Page 13 of 31
PE24.4 | Status Epilepticus — SDL Guide (Part 2)
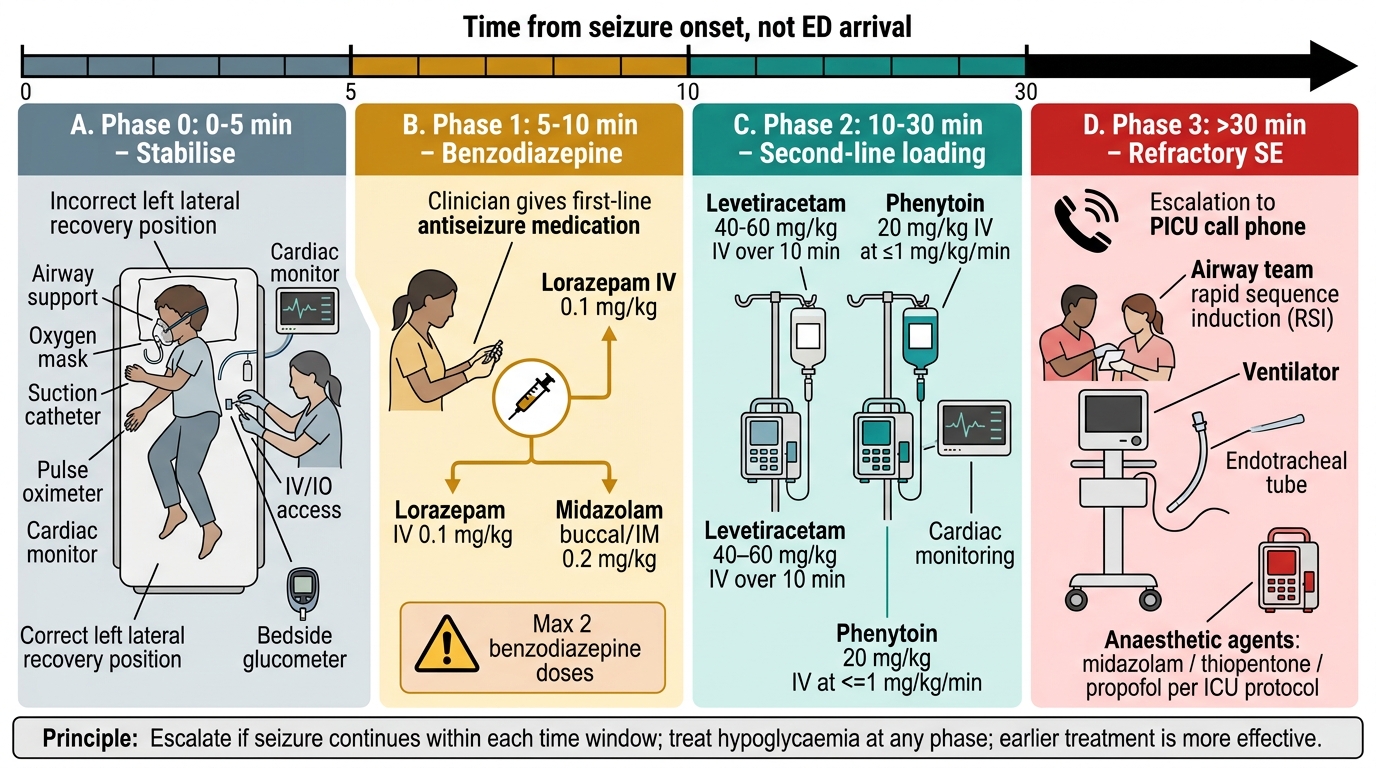
Management of Status Epilepticus: Time-Based Algorithm
The management of status epilepticus is governed by a time-based algorithm in which each phase has a defined drug choice, dose, and route, and failure to respond to a phase within its time window triggers escalation to the next phase. The principle underlying the algorithm is that earlier drugs are more effective (due to receptor availability) but more is not better at any single phase — giving a second dose of benzodiazepine beyond the recommended 2 doses increases the risk of respiratory depression without meaningfully improving seizure control. The time stamps are from onset of continuous seizure, not from arrival at the emergency department.
Phase 0 (0–5 minutes): Stabilise, recognise, prepare
While the seizure is still within the 'possibly self-limiting' window:
• Protect airway: position the child in recovery/left lateral position; suction oral secretions; jaw-thrust if airway obstructed
• Apply oxygen via face mask or nasal cannula; target SpO₂ ≥94%
• Establish IV or IO access simultaneously (do not delay treatment waiting for IV)
• Check bedside blood glucose immediately — treat hypoglycaemia at any phase
• Place on continuous SpO₂ and cardiac monitoring
• Call for help — notify senior and prepare intubation equipment
Phase 1 (5–10 minutes): First-line — Benzodiazepine
If the seizure is still continuing at 5 minutes, this is SE — give a benzodiazepine:
• IV/IO access available: lorazepam 0.1 mg/kg IV/IO (maximum single dose 4 mg); administer over 1–2 minutes. Onset 2–5 minutes. Can repeat ONCE after 5 minutes if no response (maximum 2 doses total).
