Page 15 of 42
PE23.5 | Dysentery — SDL Guide (Part 2)
Management: Bacillary vs Amoebic Dysentery
The management of a child with dysentery integrates three simultaneous clinical priorities: correcting the fluid deficit, targeting the causative organism with appropriate antimicrobial therapy, and maintaining nutritional status throughout the illness. These three pillars are not sequential — rehydration must be initiated immediately at presentation regardless of the organism, while the antimicrobial decision is guided by the clinical profile and the critical need to exclude EHEC before prescribing any antibiotic. Nutritional support prevents the compounding of illness-associated catabolism and protects intestinal mucosal recovery. Early identification and referral of children with HUS or severe systemic disease is equally essential — delay in recognising HUS in an EHEC-infected child can result in irreversible renal damage.
Provided image
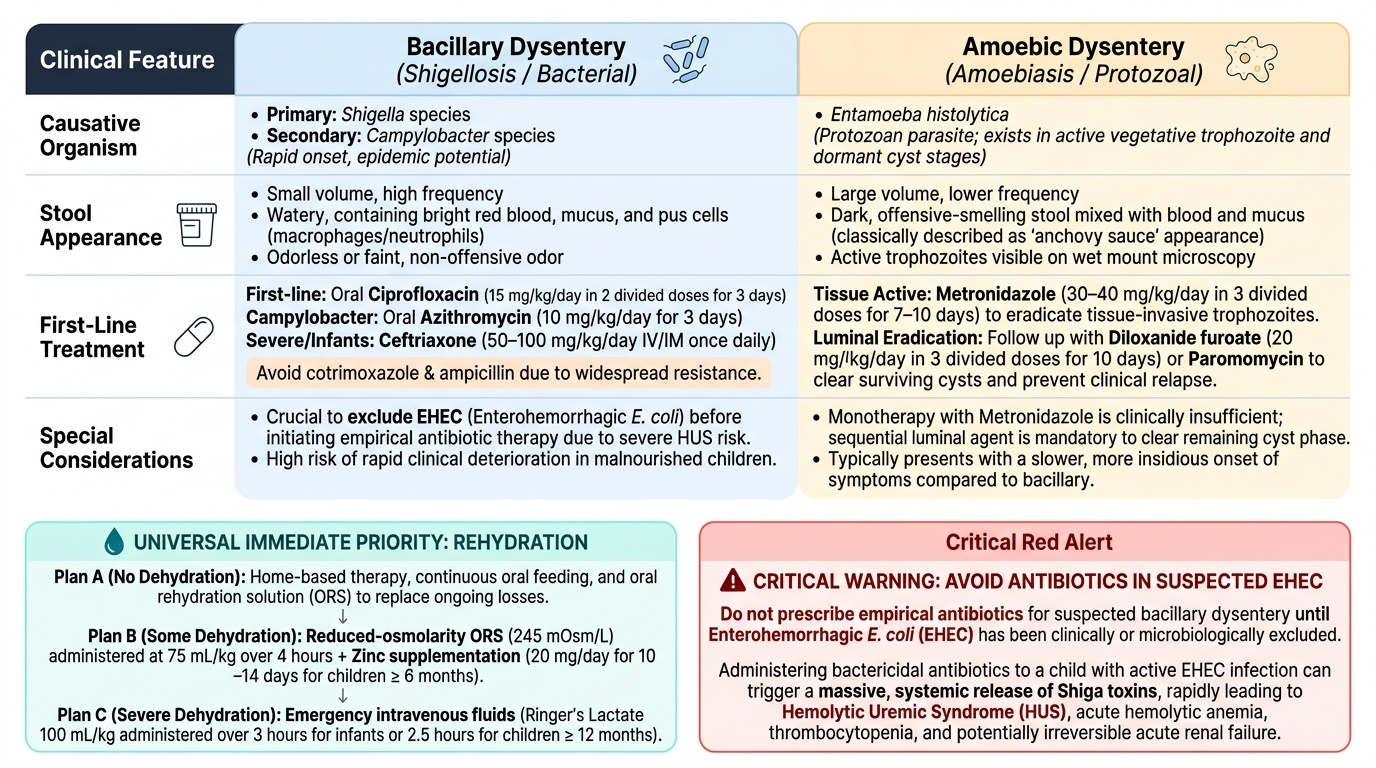
Rehydration remains the immediate priority regardless of the causative organism. Assess dehydration using IMNCI criteria and initiate the appropriate plan:
- No dehydration (Plan A): continue oral feeds, give ORS for ongoing losses.
- Some dehydration (Plan B): oral rehydration with reduced-osmolarity ORS (245 mOsm/L), 75 mL/kg over 4 hours. Zinc supplementation: 20 mg/day for 10–14 days in children ≥6 months.
- Severe dehydration (Plan C): IV Ringer's lactate 100 mL/kg over 3 hours (<12 months) or 2.5 hours (≥12 months). Reassess frequently.
Bacillary dysentery (Shigella): Ciprofloxacin is the current first-line antibiotic in India at 15 mg/kg/day in two divided doses for 3 days (oral). Ceftriaxone (50–100 mg/kg/day once daily IV/IM) is reserved for severe disease, when oral therapy is not tolerated, or in very young infants. Cotrimoxazole and ampicillin are no longer reliable due to widespread resistance. Nalidixic acid is second-line in some settings. Campylobacter dysentery: azithromycin (10 mg/kg/day for 3 days) is the drug of choice in children.
