Page 35 of 42
PE23.17-21 | Gastrointestinal Clinical Assessment — SDL Guide
Learning Objectives
- Elicit and document a structured GI and liver history from a child, including perinatal, family, dietary, and drug history
- Identify and interpret the significance of external markers of GI and liver disease including jaundice, spider angiomata, palmar erythema, clubbing, caput medusae, and vitamin deficiency signs
- Perform a systematic abdominal examination to detect and characterise hepatomegaly, splenomegaly, and ascites
- Interpret liver function tests (LFTs) distinguishing hepatocellular from cholestatic patterns
- Interpret hepatitis B and A/E viral serology markers correctly
- Interpret an abdominal USG report for common GI and hepatobiliary findings
- Enumerate the indications for upper gastrointestinal endoscopy in children
INSTRUCTIONS
Gastrointestinal clinical assessment skills form the practical foundation for everything you have learned about paediatric liver and gut disease. Without the ability to take a focused GI history, recognise the external markers of chronic liver disease, and correctly perform an abdominal examination, the theoretical knowledge of FHF, CLD, and portal hypertension remains stranded in the classroom. This module is explicitly skills-oriented — it focuses on how to do these assessments, what to look for, and how to interpret the results. These are core OSPE and clinical examination skills that will be tested directly in your final professional examinations.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 18 — Clinical Examination of GI System (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 380 — Clinical Manifestations of GI Disease (textbook)
- Hutchison's Clinical Methods, 24th ed. — Abdominal Examination (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the junior doctor on a paediatric ward. An 11-year-old girl is admitted with a 3-week history of progressive yellowing of her eyes, dark urine, and pale stools. Her mother mentions she is also not growing well. On general inspection you notice she has several spider-shaped reddish lesions on her upper chest, her palms look abnormally red, and her fingers are clubbed. Her abdomen is distended and her flanks are dull on percussion. Before you order a single investigation, your attending asks you: 'Tell me what you see and what you think it means.' What do you say?
WHY THIS MATTERS
GI and hepatobiliary clinical assessment skills are directly examined in OSPEs and long-case finals, and they are among the most practically important skills for a junior doctor managing a child with liver disease. The ability to distinguish hepatocellular jaundice from cholestatic jaundice by history and examination pattern, to correctly demonstrate ascites by shifting dullness, and to interpret a hepatitis B serology panel — these are not merely academic exercises. In clinical practice, they guide whether you order an urgent GI endoscopy for haematemesis, whether you screen for Wilson disease in an adolescent with unexplained liver disease, and whether you correctly communicate your examination findings to a gastroenterologist. These competencies span all five NMC domains covered in PE23.17–PE23.21.
RECALL
Before proceeding, activate your prior knowledge:
- Liver anatomy (from AN): the liver occupies the right hypochondrium and epigastrium; the right lobe is larger; the lower border is usually at or just below the right costal margin in the mid-clavicular line; it is normally not palpable in older children.
- Spleen anatomy (from AN): the spleen lies under the left 9th–11th ribs in the posterolateral thorax; the long axis runs along the 10th rib; it descends medially when enlarged; normally not palpable.
- Bilirubin fractions (from PY): conjugated (direct) bilirubin = water-soluble, excreted in urine (dark urine); unconjugated (indirect) = water-insoluble, not in urine. Conjugated hyperbilirubinaemia = cholestasis. Dark urine + pale stools = conjugated (obstructive/cholestatic) jaundice.
- Spider angiomata and palmar erythema: caused by impaired hepatic metabolism of oestrogen; >5 spider angiomata on the upper body are clinically significant in CLD.
History-Taking for GI and Liver Disease
A structured GI history in a child begins with the presenting complaint and then systematically explores the symptom cluster — jaundice, pain, vomiting, diarrhoea, bleeding, and growth — followed by contextual history (perinatal, family, dietary, drug, and travel history) that often unlocks the aetiology. The two most diagnostically powerful features from the history are the urine and stool colour (which immediately tells you whether jaundice is conjugated/cholestatic or unconjugated/haemolytic/pre-hepatic) and the chronology of onset (neonatal onset points to biliary atresia or metabolic disease; school-age onset points to Wilson disease, autoimmune hepatitis, or viral hepatitis). A history taken without these two elements is incomplete for any paediatric liver case. Always ask the parent to describe the stool colour — 'pale stools' or 'clay-coloured stools' mean acholic stools from biliary obstruction; 'normal-coloured stools with jaundice' suggest haemolytic or indirect hyperbilirubinaemia.
