Page 22 of 31
PE24.17-20 | Emergency Thermal Care — SDL Guide (Part 2)
Managing Hypothermia: Warm Chain and Kangaroo Mother Care
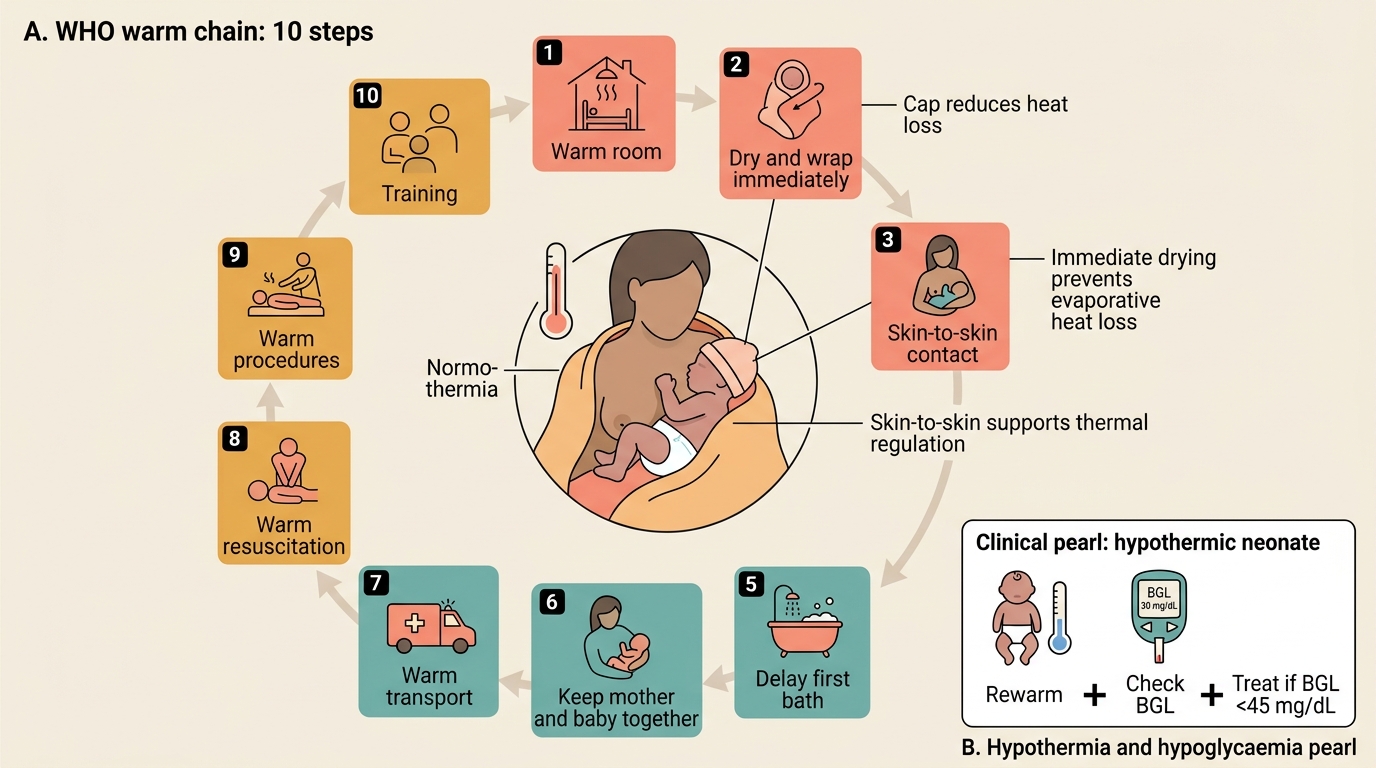
Management of hypothermia in a neonate or young child requires both rewarming (restoring normal temperature) and prevention of recurrence (environmental measures). The WHO warm chain operationalises this as a sequence of ten interlinked actions that span the entire care episode from delivery through discharge. Disrupting any single step creates the conditions for hypothermia; maintaining all ten simultaneously is the prevention standard. It is important to understand that the warm chain is not merely a neonatal ward guideline — it is a systems framework that requires every person in the care chain to act correctly at every contact with the baby. A delivery room nurse who dries the baby immediately and then hands the baby to a midwife who carries it across a cold corridor to a cold weighing scale has broken the chain at step 2. This is why training (step 10) is the last but also the most durable link: without staff who understand the physiology and the rationale, the other nine steps are routinely violated in resource-limited settings. The warm chain is therefore as much a quality-improvement tool as a clinical guideline, and internalising it is essential for any clinician who will supervise maternal and neonatal care.
