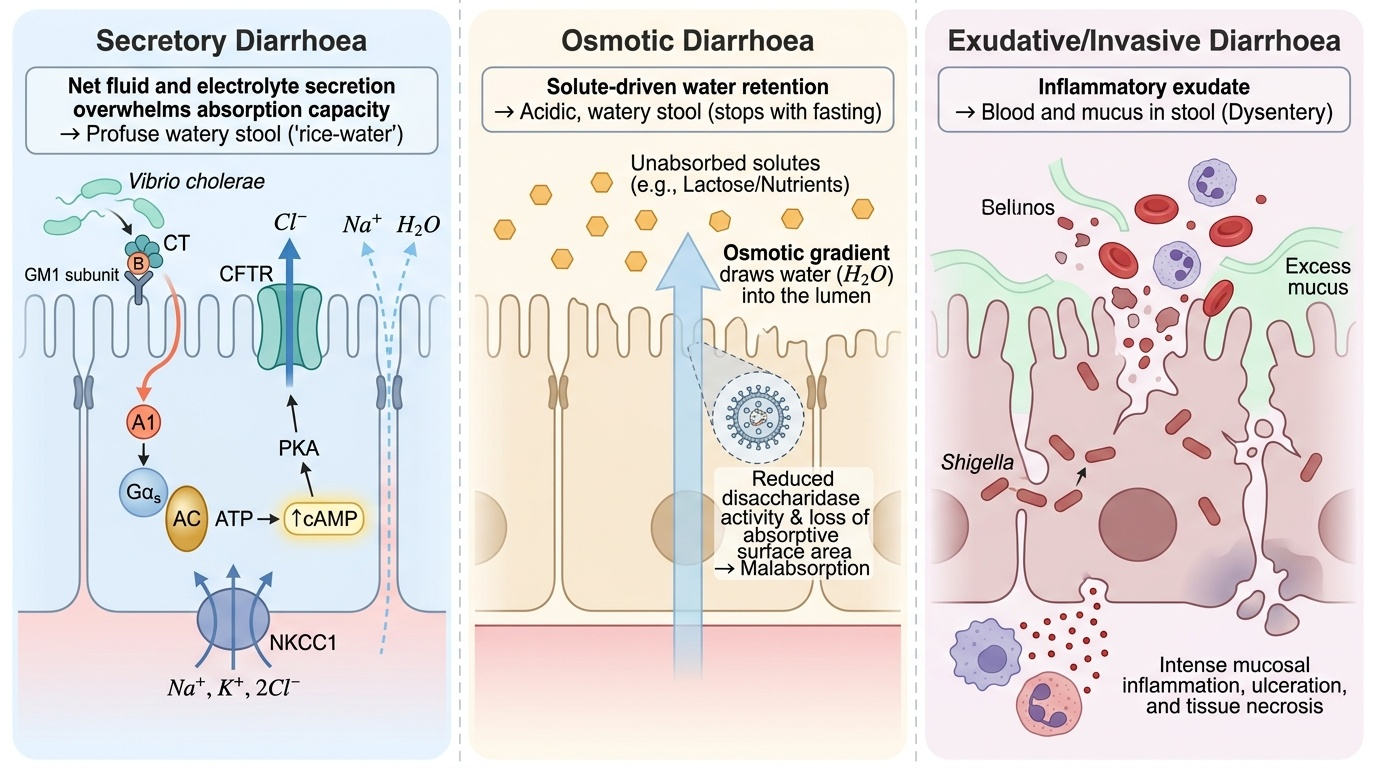
RECALL
From Year-1 Physiology, recall the mechanisms of intestinal fluid and electrolyte transport. The small intestinal epithelium has two parallel transport systems: absorptive (sodium-glucose cotransport via SGLT1, sodium-hydrogen exchange, chloride-bicarbonate exchange) and secretory (cAMP- and cGMP-activated chloride secretion via CFTR). Under normal conditions absorption exceeds secretion by several litres per day. Pathogens exploit these mechanisms: cholera toxin activates adenylate cyclase, massively raising intracellular cAMP, which locks CFTR in the open position — the gut secretes litres of isotonic fluid that overwhelms absorption, producing 'rice-water' stools. Crucially, SGLT1 (sodium-glucose cotransport) is NOT activated by cAMP and remains functional even in secretory diarrhoea — this is the entire physiological rationale for oral rehydration therapy: adding glucose to the ORS solution drives sodium (and water) absorption despite the maximal secretory stimulus.