Systematic GI and liver history checklist:
1. Jaundice:
• Age at onset, duration, progression (improving, static, worsening)
• Urine colour: dark (conjugated = hepatocellular or cholestatic) vs normal (unconjugated = haemolytic, pre-hepatic)
• Stool colour: pale/acholic (bile flow obstruction) vs normal/dark (haemolytic)
• Pruritus (itch): prominent in cholestasis (bile salt accumulation in skin)
• Skin colour change: yellowish-green tinge = cholestasis; orange-yellow = predominantly unconjugated
2. Abdominal symptoms:
• Pain: site (RUQ = liver/gallbladder; periumbilical = small bowel; LIF = sigmoid/descending colon; generalised = peritonitis/distension), character (colicky/constant), radiation (shoulder-tip = diaphragmatic irritation), relation to meals
• Vomiting: content (bile = obstructive; blood/coffee-grounds = upper GI bleed), timing, projectile vs non-projectile
• Haematemesis: bright red (active) vs coffee-ground (older blood); clot or fresh blood
• Diarrhoea: frequency, consistency, blood (infection/IBD/intussusception), mucus, nocturnal (suggests inflammatory)
• Malaena: black, tarry, foul-smelling stools = upper GI bleeding
3. Growth and nutrition:
• Weight-for-height, MUAC (SAM threshold: MUAC <11.5 cm, weight-for-height <−3 SD)
• Failure to thrive: poor caloric intake vs malabsorption (fat-soluble vitamins in cholestasis)
• Night blindness (Vitamin A deficiency), bone deformity (Vitamin D deficiency)
4. Contextual (aetiological) history:
• Perinatal: birth weight, gestational age, jaundice in neonatal period, neonatal omphalitis or umbilical catheterisation (EHPVO risk), newborn screen results
• Family history: liver disease, consanguinity, jaundice, hepatitis B status of parents (vertical transmission), Wilson disease or metabolic liver disease in siblings
• Drug history: anticonvulsants (valproate hepatotoxicity), antibiotics, herbal medicines (hepatotoxic), paracetamol doses, traditional remedies
• Dietary: breastfed vs formula (galactosaemia), weaning history, shellfish ingestion (Hepatitis A from contaminated food), nutritional adequacy
• Travel and exposures: endemic areas for Hepatitis A/E, contact with jaundiced persons, blood transfusions, dental procedures (HBV/HCV risk)
• Immunisation: Hepatitis B vaccination status (NIS: 3 doses pentavalent at 6/10/14 wk)
External Markers of GI and Liver Disease
The general examination of a child with suspected GI or liver disease is a head-to-toe survey of external markers that reflect the systemic consequences of hepatic dysfunction. These markers are not isolated findings — they form patterns that immediately suggest the nature and chronicity of the underlying disease. A child with spider angiomata, palmar erythema, and finger clubbing has been ill for months to years; a child who has only jaundice with none of these markers is more likely to have an acute process. Learning to read the body surface as a map of hepatic function is a skill that develops with supervised clinical practice but must begin with memorising what each marker means and where to look for it. The NMC competency PE23.18 specifically names 11 markers — each must be recognised on inspection and interpreted in context.
Head-to-toe survey of external markers (PE23.18 enumeration):
- Jaundice — Inspect the sclerae first (scleral icterus appears before skin yellowing; more reliable in dark-skinned individuals); progress to skin, under the tongue (sublingual icterus). Grade: mild (sclerae only), moderate (face/trunk), severe (generalised, including palms and soles in neonates).
- Pallor — Anaemia from chronic disease, haemolysis (Wilson, hepatitis-associated aplastic anaemia), hypersplenism. Check conjunctivae, tongue, palms. In combination with jaundice, pallor suggests haemolysis (lemon-yellow = haemolytic jaundice).
- Gynaecomastia — In adolescent boys; caused by impaired hepatic degradation of oestrogen in CLD. Bilateral, often tender glandular tissue; distinguish from adipomastia in obesity.
- Spider angiomata — Dilated central arteriole with radiating capillaries (spider shape) on the upper body (face, neck, chest, upper arms). Press the centre with a glass or fingertip → it blanches completely; release → refills from the centre outward. More than 5 = clinically significant CLD.
- Palmar erythema — Erythema of the thenar and hypothenar eminences with relative pallor of the palm centre. Caused by impaired oestrogen clearance. Distinguish from physiological red palms (generalised redness in febrile illness or pregnancy).
- Ichthyosis — Dry, fish-scale-like skin; seen in chronic cholestasis (bile salt deposition) and malnutrition; also in some metabolic disorders.
