Page 1 of 42
PE23.1 | Vomiting — SDL Guide
Learning Objectives
- Define vomiting and distinguish it from regurgitation and rumination
- Classify causes of vomiting in children by age group and mechanism
- Recognise bilious vomiting as a surgical emergency requiring immediate action
- Describe the diagnostic approach including key investigations such as ultrasound for hypertrophic pyloric stenosis
- Outline age-appropriate management of common causes of vomiting in children
INSTRUCTIONS
Vomiting is one of the most common presentations in paediatric practice, yet it can range from the completely benign — such as the daily regurgitation of a thriving infant — to a life-threatening surgical emergency. The clinician's first task is to identify which end of that spectrum a given child occupies. Bilious vomiting is green, and green means go — straight to the surgeon. Getting this distinction right at the bedside is the essential skill this module builds.
References
- Ghai Essential Pediatrics, 9th edition, Ch 16 (Gastrointestinal system) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 366 (Vomiting) (textbook)
- IAP Guidelines on Management of Vomiting in Children (guidelines)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-week-old male infant is brought by his anxious mother who reports that he vomits 'with great force' after every feed over the past week. The vomiting is non-bilious, milk-coloured, and shoots out nearly a metre. He is eager to feed again immediately after vomiting. On examination he is underweight for age, mildly dehydrated, and you notice visible gastric peristalsis moving left to right in the epigastrium. An olive-shaped mass is palpable in the right hypochondrium during feeding.
Contrast this with a second scenario: a 3-day-old neonate brought from the postnatal ward with a single episode of green vomiting and a mildly distended abdomen. The nurse says the baby has not yet passed meconium.
Both babies vomit. One needs a surgeon immediately; the other can wait for a clean ultrasound. Can you tell which is which — and why?
WHY THIS MATTERS