Definitions and Clinical Features of Acute Gastroenteritis
Diarrhoea is defined by the WHO as the passage of three or more loose or watery stools in a 24-hour period. A single loose stool is not diarrhoea; neither is the normal soft frequent stool of a breastfed infant. The character of the stool matters: watery diarrhoea (no blood, no mucus) is typically caused by secretory pathogens (viruses, Vibrio cholerae, ETEC); dysentery (blood and mucus in stool) indicates an invasive bacterial pathogen (Shigella, Salmonella, Campylobacter, EIEC, Entamoeba histolytica) causing mucosal disruption, inflammation, and bleeding. This stool-character distinction is not merely academic — it directly determines whether antibiotics are indicated. Watery diarrhoea is managed with ORS, zinc, and supportive care; dysentery requires a targeted antibiotic directed at the invasive pathogen. Establishing the character of the stool is therefore the first and most important clinical question in every child with diarrhoea.
Duration-based classification — clinically essential for management and prognosis:
- Acute diarrhoea: Duration less than 14 days; most common; mostly viral; self-limiting with supportive care
- Persistent diarrhoea: Duration 14–29 days; often follows acute diarrhoea; nutritional compromise; enteric pathogen persistence or co-infection
- Chronic diarrhoea: Duration 30 days or more; structural/malabsorptive cause (coeliac disease, IBD, CF, immunodeficiency) must be sought
Clinical features of acute gastroenteritis (AGE):
- Watery diarrhoea: Profuse, offensive, no blood; vomiting prominent early; rapid dehydration; viral AGE most common under 5 years
- Dysentery: Blood and mucus in small-volume frequent stools; tenesmus (rectal straining); fever; systemic features (toxicity with Shigella)
- 'Rice-water' stools: Colourless watery stools with flecks of mucus, resembling water in which rice has been washed — the hallmark of cholera
- Complications: Dehydration (most dangerous immediate complication), electrolyte disturbances (hypo/hypernatraemia, hypokalaemia), metabolic acidosis, prerenal AKI, seizures (hyponatraemia, hypoglycaemia), haemolytic uraemic syndrome (EHEC O157:H7)
Eliciting the diarrhoea history (IMNCI framework):
The following questions must be asked for every child with diarrhoea:
1. How long has the child had diarrhoea?
2. Is there blood in the stool? (→ dysentery treatment pathway)
3. How many stools per day? Any vomiting?
4. Can the child drink/breastfeed?
5. Urine output — when was the last wet nappy/urination?
6. Any recent illness, travel, antibiotic use, or sick contacts?
7. Vaccination status (rotavirus vaccine received?)
8. Feeding practices (breast-fed vs formula vs weaning foods)
Aetiology, Risk Factors, and Pathophysiology
Acute gastroenteritis in children is caused by a wide range of pathogens. The aetiology shifts with age, season, hygiene conditions, and vaccination status. Understanding the pathogen's mechanism helps predict the stool character, complications, and whether antibiotics are indicated. In children under 5 years in India, viral pathogens — particularly rotavirus — account for 70–80% of severe acute gastroenteritis. Bacterial causes dominate the dysentery picture and are more likely in older children in endemic areas with poor water sanitation. Parasitic causes tend to be associated with persistent rather than acute diarrhoea. This section also covers the risk factors that make young children in low-resource settings particularly vulnerable, and the pathophysiological mechanisms that explain why different pathogens produce such different clinical syndromes.
Provided image
Viral causes (most common, ~70-80% of AGE in young children):
- Rotavirus: Leading cause of severe dehydrating diarrhoea in children under 5 years worldwide; faecal-oral transmission; destroys brush-border enterocytes → osmotic malabsorption + reduced disaccharidase activity → secondary lactose intolerance; now preventable by oral rotavirus vaccine (Rotavac/Rotarix — included in India's NIS)
- Norovirus: Most common cause of AGE outbreaks in older children and adults; highly contagious; self-limiting 1-3 days
- Adenovirus 40/41: Second most common viral cause under 2 years; longer duration (5-12 days)
- Astrovirus, Calicivirus: Less common; sporadic
Bacterial causes:
- Vibrio cholerae: Profuse 'rice-water' watery diarrhoea; cholera toxin activates adenylate cyclase → massive cAMP-mediated chloride/water secretion; rapid, life-threatening dehydration; faecal-oral (contaminated water); treated with ORS + single-dose doxycycline (>8 years) or azithromycin (<8 years)