- Caput medusae — Dilated tortuous veins radiating from the umbilicus. Key sign: blood flows away from the umbilicus in all directions (compare to IVC obstruction where blood flows upward in both flanks). Best seen with the child standing or at 45°.
- Clubbing — Obliteration of the angle between the nail and the nail bed (Lovibond angle >180°); drumstick appearance of fingertips. In CLD from hepatopulmonary syndrome (intrapulmonary shunts). Check all 10 fingers and toenails.
- Failure to thrive (FTT) — Wasting (low weight-for-height) and stunting (low height-for-age) in chronic liver disease from malnutrition, malabsorption, and increased metabolic demands. Plot on WHO growth chart.
- Vitamin A deficiency signs — Night blindness (ask parents: does the child stumble in dim light?); Bitot's spots (white foamy patches on conjunctivae, temporal side); corneal xerosis or ulceration in severe deficiency. Seen in prolonged cholestasis (impaired fat-soluble vitamin absorption).
- Vitamin D deficiency signs — Wrist widening (widened distal radial/ulnar metaphyses), rachitic rosary (beaded costochondral junctions), bowing of legs (genu varum), frontal bossing. Seen in biliary atresia and other cholestatic CLD.
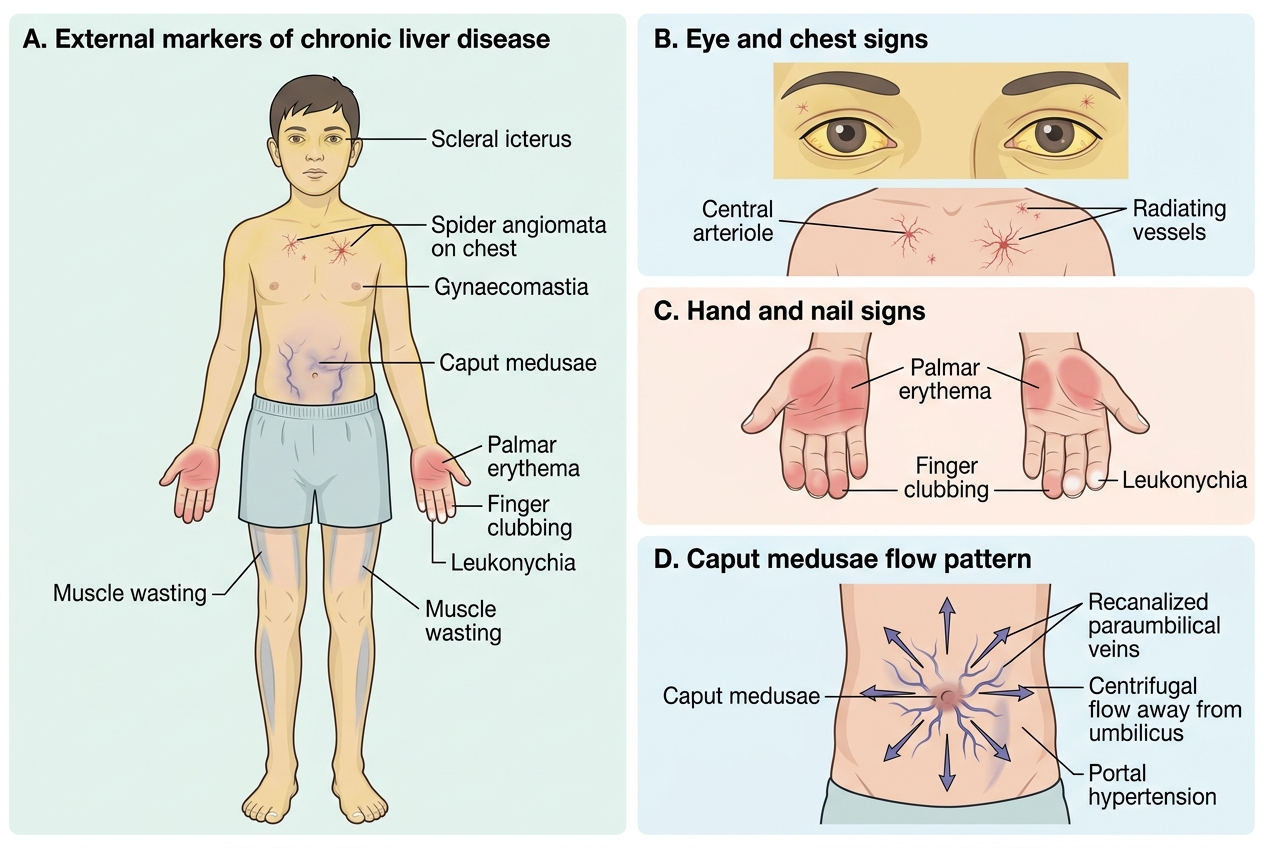
External Markers of Chronic Liver Disease in a Child
SELF-CHECK
A 13-year-old boy with chronic liver disease has dilated veins radiating from his umbilicus. His father notices the blood in the veins seems to flow downward in the lower abdomen and upward above the umbilicus. What is the CORRECT interpretation of this pattern?