The WHO Warm Chain — 10 steps:
1. Warm room — delivery room temperature ≥25°C (ideally 28°C for preterm); ward temperature maintained; windows closed.
2. Warm and dry immediately — dry the baby thoroughly within seconds of delivery using a pre-warmed towel; remove the wet towel and replace with a dry one. Drying is the most critical single step.
3. Skin-to-skin contact (Kangaroo Mother Care) — place the naked baby on the mother's bare chest, prone, between her breasts, immediately after drying.
4. Breastfeeding — breastmilk provides calories for thermogenesis; early breastfeeding within 1 hour of birth.
5. Delay first bath — first bath is delayed until at least 24 hours after birth (WHO recommendation); earlier bathing causes rapid heat loss through evaporation.
6. Keep mother and baby together — do not separate well babies from their mothers for nursery routines.
7. Warm transport — if transfer is needed, wrap warmly, use a warm transport incubator or KMC during transport.
8. Warm resuscitation — all resuscitation equipment (radiant warmer, dry towels) must be pre-warmed before use.
9. Warm procedures — any examination, blood draw, or procedure should be performed under a radiant warmer with the baby covered as much as possible.
10. Training — all staff caring for newborns must understand and implement all 10 steps.
Kangaroo Mother Care (KMC) — technique:
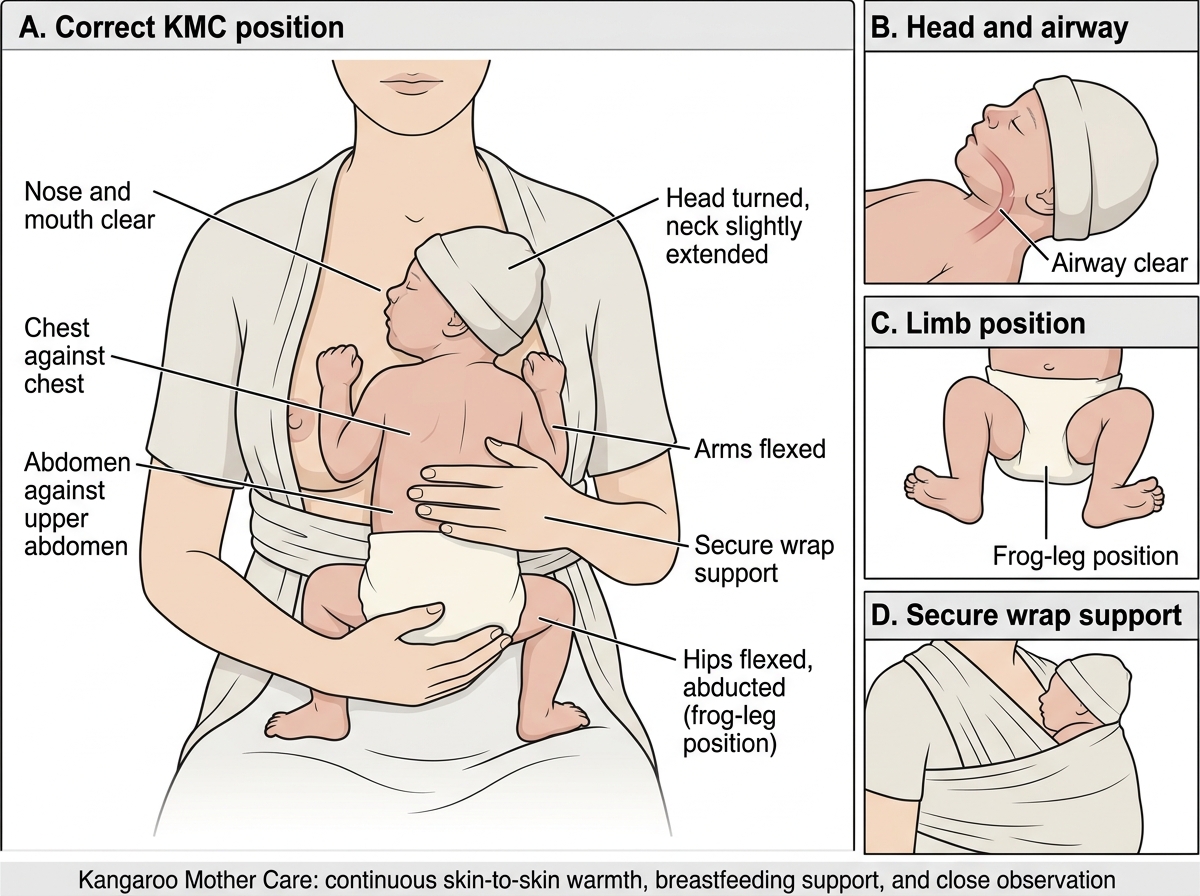
KMC is the practice of skin-to-skin contact between a mother (or trained caregiver) and a newborn, with the infant placed upright and prone on the parent's bare chest. The evidence base is strong: multiple randomised trials show KMC reduces neonatal mortality, hypothermia episodes, infection rates, and hospital stay in low-birthweight and preterm infants.
Correct KMC positioning:
• Infant placed upright between mother's breasts, prone (face forward, head in 'sniffing position' to maintain airway)
• Infant wears a nappy and a hat; the rest of the body is skin-to-skin
• Mother's clothing wraps around both infant and mother to secure position
• The infant's head should be turned to one side with the neck slightly extended — not flexed (risk of airway obstruction)
• Infant's abdomen is at the level of the mother's epigastrium
• Mother can move, walk, and sleep in a semi-reclined position
Advantages of KMC over a radiant warmer: zero cost, stimulates breastfeeding via skin contact and oxytocin, promotes bonding, reduces infection risk (mother's skin flora is safer than hospital surfaces), and can be continued during transport.