• No IV/IO access: midazolam buccal 0.2–0.3 mg/kg (maximum dose 10 mg) — squirt into the buccal mucosa between the cheek and gum; or midazolam IM 0.2 mg/kg. Alternative if midazolam unavailable: diazepam rectal 0.5 mg/kg (maximum 10 mg) via rectal tube.
• Diazepam IV 0.2–0.3 mg/kg (maximum 10 mg) is an alternative to lorazepam when lorazepam is unavailable, but has a shorter anticonvulsant duration due to rapid redistribution.
• Monitor for respiratory depression after each benzodiazepine dose — have bag-valve-mask ready.
Phase 2 (10–30 minutes): Second-line — Non-benzodiazepine antiepileptic
If the seizure persists after 2 benzodiazepine doses, give a second-line agent:
• Phenytoin 18–20 mg/kg IV over 20 minutes (rate ≤1 mg/kg/min to avoid cardiac arrhythmia and hypotension; maximum rate 50 mg/min in adults). Phenytoin must be diluted in 0.9% saline (precipitates in dextrose). Monitor ECG and BP during infusion.
• Fosphenytoin 18–20 mg/kg PE (phenytoin equivalents) IV or IM: the prodrug of phenytoin; can be given more rapidly (≤150 mg PE/min) and IM (unlike phenytoin). Does NOT precipitate in dextrose.
• Levetiracetam 40–60 mg/kg IV (maximum 3000 mg) over 5–10 minutes: the ConSEPT (NZ/Australia) and EcLiPSE (UK) trials (both published 2019) demonstrated that levetiracetam is non-inferior to phenytoin for second-line treatment of paediatric SE and has a more favourable safety profile (no cardiac monitoring required, no precipitation in dextrose). Levetiracetam is increasingly preferred as the second-line agent in paediatric practice.
• Phenobarbitone 15–20 mg/kg IV over 20–30 minutes: historically second-line but now third-line in many algorithms; remains first-line in neonates (where phenytoin is less effective due to immature sodium channel expression). Significant sedation and respiratory depression.
Phase 3 (>30 minutes): Refractory SE — Intensive care
SE persisting beyond 30 minutes despite phases 1 and 2 is refractory SE — requiring intensive care and anaesthetic management:
• Call PICU immediately
• Rapid sequence intubation (RSI) for airway protection and controlled ventilation
• Anaesthetic agents as continuous infusions: midazolam infusion (0.05–2 mg/kg/h), propofol (avoid in children <16 yr — paediatric propofol infusion syndrome), ketamine (0.5–3 mg/kg/h), or thiopentone (3–5 mg/kg bolus, then infusion) — all require continuous EEG monitoring to confirm burst-suppression and assess for NCSE
• Continue treating metabolic causes concurrently
| Drug | Dose | Route | Rate / Notes |
|---|---|---|---|
| Lorazepam | 0.1 mg/kg (max 4 mg) | IV/IO | Over 1–2 min; repeat once after 5 min |
| Midazolam | 0.2–0.3 mg/kg (max 10 mg) | Buccal/IM | For no-IV access; buccal = between cheek and gum |
| Diazepam | 0.2–0.3 mg/kg (max 10 mg) IV; 0.5 mg/kg (max 10 mg) rectal | IV or rectal | IV: over 2–3 min; rectal if no IV/buccal midazolam |
| Phenytoin | 18–20 mg/kg (max 1000 mg) | IV only (in 0.9% saline) | ≤1 mg/kg/min; ECG monitoring; not IM |
| Fosphenytoin | 18–20 mg PE/kg (max 1500 mg PE) | IV or IM | ≤150 mg PE/min IV; can give IM |
| Levetiracetam | 40–60 mg/kg (max 3000 mg) | IV | Over 5–15 min; no ECG monitoring needed |
| Phenobarbitone | 15–20 mg/kg (max 1000 mg) | IV | Over 20–30 min; first-line in neonates |
Time-Based Management of Pediatric Status Epilepticus
SELF-CHECK
A 6-year-old child (weight 20 kg) with known epilepsy on sodium valproate presents with a generalised tonic-clonic seizure lasting 12 minutes. She has received one dose of IV lorazepam 0.1 mg/kg (2 mg) 5 minutes ago with no response. The seizure continues. What is the most appropriate next step?
A. Give a second dose of IV lorazepam 0.1 mg/kg immediately
B. Give IV phenytoin 18 mg/kg at ≤1 mg/kg/min or IV levetiracetam 40-60 mg/kg
C. Give IM midazolam 0.2 mg/kg as the second benzodiazepine
D. Wait 5 more minutes before escalating to a second-line agent
Reveal Answer
Answer: B. Give IV phenytoin 18 mg/kg at ≤1 mg/kg/min or IV levetiracetam 40-60 mg/kg
After ONE dose of IV lorazepam with no response at 5 minutes, the next step is a second benzodiazepine dose (lorazepam × 1 more) OR escalation to Phase 2 (second-line agent). Since the seizure has already lasted 12 minutes and one lorazepam dose has failed, the algorithm supports moving directly to the second-line agent: phenytoin 18-20 mg/kg IV (in saline, rate ≤1 mg/kg/min, max 400 mg for this 20 kg child) or levetiracetam 40-60 mg/kg IV (800-1200 mg). Option A (a second lorazepam) is appropriate ONLY if lorazepam was given once and 5 minutes have elapsed — but here the question already shows the first dose has been given 5 minutes ago and failed; a second benzodiazepine could be given but escalation to second-line is the priority. The ConSEPT/EcLiPSE trials support levetiracetam as equivalent to phenytoin with a better safety profile.