A. This is IVC obstruction — blood flows upward in both flanks
B. This is caput medusae from portal hypertension — blood flows away from the umbilicus in all directions through recanalized paraumbilical veins
C. This is normal — superficial abdominal veins always follow gravity
D. This is Budd-Chiari syndrome — blood flows downward in the upper abdomen and upward in the lower
Reveal Answer
Answer: B. This is caput medusae from portal hypertension — blood flows away from the umbilicus in all directions through recanalized paraumbilical veins
Caput medusae from portal hypertension shows blood flowing AWAY from the umbilicus in all directions (centrifugal flow) through recanalized paraumbilical veins that connect the portal system to the superficial epigastric veins. In IVC obstruction, the obstruction is below the hepatic veins, so collateral flow bypasses the obstruction: blood flows upward in BOTH flanks (from below the obstruction to above). The described pattern — downward below umbilicus, upward above — is consistent with caput medusae (portal hypertension), not IVC obstruction.
Abdominal Examination: Hepatosplenomegaly and Ascites
The abdominal examination in a child with suspected liver or GI disease follows the standard sequence of inspection, percussion, and palpation, but with specific modifications for paediatric patients — the child must be positioned supine with knees flexed (to relax the abdominal wall muscles), the examiner's hands must be warm, and palpation must begin in the right iliac fossa (where the liver edge will not be before moving upward toward the costal margin). Starting palpation too high (directly under the costal margin) risks missing a massively enlarged liver whose edge has descended into the right iliac fossa. Similarly, spleen palpation begins in the right iliac fossa and moves diagonally toward the left costal margin, because a massive spleen can cross the midline. These technique points are directly examined in OSPEs and are commonly failed by students who start palpation at the 'expected' location rather than the iliac fossa.
1. Inspection:
• Shape of abdomen: scaphoid (wasted), full (normal), distended (ascites, gaseous, organomegaly)
• Umbilicus: central (normal), everted (ascites), upward displacement (massive ascites)
• Visible veins: caput medusae (portal hypertension); direction of flow
• Scars: right subcostal (Kocher's incision for liver/biliary surgery, Kasai portoenterostomy), midline, paramedian
• Visible pulsations: aortic in thin children (normal); hepatic pulsation in tricuspid regurgitation
• Visible peristalsis: in gastric outlet obstruction (epigastric waves, left to right)
2. Percussion:
• Liver span: Percuss in the right midclavicular line from above lung resonance downward to find upper border of liver dullness (normally 5th intercostal space), then from below (iliac fossa) upward to find lower border (costal margin level). Liver span = distance between the two borders; normal 5–10 cm in school-age children.
• Splenic dullness: Percuss Traube's space (triangular area bounded by left 6th rib superiorly, left anterior axillary line laterally, left costal margin inferiorly) — normally tympanic; dullness suggests splenomegaly.
• Ascites detection (shifting dullness): Percuss from the umbilicus laterally toward the flank — the transition from tympanic (central) to dull (lateral) marks the fluid level. Ask the patient to roll toward the opposite side (lateral decubitus) and wait 30 seconds → if the dull area shifts toward the dependent flank, ascites is present (shifting dullness = positive). Fluid thrill: detected only with large ascites; flick one flank with a finger while placing the other hand firmly on the opposite flank (helper places edge of hand on midline to prevent transmission through fat).
3. Palpation:
• Liver palpation: Begin in the right iliac fossa with the flat of the right hand, pressing gently inward and upward at 45°; ask the child to breathe deeply — feel for the liver edge descending with inspiration. Move progressively upward in 2 cm steps. Record the liver edge in cm below the right costal margin in the midclavicular line. Characterise: smooth or nodular (cirrhosis = nodular), tender or non-tender, hard or soft, pulsatile (tricuspid regurgitation).