- Shigella (dysentery): Invasive; destroys colonic mucosa → blood/mucus in stool; most virulent organism in paediatric diarrhoea; complications include Ekiri syndrome (fatal toxic encephalopathy), reactive arthritis, haemolytic uraemic syndrome; treat with azithromycin or ceftriaxone (cephalexin/amoxicillin resistance common)
- Salmonella (non-typhoidal): Watery or bloody diarrhoea; systemic invasion in infants; antibiotics only for systemic disease or immunocompromised
- E. coli: Five pathogenic types — ETEC (traveller's diarrhoea, secretory); EPEC (infants, persistent diarrhoea); EIEC (dysentery-like, invasive); EHEC O157:H7 (HUS — haemolytic uraemic syndrome — microangiopathic haemolytic anaemia + thrombocytopenia + AKI; antibiotics CONTRAINDICATED as they increase toxin release); EAEC (persistent)
- Campylobacter jejuni: Bloody diarrhoea; poultry-associated; self-limiting; antibiotics (azithromycin) only if prolonged or severe
- Yersinia enterocolitica: Mimics appendicitis (mesenteric lymphadenitis); rare
Parasitic causes:
- Giardia lamblia: Most common intestinal parasite causing diarrhoea; cysts in contaminated water; watery/fatty malabsorptive stools; trophozoites or cysts in stool; treated with metronidazole
- Entamoeba histolytica: Amoebic dysentery; bloody mucoid stools; extraintestinal spread (liver abscess); distinguish from non-pathogenic E. dispar by antigen testing/PCR; treat with metronidazole + diloxanide
- Cryptosporidium: Profuse watery diarrhoea, especially severe in immunocompromised (HIV)
Risk factors:
- Age <2 years (immature immunity, formula feeding, weaning-age food contamination)
- Malnutrition (impaired gut barrier, reduced secretory IgA)
- Contaminated water supply or open defecation in household
- Non-breastfed or abruptly weaned
- Lack of rotavirus vaccination
- Daycare or institutional settings (norovirus, rotavirus clusters)
- Recent antibiotic use (disrupts gut flora → C. difficile)
SELF-CHECK
An 8-month-old infant has profuse watery diarrhoea 15 times per day for 2 days during a community cholera outbreak. He is being exclusively breastfed. What is the CORRECT immediate management?
A. Nil by mouth and IV Ringer's Lactate immediately
B. Oral rehydration with reduced-osmolarity ORS and continued breastfeeding
C. Ciprofloxacin syrup and zinc sulphate only
D. Loperamide 2 mg orally to reduce stool frequency
Reveal Answer
Answer: B. Oral rehydration with reduced-osmolarity ORS and continued breastfeeding
Even in suspected cholera with profuse watery diarrhoea, oral rehydration therapy with reduced-osmolarity ORS is appropriate as long as the child can drink. The sodium-glucose cotransporter (SGLT1) remains functional despite cholera toxin's effect on CFTR, so glucose in ORS drives sodium and water absorption. ORS Plan B (75 mL/kg over 4 hours for 'some dehydration') or Plan A (home-based) applies depending on dehydration assessment. Breastfeeding should continue throughout. Loperamide is CONTRAINDICATED in children under 2 years. IV fluids (Plan C) are reserved for severe dehydration. Antibiotics (single-dose doxycycline >8 years or azithromycin <8 years) shorten duration in confirmed cholera but are not the first management step — hydration takes priority.
Assessment of Dehydration: IMNCI Framework
Dehydration assessment is the most critical clinical skill in managing acute gastroenteritis, because it determines which ORS plan to prescribe. The IMNCI framework provides a validated, reproducible system applicable in any setting — no laboratory tests required. Dehydration is classified into three categories based on specific clinical signs, each requiring a different management plan. The decision to send a child home with ORS packets (Plan A), admit to a facility for supervised rehydration (Plan B), or initiate emergency IV fluids (Plan C) rests entirely on this bedside assessment. A clinician who cannot reliably classify dehydration by clinical signs will either under-treat — risking death from shock — or over-treat with unnecessary IV fluids that are associated with their own risks (fluid overload, infection). The four IMNCI signs are specifically chosen because they can be assessed without any equipment in a primary health centre or a home visit.
Provided image
The assessment has two components: history (to estimate fluid losses and current intake) and examination (to detect clinical signs of dehydration). These must always be performed together, as neither alone is sufficient.
History elements:
- How many stools per 24 hours, and how much volume per stool (soaking the nappy vs large watery stools)?
- Any vomiting — how often? Can the child drink?
- Last urination — when? Was the nappy wet in the last 4-6 hours?
- Any tears when crying? Normal level of consciousness?
