Page 1 of 31
PE24.{1,21} | Cardiorespiratory Arrest — SDL Guide
Learning Objectives
- Describe the aetio-pathogenesis and clinical recognition of cardiorespiratory arrest in children
- Explain the anatomical and physiological basis of paediatric basic life support (BLS)
- Demonstrate the correct sequence, compression technique, compression-to-ventilation ratio, and depth of paediatric BLS
- Distinguish shockable (VF/pVT) from non-shockable (asystole/PEA) rhythms and describe rhythm-directed advanced life support
- Outline the principles of post-resuscitation care after return of spontaneous circulation (ROSC)
- Perform BLS on a paediatric manikin using the correct PALS C-A-B sequence
INSTRUCTIONS
Cardiorespiratory arrest in a child is among the most time-critical emergencies in clinical medicine. Unlike adults, where cardiac arrest is most often primary (arrhythmic), paediatric arrests are predominantly secondary to progressive respiratory failure or shock — making early recognition and airway management pivotal. A final-year student who witnesses a paediatric arrest must be able to initiate BLS immediately, perform effective chest compressions, provide mask ventilation, and call for help in a structured manner. This module equips you with the knowledge and simulated skill to respond to cardiorespiratory arrest in a child or infant.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 27 — Paediatric Emergencies (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 78 — Resuscitation and Stabilisation (textbook)
- AHA PALS Guidelines 2020 — Paediatric Basic and Advanced Life Support (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are on a paediatric ward when a nurse calls urgently: a 3-year-old who was admitted for pneumonia has become unresponsive. You rush to the bedside. The child is limp, pale, and not breathing. You check for a pulse at the brachial artery — absent. The monitor shows a flat line. You are the first responder. What do you do in the next 60 seconds?
WHY THIS MATTERS
Paediatric cardiorespiratory arrest is rare compared to adult arrest, but survival is critically dependent on the quality of the first response in the first few minutes. In India, where dedicated paediatric emergency teams may not be immediately available at every facility, any trained final-year student or intern may be the first provider at the bedside. High-quality BLS — correct compression depth, rate, and ventilation — buys time until advanced support arrives. Understanding the paediatric PALS algorithm also prepares you for the MBBS examination, postgraduate entrance tests, and your clinical internship in paediatric wards, emergency rooms, and district hospitals.
RECALL
Before proceeding, recall the following from your earlier years:
• Cardiac output = heart rate × stroke volume; in children, cardiac output is rate-dependent (fixed stroke volume) — bradycardia rapidly reduces output.
• Respiratory mechanics: tidal volume, lung compliance, resistance; children have smaller functional residual capacity and higher oxygen consumption per kg, making them desaturate faster.
• Oxygen-haemoglobin dissociation curve: the steep part of the curve means a small fall in PaO₂ causes a large drop in saturation in a compromised child.
• Vasovagal and baroreceptor reflexes: bradycardia in a child often signals severe hypoxia (not primary arrhythmia), which is the fundamental reason paediatric resuscitation prioritises airway and breathing.
Clinical Indication: Recognising Cardiorespiratory Arrest in a Child
Cardiorespiratory arrest is defined as the cessation of effective respiratory effort and effective cardiac output, resulting in absent delivery of oxygenated blood to vital organs. In the clinical setting, arrest is recognised by the triad of unresponsiveness (no response to voice or touch), absence of normal breathing (apnoea or only agonal gasps), and absence of a palpable central pulse for ≥10 seconds. Unlike adults, where sudden cardiac arrest most often reflects a primary arrhythmic event (typically ventricular fibrillation), paediatric arrests are predominantly secondary — occurring as the end-point of progressive respiratory failure or circulatory shock. This is why the peri-arrest state (impending arrest) is often detectable and therefore preventable with prompt intervention.
Provided image
Aetiologically, the commonest precursors to paediatric cardiorespiratory arrest include: severe respiratory conditions (pneumonia, bronchiolitis, croup, asthma, foreign-body aspiration), circulatory shock (septic, hypovolaemic, cardiogenic), near-drowning, trauma, severe metabolic derangements (hypoglycaemia, electrolyte disturbances), and toxin ingestion. Respiratory arrest precedes cardiac arrest in most paediatric cases by several minutes, during which the child is hypoxic but the heart is still perfusing — this is the critical window for intervention. Primary ventricular fibrillation and primary cardiac arrest are less common in children but do occur in congenital heart disease and commotio cordis (chest trauma).