• Spleen palpation: Begin in the right iliac fossa (to detect massive splenomegaly that has crossed the midline), move diagonally toward the left costal margin. Record size in cm below the left costal margin in the left midclavicular line. The spleen has a medial notch palpable on its upper border in large spleens — this helps distinguish from the left kidney.
• Normal findings: Liver palpable up to 2 cm below the right costal margin in children under 3 years (normal); spleen not normally palpable at any age.
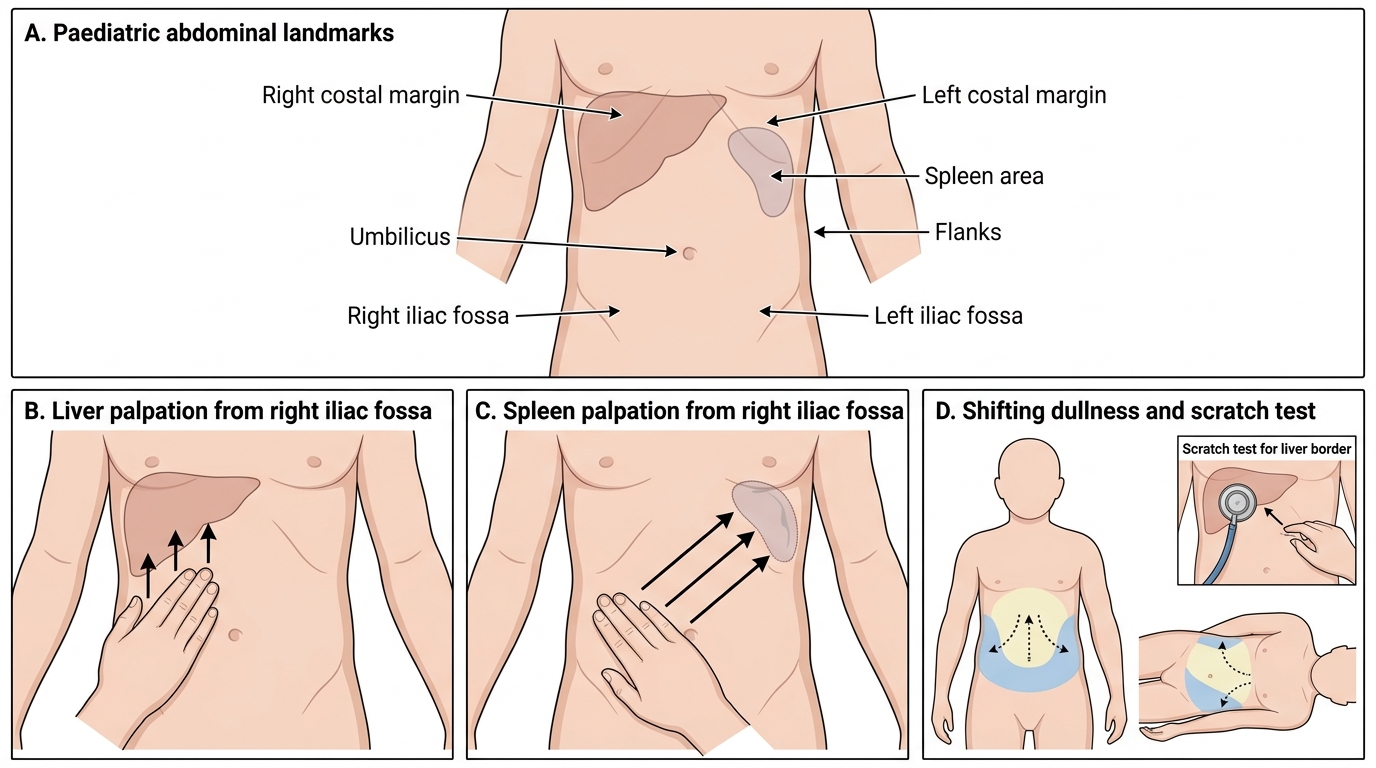
Paediatric Abdominal Examination: Liver, Spleen and Ascites
CLINICAL PEARL
The 'scratch test' for liver border — useful in gaseous abdomen: In a child with a lot of intestinal gas, percussion may give inconsistent results for the liver border. The scratch test: place the stethoscope diaphragm over the liver area and scratch the skin with a fingernail, moving from the epigastrium toward the right flank. The scratching sound is louder when transmitted through solid liver, and suddenly quieter when you reach the liver edge (or the gas-filled colon). This gives a reliable liver border assessment when standard percussion is difficult. It is a simple bedside technique that every paediatrician should master for difficult abdominal examinations.