- Duration of illness
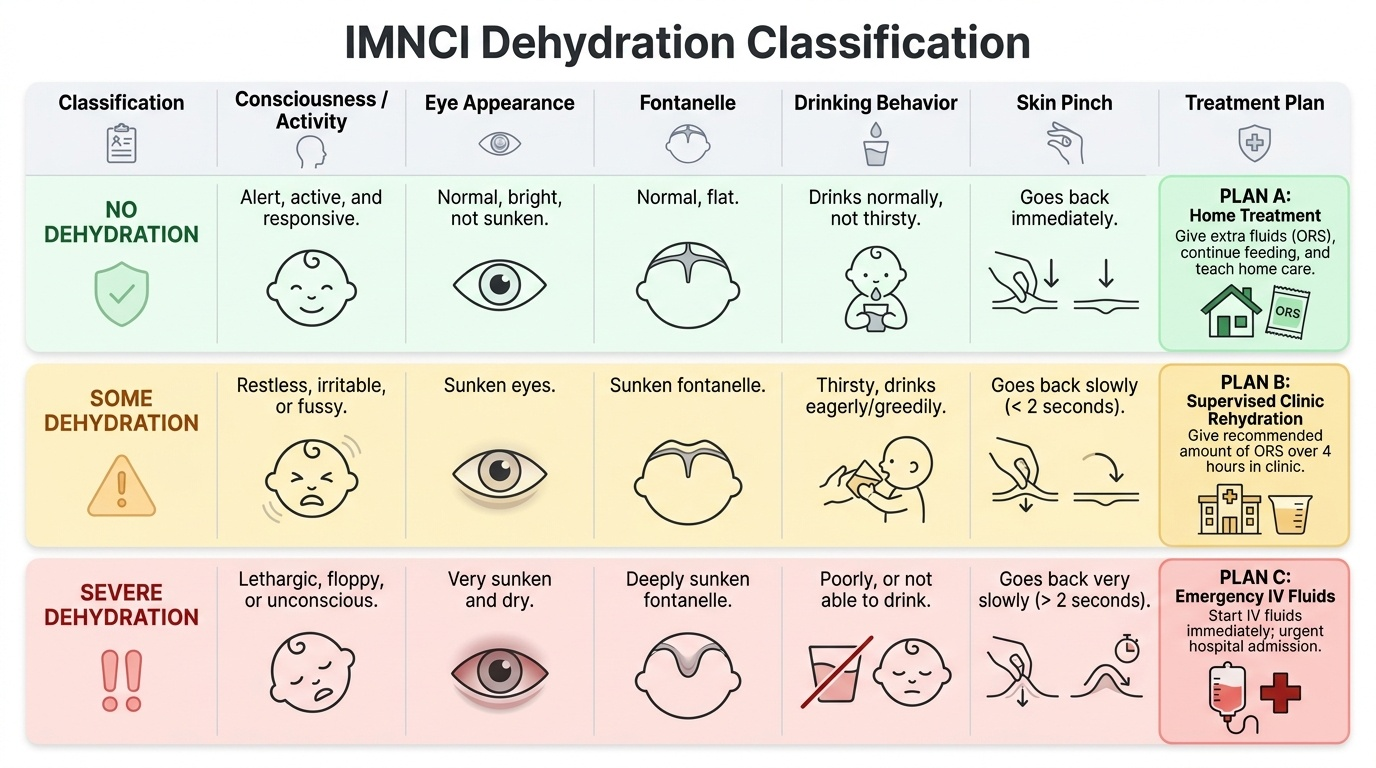
IMNCI clinical signs and classification:
Assess FOUR signs: general condition (consciousness, activity), eyes (sunken or normal), drinking (cannot drink/drinks poorly vs drinks eagerly/thirsty vs normal), skin pinch (how quickly does the skin return when pinched for 1 second?).
No dehydration: Signs normal; no two signs from either 'some' or 'severe' category. → Plan A (home ORT)
Some dehydration: Two or more of: restless or irritable; sunken eyes; drinks eagerly, thirsty; skin pinch slow (goes back in 1-2 seconds). → Plan B (supervised ORS in facility, 75 mL/kg over 4 hours)
Severe dehydration: Two or more of: lethargic or unconscious; sunken eyes; not able to drink or drinks poorly; skin pinch very slow (>2 seconds, 'tenting'). → Plan C (IV fluids immediately)
Examination technique for skin turgor (skin pinch test): Pinch the skin of the abdomen between thumb and index finger for 1 second. In a well-hydrated child, the skin returns immediately to its original position (normal turgor). In mild-to-moderate dehydration, it returns slowly over 1-2 seconds. In severe dehydration, it is very slow, forming a tent that persists >2 seconds.
Signs of complications to actively seek:
- Prerenal AKI: Oliguria/anuria, elevated serum creatinine and urea, fractional excretion of sodium <1% (pre-renal pattern); urine specific gravity >1.025
- Electrolyte disturbances: Hyponatraemia (lethargy, seizures — especially if ORS is diluted with plain water); hypernatraemia (doughy-firm skin, hyperirritability, risk with hyperosmolar home remedies); hypokalaemia (abdominal distension, ileus, weakness — severe AGE depletes potassium)
- Metabolic acidosis: Rapid deep breathing (Kussmaul's) from bicarbonate loss in severe diarrhoea
- Shock: Hypotension, tachycardia, cold extremities, prolonged capillary refill — indicates ≥10% dehydration