CLINICAL PEARL
Glucose first, always. Before reaching for the lorazepam, check (or assume and treat) the blood glucose. A seizing hypoglycaemic child will not stop seizing with benzodiazepines alone — treating hypoglycaemia may abort the seizure entirely or significantly improve the response to antiepileptics. The glucose check takes 30 seconds; do it while the benzodiazepine is being drawn up.
Every minute of SE increases benzodiazepine resistance. The GABA-A receptor internalisation that begins at 5–10 minutes of sustained seizure is the pharmacological reason the treatment algorithm is time-based, not response-based. This is why guidelines mandate that phenytoin/levetiracetam should not wait until 'one more benzodiazepine has failed' — the window for effective Phase-2 drug action narrows with every minute of delay. Give Phase-2 drugs at 15–20 minutes, not at 30 minutes.
Isoniazid (INH) and pyridoxine. In areas of high TB prevalence (including India), isoniazid toxicity is an important reversible cause of refractory SE in children on TB treatment. INH depletes pyridoxine (vitamin B6) → reduces GABA synthesis → severe SE refractory to all standard antiepileptics. The antidote is pyridoxine 70 mg/kg IV (up to 5 g). Suspect this in any child on INH who presents with refractory SE.
Self-Assessment: Status Epilepticus
Test your knowledge and clinical reasoning across the full scope of this module before your next paediatric clinical encounter or examination. The drug-dosing questions require you to calculate both the dose in mg/kg AND convert to a volume given the concentration of the available preparation — this two-step calculation is the format used in MBBS OSCEs and prescribing assessments. For the algorithm questions, describe each phase with its time window, drug name, dose, and route — not just the name of the drug. This level of detail is what separates a safe clinical response from a generic answer. The GABA-A receptor internalisation question (question 4) is a conceptual rather than a factual question — practise explaining the mechanism in your own words as if you are teaching a junior colleague, because this is the explanation you will be expected to give in a viva or clinical teaching session. For the ConSEPT/EcLiPSE question, memorise not just the conclusion (levetiracetam non-inferior) but the trial populations and endpoints, as these are frequently tested in structured clinical examinations at the postgraduate entrance level.
- Define status epilepticus using the ILAE 2015 operational definition. Why was the older 30-minute definition replaced?
- A 10-year-old child (weight 30 kg) is having a generalised tonic-clonic seizure for 9 minutes. There is IV access. Calculate the lorazepam dose in mg and state the maximum single dose.
- The same child does not respond to the maximum benzodiazepine doses. You decide to use levetiracetam. Calculate the dose (using 40 mg/kg) and give the infusion rate.
- Why does benzodiazepine efficacy decrease with time in SE? What is the molecular mechanism?
- List THREE metabolic causes of seizures in children that must be corrected alongside antiepileptic drugs.
- What is the significance of the ConSEPT and EcLiPSE trials for second-line SE management?
Answers:
1. ILAE 2015: SE = seizure ≥5 minutes (t1 — treatment threshold) or ≥2 seizures without return to baseline. The 30-minute definition was replaced because seizures lasting >5 min rarely stop spontaneously and benzodiazepine efficacy declines with duration due to GABA-A receptor internalisation — earlier treatment is more effective.
2. Lorazepam 0.1 mg/kg × 30 kg = 3 mg IV. Maximum single dose = 4 mg. If the 3 mg dose fails, a second 3 mg dose (not exceeding 4 mg/dose) can be given after 5 minutes.
3. Levetiracetam 40 mg/kg × 30 kg = 1200 mg IV over 5–15 minutes. Standard preparation 500 mg/5 mL (100 mg/mL): volume = 1200 mg ÷ 100 mg/mL = 12 mL, diluted in 50–100 mL 0.9% NS, infused over 10–15 min.
4. Sustained SE → GABA-A receptor internalisation (endocytosis) removes receptors from the synaptic membrane → benzodiazepines cannot potentiate GABA-A conductance (their binding site is on the receptor) → progressive pharmacoresistance. This begins at 5–10 min of continuous SE.
5. Any three: hypoglycaemia, hyponatraemia, hypocalcaemia, hypomagnesaemia, pyridoxine deficiency (neonates), isoniazid toxicity.
6. ConSEPT (NZ/Australia) and EcLiPSE (UK), both published 2019: head-to-head RCTs comparing levetiracetam vs phenytoin as second-line SE treatment in children — found levetiracetam NON-INFERIOR to phenytoin for seizure cessation at 60 min; levetiracetam has fewer drug interactions, requires no cardiac monitoring, and does not precipitate in dextrose — supporting its use as first-choice second-line agent.