Vomiting accounts for a substantial proportion of paediatric emergency consultations and hospital admissions in India. While the majority of cases are caused by gastroenteritis or physiological gastro-oesophageal reflux, a failure to recognise bilious vomiting or other red-flag presentations can result in catastrophic outcomes — midgut volvulus secondary to malrotation has a mortality of nearly 100% if not decompressed within hours. Beyond the surgical emergency, understanding the spectrum of causes by age allows the clinician to rationalise investigation, avoid unnecessary imaging, and counsel parents appropriately. The management of common causes — ORS for associated dehydration, position changes for GERD, and timely surgery for pyloric stenosis — directly impacts morbidity and nutrition in early infancy.
RECALL
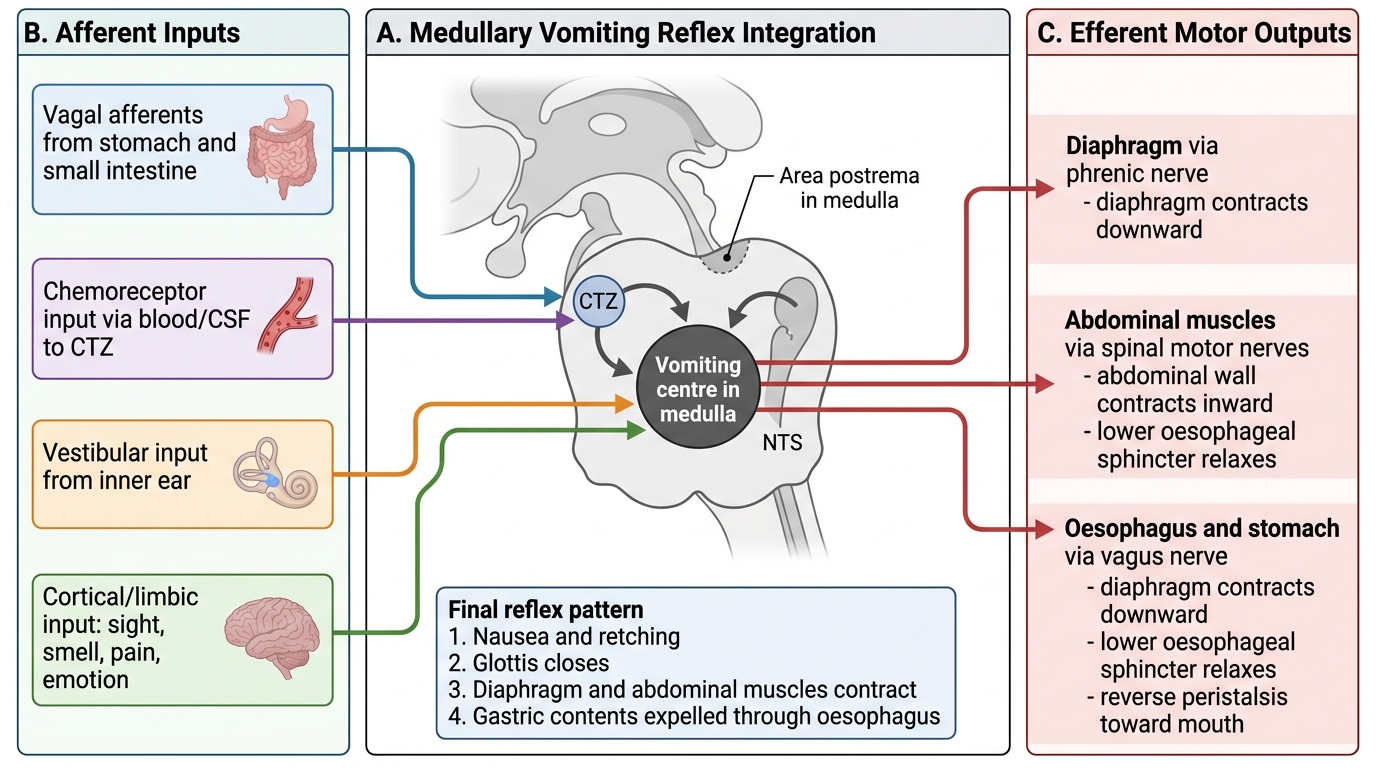
Before proceeding, recall the physiology of the vomiting reflex from your Year-1 Physiology course. The vomiting centre (VC) lies in the medullary reticular formation and receives inputs from several sources: the chemoreceptor trigger zone (CTZ) in the area postrema (outside the blood-brain barrier, sensitive to drugs and toxins), the vestibular system (motion sickness), the nucleus tractus solitarius (visceral afferents via the vagus nerve), and higher cortical centres (emotion, anticipatory vomiting). The efferent arm of the reflex coordinates diaphragm, abdominal wall, and oesophageal/cardiac sphincter relaxation to expel gastric contents. Recall also the anatomy of the pylorus (the muscular junction of stomach and duodenum) and the ligament of Treitz (duodenojejunal flexure, the landmark for bilious vs non-bilious contents). Bile enters the duodenum BEYOND the pylorus and below the ligament of Treitz — vomitus containing bile therefore implies an obstruction at or below the duodenum.
Clinical Presentation and Classification of Vomiting
Vomiting is the forceful expulsion of gastric or intestinal contents through the mouth, coordinated by the vomiting centre and involving active contraction of abdominal muscles. It must be distinguished from regurgitation (effortless passive return of gastric contents, without nausea or effort — typical of physiological GERD in infancy) and rumination (voluntary re-chewing and re-swallowing of food, a behavioural pattern seen in older children and adolescents). This distinction matters because regurgitation is benign and self-resolving in most infants, while vomiting always warrants a cause.