Clinical recognition is structured around a rapid primary assessment:
• Responsiveness: tap shoulders firmly and call the child's name
• Breathing: look, listen, and feel for ≤10 seconds — note agonal breathing (occasional, gasping, irregular) is NOT effective breathing
• Pulse check: brachial artery in infants (<1 year), carotid or femoral in children; check for ≤10 seconds; if absent or heart rate <60/min with signs of poor perfusion in an infant, initiate CPR
• Colour and tone: mottled, cyanosed, or ashen skin with generalised hypotonia are ominous signs
Anatomy and Physiology Relevant to Paediatric Resuscitation
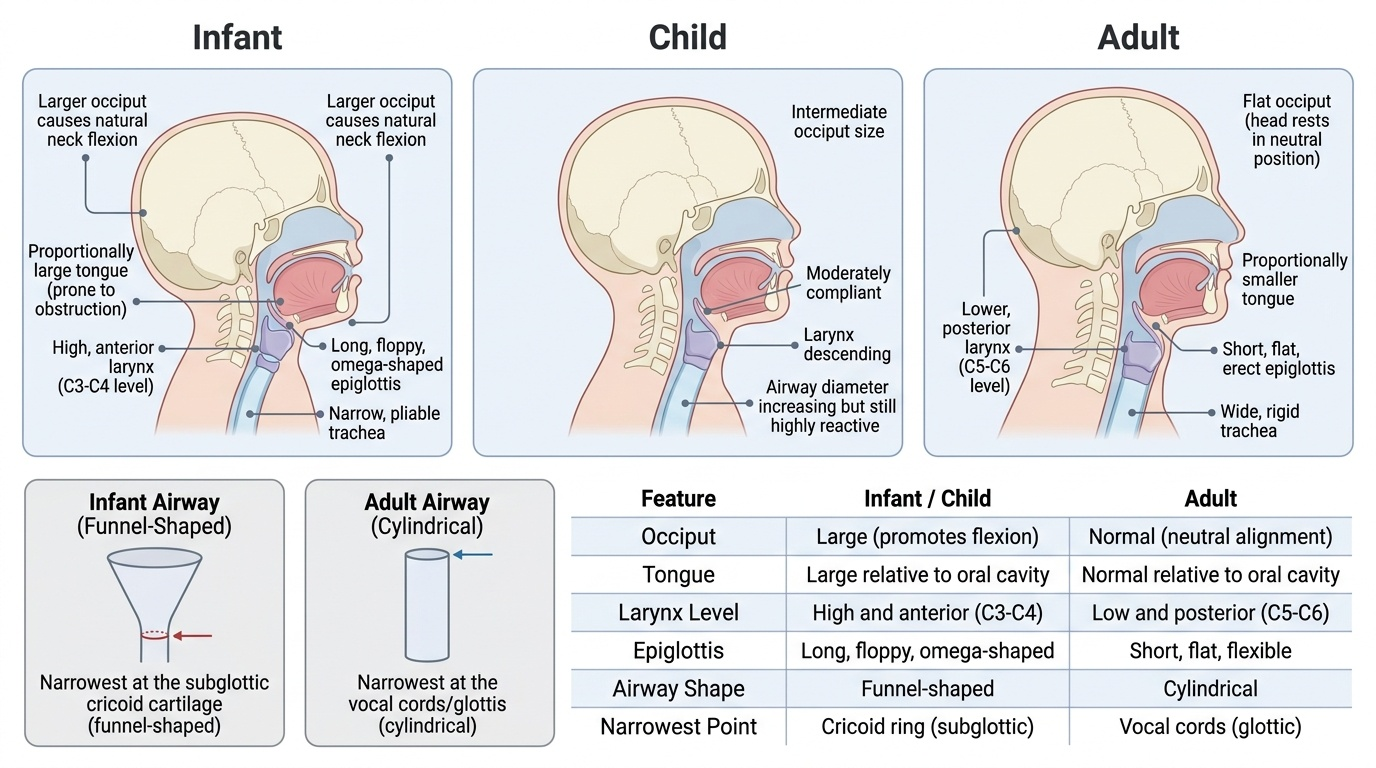
The paediatric airway differs from the adult airway in several critical ways that directly shape resuscitation technique. In infants, the occiput is proportionally large, causing passive neck flexion when the child is supine — this naturally obstructs the airway and requires a 'sniffing' or neutral position to open it (not hyperextension as in adults). The tongue is proportionally larger relative to the oral cavity, making it the most common cause of upper airway obstruction in an unconscious child. The larynx is located more anteriorly and superiorly (at C3-4 in infants vs C4-5 in adults) and the epiglottis is floppy and omega-shaped, both of which increase the difficulty of direct laryngoscopy. The subglottis is the narrowest part of the airway in children (vs the glottis in adults) and is functionally 'funnel-shaped', which is why even a small amount of mucosal oedema (croup, post-extubation) causes dramatic obstruction.