Rewarming a hypothermic neonate:
For mild-to-moderate hypothermia: KMC is first-line if the infant is stable and able to feed. Place under a radiant warmer if KMC is not possible. Rewarm gradually (no faster than 1°C/hour) — rapid rewarming risks cutaneous vasodilation and hypotension. Check blood glucose every 30 minutes during rewarming (hypoglycaemia is the primary metabolic complication). Repeat axillary temperature every 15–30 minutes until ≥36.5°C for two consecutive readings.
Correct Kangaroo Mother Care Position
WHO Warm Chain for Newborn Thermal Care
CLINICAL PEARL
Always check blood glucose in a hypothermic neonate. Hypothermia and hypoglycaemia frequently co-exist: the metabolic stress of cold triggers glucose consumption for thermogenesis, rapidly depleting the neonate's already-limited glycogen stores. A baby who appears lethargic from 'just hypothermia' may actually have a BGL of 30 mg/dL and will not improve with warming alone until the glucose is corrected. The sequence is: rewarm + check BGL + treat hypoglycaemia if BGL <45 mg/dL. Never address only one without the other.
Managing Hyperthermia and Heat Stroke in Children
Hyperthermia in children has two main causes with different mechanisms and management: fever (elevated hypothalamic set point from pyrogens, part of the inflammatory response) and heat stroke (failure of thermoregulation from environmental heat load exceeding the body's dissipation capacity). The clinical distinction matters because management is different: fever responds to antipyretics (paracetamol) and treating the underlying infection; heat stroke requires emergency physical cooling because the hypothalamic set point is not elevated — the body is simply overheating and antipyretics are ineffective.
Fever management in children:
Fever (axillary >37.5°C) is a physiological response to infection and is not harmful at moderate levels. The indication for antipyretic treatment is primarily comfort — to relieve the distress associated with high fever — and to reduce the risk of febrile seizures in susceptible children. Paracetamol (acetaminophen) is the first-line antipyretic: dose 10–15 mg/kg every 4–6 hours (maximum 5 doses in 24 hours). Ibuprofen is an alternative in children over 3 months (5–10 mg/kg every 6–8 hours). Aspirin is contraindicated in children due to the risk of Reye's syndrome.