Provided image
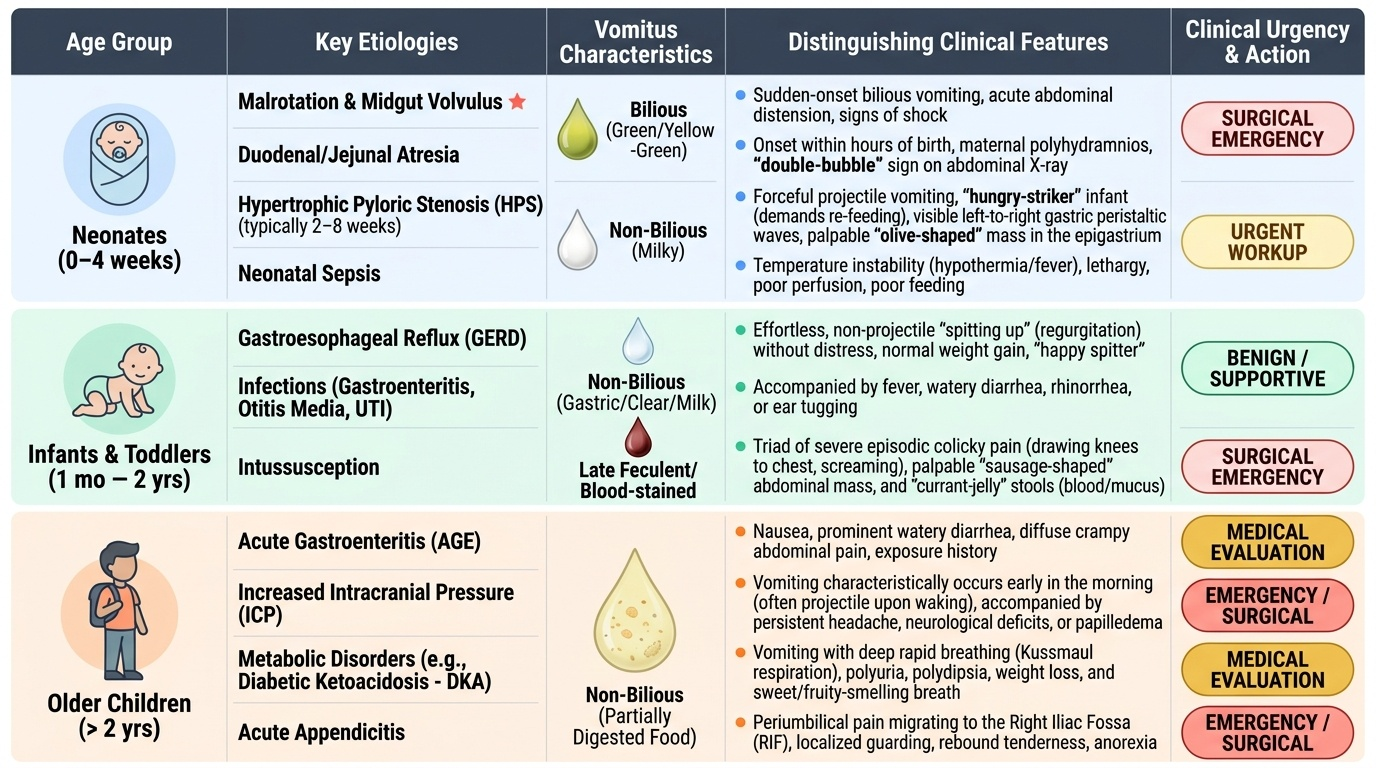
The clinical approach to vomiting in children is fundamentally age-stratified, because the causes change dramatically with developmental stage — a differential diagnosis that encompasses malrotation in the neonate, hypertrophic pyloric stenosis in the young infant, intussusception in the toddler, and appendicitis or increased intracranial pressure in the older child. The history must therefore always begin with the child's age, before any other feature is interpreted. The single most important historical feature is the colour of the vomitus, which can immediately tell you whether you are dealing with a surgical emergency:
- Bilious (green or yellow-green) vomiting indicates that intestinal contents beyond the ligament of Treitz are being expelled. This is a surgical emergency until proven otherwise. The default diagnosis is malrotation with midgut volvulus — a twisting of the intestines around the superior mesenteric artery that can progress to total intestinal infarction within hours. Other causes of bilious vomiting include duodenal/jejunal atresia (neonates), adhesional obstruction, and Hirschsprung's disease with enterocolitis.
- Projectile non-bilious vomiting in an infant aged 2–8 weeks strongly suggests hypertrophic pyloric stenosis (HPS) — hypertrophy of the pyloric muscle causing gastric outlet obstruction. The vomitus contains only gastric contents (milk-coloured, never bile), the infant is hungry immediately after, and visible gastric peristalsis (waves moving left to right across the epigastrium) may be observed.
- Non-projectile, non-bilious vomiting is the most common pattern and encompasses the vast majority of causes from infection to GERD to metabolic disorders.