The physiological rationale for the airway-first approach in children is rooted in their higher metabolic rate and oxygen consumption per kilogram body weight. Children consume approximately 6–8 mL O₂/kg/min compared to 3–4 mL/kg/min in adults, meaning their oxygen reserves deplete far faster during apnoea. The functional residual capacity is proportionally lower, and the closing capacity may exceed FRC during tidal breathing in infants — leading to early airway closure and V/Q mismatch. This physiology explains why a child can progress from respiratory distress to respiratory failure to cardiac arrest within minutes, and why restoration of oxygenation and ventilation (not just cardiac rhythm) is the cornerstone of paediatric resuscitation.
Cardiac physiology relevant to CPR: the myocardium is relatively non-compliant in infants, and cardiac output is primarily rate-dependent (stroke volume is less variable). Effective chest compressions must restore adequate coronary and cerebral perfusion pressure — determined by compression depth, rate, and minimising interruptions. The thorax in children is more compliant and elastic than in adults, enabling effective compressions with a single hand or even two fingers in infants, but requiring one-third anteroposterior (AP) depth to generate sufficient intrathoracic pressure.
BLS for Children: Technique and Sequence
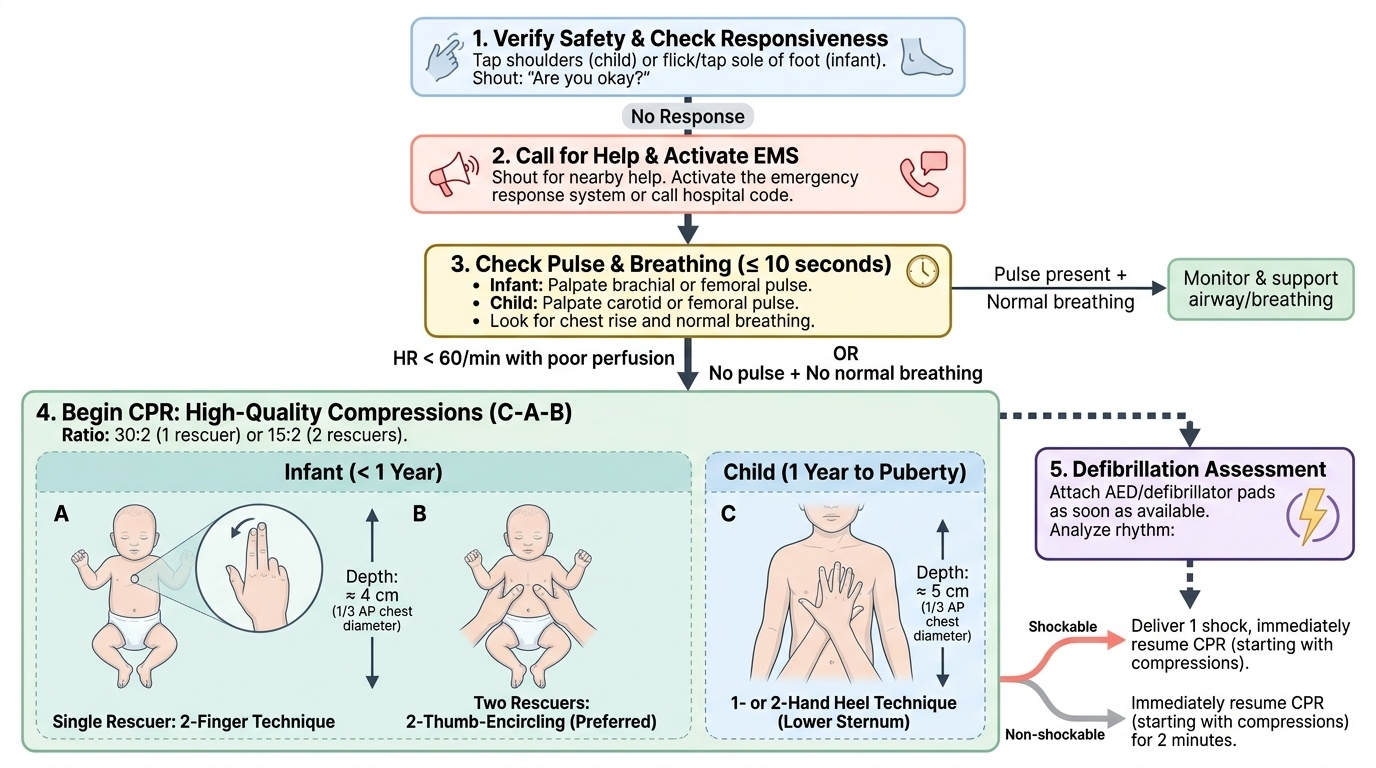
Paediatric basic life support (BLS) follows the C-A-B sequence (Compressions → Airway → Breathing) rather than the traditional A-B-C, because cardiac output and coronary perfusion must be established promptly in arrested patients. The sequence is as follows:
Provided image
Step 1 — Ensure safety and check responsiveness. Tap the child's shoulders and call aloud; tap the foot of an infant. If no response, shout for help and activate the emergency response system (in hospital: call code).
Step 2 — Simultaneously check pulse and breathing (≤10 seconds). In infants: brachial or femoral pulse. In children: carotid or femoral pulse. If absent pulse (or HR <60/min with poor perfusion) and no normal breathing, begin CPR immediately.
Step 3 — Compressions. Position the child supine on a firm surface.
• Infants (<1 year): 2-finger technique (middle and ring fingers over the centre of the chest, just below the nipple line) for a single rescuer; 2-thumb-encircling technique for two rescuers (thumbs over mid-sternum, hands encircle the chest — preferred as it generates higher peak aortic pressure).