Tepid sponging (lukewarm water, not cold or alcohol) can reduce fever temperature but does not treat the underlying set-point elevation and should be used as a supplement, not a replacement, for antipyretics. Cold sponging or ice packs cause vasoconstriction and shivering, which counterproductively generate heat — use tepid water only.
Heat stroke — recognition and emergency management:
Heat stroke occurs when environmental heat load exceeds the body's dissipation capacity — most commonly in infants left in closed cars in summer, during heat waves, or in children with anhidrotic conditions. The defining features are: (1) core temperature >40°C; (2) CNS dysfunction (confusion, agitation, seizures, loss of consciousness); (3) history of heat exposure or exertion; (4) often absent sweating (classic heat stroke).
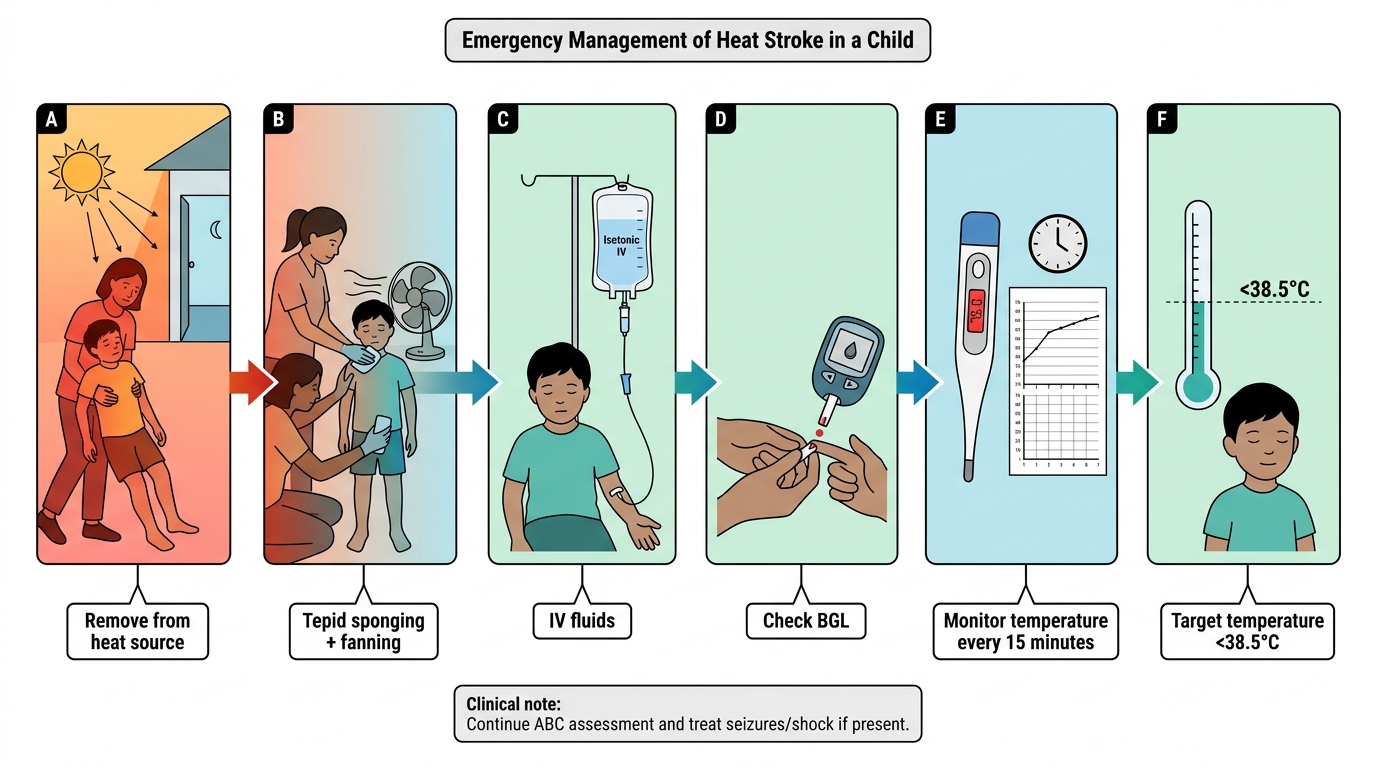
Emergency cooling for heat stroke:
• Remove from heat source immediately
• Remove all clothing
• Tepid water sponging + fanning (evaporative cooling) — most effective non-invasive method
• Apply ice packs to groin, axillae, and neck (areas of large vessels) if available
• IV or oral fluids to replace volume
• Check BGL and treat hypoglycaemia
• Oxygen supplementation
• Target: core temperature <38.5°C — stop active cooling at this point to avoid overshoot hypothermia
• Monitor temperature every 15 minutes during cooling
• Refer urgently to higher centre if CNS signs (seizures, loss of consciousness) — these indicate serious heat illness requiring ICU care
Emergency Management of Pediatric Heat Stroke
SELF-CHECK
A 4-month-old infant is found unresponsive in a hot car. His temperature is 41.2°C. He is not sweating and has a seizure. What is the SINGLE most important immediate intervention?
A. Administer paracetamol 15 mg/kg rectally
B. Initiate tepid water sponging and fanning for evaporative cooling while removing clothing
C. Give IV diazepam 0.3 mg/kg for the seizure as the first action
D. Apply ice packs to the entire body surface
Reveal Answer
Answer: B. Initiate tepid water sponging and fanning for evaporative cooling while removing clothing
This is heat stroke (temperature >40°C + CNS dysfunction + heat exposure). Antipyretics are ineffective in heat stroke — they lower the hypothalamic set point, which is not elevated here; the problem is environmental heat overload. The first action is emergency cooling: remove from heat source, remove clothing, tepid sponging + fanning (evaporative cooling). Ice packs to groin/axillae/neck (not whole body — whole-body ice causes vasoconstriction and shivering, which generates more heat). Diazepam is needed if the seizure persists, but cooling is the primary intervention.
Interpretation and Monitoring: Ongoing Temperature Maintenance