Additional clinical features that guide assessment:
- Timing relative to feeds: immediately after feeds (GERD, HPS); hours after (obstruction, gastroenteritis)
- Blood in vomitus (haematemesis): bright red (oesophageal, Mallory-Weiss, stress ulcer) vs coffee-ground (gastric bleeding)
- Associated fever: gastroenteritis, sepsis, meningitis, urinary tract infection
- Headache, altered consciousness, bulging fontanelle: raised intracranial pressure (meningitis, encephalitis, hydrocephalus, intracranial bleed)
- Abdominal distension: obstruction, Hirschsprung's enterocolitis
Pathophysiology and Aetiology
The pathophysiology of vomiting involves activation of the vomiting centre by one or more afferent inputs. Understanding which input is dominant for each cause helps explain the clinical presentation and guides treatment.
Central pathway (CTZ-mediated): Drugs (opioids, chemotherapy, digoxin), metabolic disturbances (uraemia, hyperammonaemia, diabetic ketoacidosis, congenital adrenal hyperplasia), and toxins activate dopamine D2 and 5-HT3 receptors in the CTZ. This is why ondansetron (5-HT3 antagonist) is effective for chemotherapy-induced vomiting and why vomiting accompanies many systemic illnesses.
Peripheral/vagal pathway (visceral afferents): Distension, inflammation, or obstruction of the gastrointestinal tract activates mechanoreceptors and chemoreceptors in the gut wall, relayed via the vagus nerve to the nucleus tractus solitarius. This mechanism underlies vomiting in gastroenteritis, obstruction, and peritonitis.
Vestibular pathway: Motion sickness and labyrinthitis activate histamine H1 and muscarinic M1 receptors — relevant for cyclical vomiting syndrome and motion sickness in children.
Age-based aetiology:
Neonates (0–4 weeks):
- Surgical: Malrotation ± volvulus (bilious vomiting, surgical emergency); oesophageal/duodenal/jejunal/ileal atresia; Hirschsprung's disease (delayed passage of meconium >48 h after birth, rectal biopsy shows aganglionosis of myenteric plexus); anorectal malformations; imperforate anus
- Medical: Physiological regurgitation; sepsis/meningitis; congenital adrenal hyperplasia (salt-wasting crisis, bilious vomiting, ambiguous genitalia in females); inborn errors of metabolism
Infants (1–12 months):
- Hypertrophic pyloric stenosis (HPS): Most common surgical cause in this age group; peak incidence 3–6 weeks; male predominance 4:1; pyloric muscle hypertrophy → progressive gastric outlet obstruction → metabolic alkalosis (loss of HCl) with hypokalaemia and hypochloraemia
- GERD/physiological regurgitation: Most common cause overall; self-limiting in the majority
- Intussusception: Peak 6–18 months; ileocolic most common; presents with paroxysmal crying, bloody ('currant-jelly') stool, sausage-shaped abdominal mass — vomiting is a prominent early feature
- Infections: Gastroenteritis (rotavirus most common in unvaccinated), urinary tract infection, otitis media (reflex vomiting)
Toddlers and older children (1–12 years):
- Gastroenteritis: Most common cause; rotavirus, norovirus, adenovirus, Salmonella, E. coli
- Raised intracranial pressure: Morning vomiting, headache, papilloedema — must not be missed; causes include meningitis, encephalitis, cerebral tumours, hydrocephalus, subdural haematoma
- Surgical acute abdomen: Appendicitis (periumbilical → right iliac fossa pain, fever, guarding); intussusception (still seen up to 5 years)
- Metabolic/systemic: Diabetic ketoacidosis, Addison's disease, uraemia
- Cyclical vomiting syndrome (CVS): Recurrent stereotyped episodes with symptom-free intervals; associated with migraine family history; autonomic features
- Psychogenic/functional: School-related, functional dyspepsia, bulimia in adolescents
Neural Pathways of the Vomiting Reflex
SELF-CHECK
A 5-week-old male infant presents with 1-week history of projectile vomiting after every feed. The vomitus is milk-coloured and non-bilious. He appears hungry after vomiting. Examination reveals mild dehydration and a palpable olive-shaped mass in the right hypochondrium. Which investigation will confirm the diagnosis?