Amoebic dysentery (Entamoeba histolytica): Metronidazole (30–40 mg/kg/day in 3 divided doses for 7–10 days) is the drug of choice — it kills trophozoites in the tissue and lumen. After metronidazole, a luminal agent is added to eradicate intestinal cysts and prevent relapse: diloxanide furoate (20 mg/kg/day in 3 divided doses for 10 days) or paromomycin. Tinidazole is an alternative to metronidazole with a shorter course (50–60 mg/kg/day for 3 days in adults, adjusted for children), better tolerance, and higher tissue concentration.
EHEC (E. coli O157:H7) — critical management: ANTIBIOTICS ARE CONTRAINDICATED. Management is supportive: rehydration, careful fluid and electrolyte management, and early recognition of HUS. Blood transfusion for severe anaemia, platelet transfusion (only if active bleeding — not for prophylaxis), and renal replacement therapy (peritoneal dialysis or haemodialysis) if AKI is severe. Children with HUS should be managed in a paediatric nephrology unit.
Nutritional support: resume age-appropriate feeding as soon as the child can tolerate oral intake. Do not withhold food — prolonged fasting worsens intestinal healing and increases the risk of malnutrition. Breastfed infants should continue breastfeeding throughout.
Indications for hospitalisation: severe dehydration, inability to drink or feed, bloody diarrhoea in an infant <3 months, suspected HUS, high fever with toxic appearance, immunocompromised status, or failure to improve on outpatient therapy.
SELF-CHECK
A 5-year-old develops bloody diarrhoea without fever after eating at a picnic. On day 4 of illness his mother notes he has become pale and is urinating less. His CBC shows haemoglobin 7 g/dL with schistocytes on smear, platelets 40,000/µL, and creatinine is elevated. What is the most important management decision?
A. Start ciprofloxacin immediately to eliminate the causative organism
B. Give intravenous ceftriaxone for 7 days
C. Withhold antibiotics, provide supportive rehydration, and monitor for renal failure
D. Start metronidazole for suspected amoebic dysentery
Reveal Answer
Answer: C. Withhold antibiotics, provide supportive rehydration, and monitor for renal failure
This presentation is classic for EHEC O157:H7-associated haemolytic uraemic syndrome (HUS): afebrile bloody diarrhoea followed by the triad of microangiopathic haemolytic anaemia (schistocytes), thrombocytopaenia, and acute kidney injury. Antibiotics — especially fluoroquinolones and beta-lactams — are CONTRAINDICATED in EHEC infection because they lyse bacteria and release Shiga toxin, dramatically worsening HUS risk. Management is entirely supportive: careful fluid balance, transfusion for severe anaemia, and renal replacement therapy if needed.
Self-Assessment
The following self-assessment section consolidates the core diagnostic and management reasoning you have built across this module. Dysentery management requires integrating pathophysiology, microbiology, antibiotic stewardship, and a life-critical clinical decision about EHEC into a rapid bedside assessment. Work through the questions below before checking the answers — the ability to reason through each scenario rather than simply recall answers is the skill that matters at the bedside and in high-stakes examinations. Focus especially on the EHEC/HUS scenario, where the instinct to 'treat with an antibiotic' must be consciously overridden by mechanistic understanding of why it causes harm.
Each question below maps to a key learning objective and can be used both for independent study and as a framework for discussing dysentery cases with your supervisor or in a small-group session.
Key recall questions:
1. What is the most common cause of bloody diarrhoea in Indian children?
2. What clinical feature distinguishes EHEC-associated dysentery from Shigella dysentery, and why is this distinction life-critical?
3. Name the first-line antibiotic for Shigella dysentery in India and the reason cotrimoxazole is no longer reliable.
4. What is the drug of choice for amoebic dysentery, and which luminal agent must always follow?
5. Describe the triad of haemolytic uraemic syndrome and the management principle.
Answers: 1. Shigella dysenteriae. 2. EHEC typically presents without fever (afebrile bloody diarrhoea); giving antibiotics in EHEC triggers Shiga toxin release and precipitates HUS. 3. Ciprofloxacin 15 mg/kg/day for 3 days; widespread Shigella resistance to cotrimoxazole renders it unreliable. 4. Metronidazole (tissue amoebicide) followed by diloxanide furoate (luminal cyst eradicator). 5. Microangiopathic haemolytic anaemia + thrombocytopaenia + acute kidney injury; management is supportive — antibiotics CONTRAINDICATED.
SELF-CHECK
A 6-year-old with Shigella dysentery confirmed on stool culture cannot tolerate oral medication due to vomiting. Which antibiotic and route is appropriate?
A. Oral cotrimoxazole — it remains effective as first-line treatment
B. Intravenous ceftriaxone 50–100 mg/kg/day once daily
C. Oral metronidazole — covers both bacterial and amoebic causes
D. No antibiotic needed; dysentery is self-limiting
Reveal Answer
Answer: B. Intravenous ceftriaxone 50–100 mg/kg/day once daily
When a child with confirmed Shigella dysentery cannot tolerate oral medication, intravenous ceftriaxone (50–100 mg/kg/day, once daily) is the appropriate parenteral choice. Cotrimoxazole is no longer reliable due to widespread Shigella resistance. Metronidazole covers Entamoeba histolytica but has no role in bacillary dysentery. While some mild dysentery episodes are self-limiting, Shigella infection in children warrants antibiotic treatment to shorten illness duration and reduce complications.