After initiating warming or cooling measures, ongoing monitoring is essential to track the response, detect complications, and adjust the intervention. Temperature management is not a one-time action but a continuous clinical process, particularly in neonates whose temperature is highly labile and dependent on the environment at every moment. A neonate who reaches 36.5°C after one hour of KMC may drop below that threshold again within 30 minutes if the environmental measures are not sustained — clothing removed for a blood draw, a door left open, the mother taken away for a procedure. This vulnerability is why the monitoring protocol specifies repeated measurements rather than a single target temperature, and why environmental controls are listed as a formal part of the management plan rather than background assumptions. Clinicians who understand temperature lability in neonates instinctively check the environment whenever a baby is reported as 'not improving' with warming — the most common reason is a break in the environmental measures, not a failure of the warming intervention itself. Similarly, a child being cooled for heat stroke can overshoot into hypothermia if cooling is not stopped at the target temperature; monitoring every 15 minutes is what prevents this overshoot.
For a hypothermic neonate undergoing rewarming, the monitoring protocol is:
• Axillary temperature every 15–30 minutes during rewarming
• Target: reach ≥36.5°C within 2–4 hours of initiating rewarming, then maintain
• Blood glucose check every 30 minutes during rewarming — hypoglycaemia must be identified and corrected simultaneously
• Observe clinical response: improving tone, spontaneous movement, attempts to feed = favourable signs; persistent lethargy, worsening colour, or respiratory distress despite warming = investigation for sepsis or other cause
• Confirm sustained normothermia: two consecutive readings ≥36.5°C at least 30 minutes apart before discontinuing intensive warming
Environmental measures to maintain normal temperature (PE24.19):
Preventing hypothermia is far preferable to treating it. The following environmental controls are standard in any paediatric ward or neonatal care area:
• Room temperature: maintain at ≥25°C in general wards, ≥28°C in neonatal areas; use a room thermometer, not subjective assessment
• Avoid draughts: close windows and doors during procedures; position beds away from windows and air-conditioning vents
• Clothing and wrapping: dress the baby in warm clothes appropriate for the season; a hat prevents significant heat loss from the large head surface area in neonates
• Pre-warm examination surfaces: place a warm towel on the examination table before undressing the baby for examination; never place a baby on a cold metal surface
• Post-procedure wrapping: immediately re-dress and wrap after any examination or procedure
• Monitoring environment: teach parents to check for cold hands and feet as an early sign of thermal stress before the core temperature drops
For a child with heat stroke undergoing cooling:
• Temperature every 15 minutes
• Stop active cooling when temperature reaches 38.5°C — continue monitoring to detect rebound hyperthermia
• Neurological status assessment every 30 minutes — improving consciousness = favourable; persistent seizures or coma = ICU referral
SELF-CHECK
Which of the following is the most important immediate step in the WHO warm chain immediately after a hospital delivery?