A. Barium meal showing 'string sign'
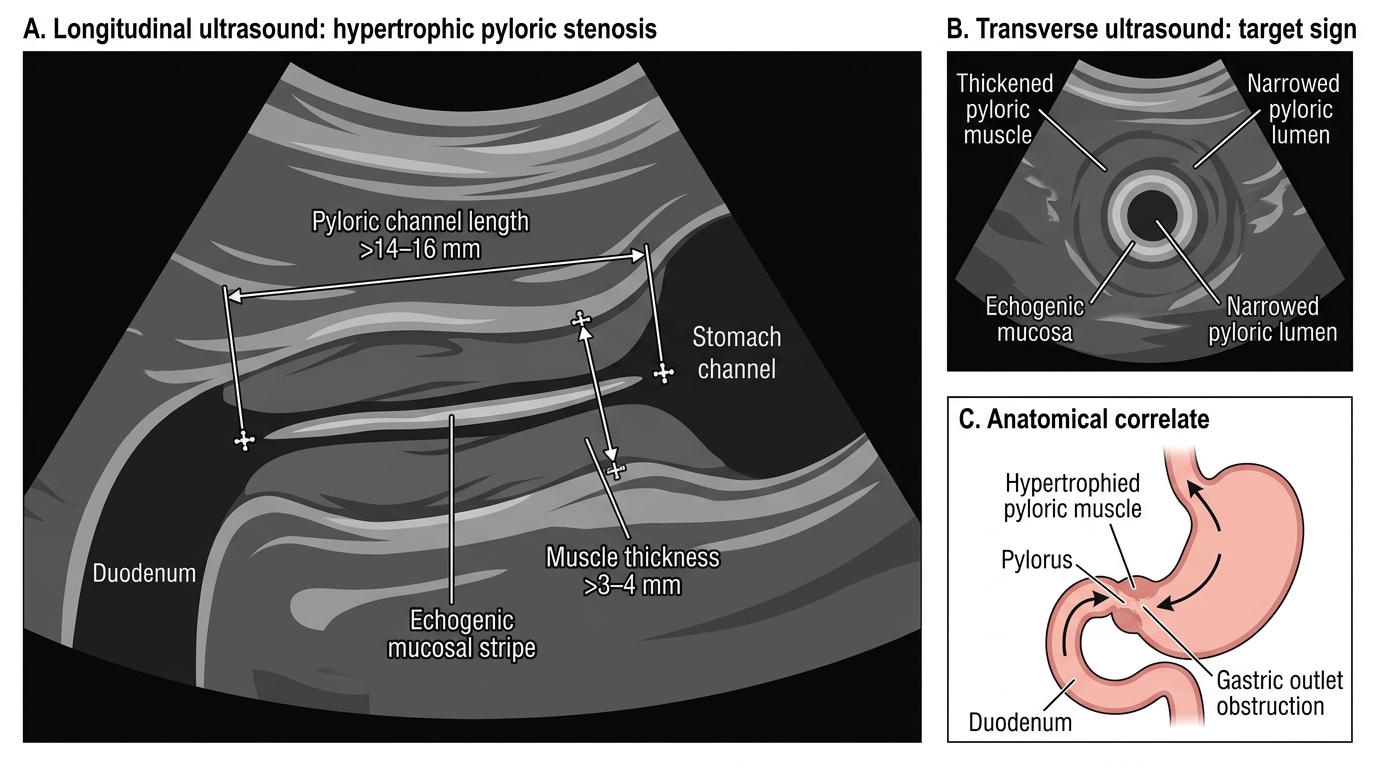
B. Ultrasound of abdomen showing pyloric muscle thickness >3-4 mm and channel length >14-16 mm
C. Plain X-ray abdomen erect showing air-fluid levels
D. Upper GI endoscopy
Reveal Answer
Answer: B. Ultrasound of abdomen showing pyloric muscle thickness >3-4 mm and channel length >14-16 mm
Ultrasound is the investigation of choice for hypertrophic pyloric stenosis (HPS). The diagnostic criteria are pyloric muscle wall thickness >3-4 mm and pyloric channel length >14-16 mm. The clinical picture of a 3-6 week old male with projectile non-bilious vomiting, hunger after vomiting, visible peristalsis, and palpable olive mass is classic. The 'string sign' on barium meal (outlining the elongated channel) is confirmatory but barium studies are now rarely done — ultrasound is non-invasive, quick, and highly accurate (sensitivity >95%).