• Children (1 year to puberty): heel of one or two hands over the lower half of the sternum (two-hand technique preferred for larger children).
• Depth: compress to one-third the anteroposterior (AP) chest diameter — approximately 4 cm in infants and approximately 5 cm in children. Do not exceed 6 cm.
• Rate: 100–120 compressions per minute for all ages.
• Recoil: allow full chest recoil after each compression; do not lean on the chest.
• Interruptions: minimise to <10 seconds; high-quality uninterrupted CPR is the most important determinant of outcome.
Step 4 — Airway. Open the airway using head-tilt chin-lift (no cervical spine injury) or jaw-thrust (suspected cervical injury). In infants, use a neutral/sniffing position; in children, use slight extension.
Step 5 — Breathing. Deliver two rescue breaths (1 second each, visible chest rise). In infants: mouth-to-mouth-and-nose. In children: mouth-to-mouth with nose pinched. In a healthcare setting, use a bag-valve-mask (BVM) with supplemental oxygen.
Compression-to-ventilation ratio:
• Single rescuer (infant or child): 30:2
• Two rescuers (infant or child): 15:2
• Exception: Once an advanced airway (endotracheal tube, LMA) is in place, give continuous compressions at 100–120/min with asynchronous ventilation at 10 breaths/min — do NOT pause compressions for each breath.
AED use: attach as soon as available; use paediatric pads/key (for children <8 years or <25 kg) if available to reduce energy delivery; if only adult pads available, proceed with them. Defibrillation is ONLY for shockable rhythms — do not shock asystole or PEA.
SELF-CHECK
A 2-year-old child is found unresponsive and pulseless. Two rescuers are present. What is the correct compression-to-ventilation ratio and compression depth for this child?
A. 30:2 with depth 2 cm
B. 15:2 with depth one-third AP diameter (~5 cm)
C. 30:2 with depth one-third AP diameter (~5 cm)
D. 15:2 with depth one-half AP diameter (~7 cm)
Reveal Answer
Answer: B. 15:2 with depth one-third AP diameter (~5 cm)
For a child (1 year to puberty) with TWO rescuers, the PALS ratio is 15:2 (not 30:2 which applies to a single rescuer). Compression depth should reach one-third the anteroposterior chest diameter, approximately 5 cm in a child. Depths of 2 cm are inadequate to generate sufficient intrathoracic pressure, and half the AP diameter (7 cm) exceeds the recommended maximum of 6 cm.