A. Weigh the baby on the digital scale
B. Apply vitamin K injection
C. Thoroughly dry the baby and replace the wet towel with a dry warm one
D. Place the baby under the radiant warmer for 30 minutes before giving to the mother
Reveal Answer
Answer: C. Thoroughly dry the baby and replace the wet towel with a dry warm one
Drying immediately and thoroughly is the most critical step in preventing neonatal hypothermia — evaporation from wet skin is the dominant heat loss mechanism in the first minutes of life. The wet towel is replaced with a dry one immediately. Weighing should be delayed until after drying and skin-to-skin contact is established. Vitamin K is important but not the first priority. Separating the baby from the mother for a radiant warmer is not necessary for a well baby and breaks the warm chain; skin-to-skin contact (KMC) is equally effective and preferred.
Supervised Practice: Temperature Assessment and Thermal Care Scenarios
Temperature assessment and thermal care are practical skills that require hands-on practice to execute correctly under the time pressure of a neonatal emergency. The skin of a neonate is an unreliable subjective thermometer; only an axillary reading gives you the information you need to classify and act. Similarly, KMC positioning — which looks simple in a photograph — requires practice to achieve the correct head alignment, chest positioning, and clothing wrap that ensure both airway safety and effective warmth transfer. The supervised practice scenarios below should be completed in the clinical setting during your paediatric posting.
Scenario A — Correct thermometry technique:
On a clinical patient (under supervision) or a mannequin: ensure axilla is dry; place thermometer bulb correctly in the axilla centre; hold the arm firmly against the chest wall; record reading after the digital beep (or 3 minutes for a glass thermometer). Classify the reading using the correct temperature thresholds. State what value would indicate mild, moderate, and severe hypothermia.
Scenario B — KMC positioning:
With a nursing doll or supervised on a patient: place the doll prone and upright between the 'mother's' breasts; ensure the head is in a neutral position (not flexed forward); ensure the nappy and hat are in place; wrap the clothing around both; verbally describe the safety check (airway visible, head not flexed, abdomen at epigastric level, limbs in frog-leg position).
Scenario C — Warm chain checklist application:
In the delivery room or simulation setting: go through each of the 10 warm chain steps verbally and demonstrate those that are simulatable (drying technique, room temperature check, surface pre-warming, KMC initiation, delay of bath).
Scenario D — Hypothermic neonate management sequence:
For a simulated 2-day-old with axillary temperature 35.0°C: state the classification (moderate hypothermia); initiate KMC or radiant warmer; check BGL and treat if low; state monitoring frequency (temperature every 15–30 min; BGL every 30 min); state the target temperature and when to confirm recovery (two readings ≥36.5°C).
Environmental measures documentation:
| Setting | Minimum room temperature | Key additional measures |
|---|---|---|
| Delivery room | ≥25°C (28°C for preterm) | Pre-warm surfaces, no draughts, immediate drying |
| Postnatal ward | ≥25°C | Clothing + hat, KMC, avoid fans near neonate |
| Sick newborn unit | ≥28°C | Radiant warmer/incubator, minimise procedures, warm resuscitation |
| Transport | Maintain 36.5–37.5°C | KMC during transport, warm blankets, monitor thermometer |