Evaluation and Investigations
A structured clinical evaluation begins with a thorough history and examination before ordering any investigation. History should specifically ascertain the colour and character of vomiting, its onset and duration, relationship to feeding, associated symptoms (fever, diarrhoea, headache, rash, jaundice, weight loss), and the infant's overall feed intake and urine output (indicators of dehydration severity). The history of colour alone can triage the child to the surgical or medical pathway — green or yellow-green vomiting mandates immediate surgical consultation before any further evaluation. For non-bilious vomiting, the age of the child, the projectile nature, and the associated features then guide the differential. Always establish hydration status early, as dehydration assessment determines the urgency and route of rehydration.
Key clinical examination findings:
- Hydration status: Assess skin turgor (tenting), capillary refill time, fontanelle fullness (sunken = dehydrated), mucous membranes, eye recession, and urine output. Use the IMNCI dehydration classification: no dehydration, some dehydration, or severe dehydration.
- Abdomen: Visible peristalsis (HPS or high obstruction); distension (lower obstruction, Hirschsprung's); tenderness and guarding (appendicitis, peritonitis); a sausage-shaped mass in right iliac fossa moving towards the umbilicus (intussusception); olive-shaped firm mass in right hypochondrium during a quiet feed (HPS — feeds with one hand, palpates with the other)
- Neurological: Bulging fontanelle, neck stiffness, altered consciousness, papilloedema (raised ICP)
- General: Jaundice (hepatitis, biliary atresia), ambiguous genitalia (CAH), ill-looking child with purpuric rash (meningococcaemia)
Investigations (targeted, not shotgun):
For suspected surgical emergencies:
- Ultrasound abdomen: First-line for HPS (pyloric muscle thickness and channel length), intussusception (target sign = concentric circles on transverse USG), and malrotation (abnormal position of superior mesenteric artery/vein)
- Plain X-ray abdomen (erect + supine): Double-bubble sign (duodenal atresia); absence of gas beyond the proximal small bowel (high obstruction); multiple air-fluid levels (lower obstruction). This is the first imaging in a neonate with bilious vomiting.
- Upper GI contrast study (UGIS): Gold standard for malrotation — shows the duodenojejunal flexure (ligament of Treitz) in an abnormal position. Used when USG is inconclusive.
For medical/metabolic causes:
- Serum electrolytes: HPS → metabolic alkalosis (pH ↑, bicarbonate ↑), hypokalaemia (K⁺ ↓), hypochloraemia (Cl⁻ ↓). Urine paradoxically acidic (paradoxical aciduria) despite alkalosis — a classic finding.
- Blood glucose, urea, creatinine, ammonia: Metabolic causes, uraemia
- Urine routine and culture: UTI causing reflex vomiting
- CSF analysis: Meningitis
- Blood culture: Sepsis
Ultrasound Diagnosis of Hypertrophic Pyloric Stenosis
| Investigation | When to order | Key finding |
|---|---|---|
| Ultrasound abdomen | Suspected HPS, intussusception, malrotation | Pyloric muscle >3-4mm/channel >14-16mm; target sign; SMA-SMV inversion |
| Plain X-ray abdomen | Bilious vomiting in neonate | Double-bubble, absent gas, air-fluid levels |
| Serum electrolytes | Persistent vomiting, dehydration | Metabolic alkalosis + hypokalaemia + hypochloraemia in HPS |
| Upper GI contrast | Suspected malrotation (if USG inconclusive) | Abnormal DJ flexure position |
| Blood glucose | Ill neonate or altered consciousness | Hypoglycaemia as cause or consequence |
| CSF | Fever + vomiting + neurological signs | Cells, protein, glucose for meningitis |
CLINICAL PEARL
Bilious vomiting is a surgical emergency until proven otherwise. Any green or yellow-green vomiting in an infant or child must be evaluated urgently for intestinal obstruction — particularly malrotation with midgut volvulus. Do not wait for multiple episodes or reassure parents that it will resolve. The window to save viable bowel in volvulus is hours, not days. Similarly, a neonate who has NOT passed meconium by 48 hours of life AND is vomiting should be evaluated for Hirschsprung's disease — a rectal biopsy demonstrating aganglionosis of the submucosal and myenteric plexuses is diagnostic. Contrast enema may show a transition zone (narrow aganglionic segment to dilated proximal colon).