Page 16 of 31
PE24.{5,15} | Unconscious Child — SDL Guide (Part 2)
Emergency Management: Airway, Glucose, Seizure Control and Safe Positioning
Emergency management of the unconscious child is executed in the same ABCDE priority order as the assessment, with specific interventions for the most common and most reversible causes. The following sequence is based on IAP and WHO emergency guidelines. A critical principle governs this entire management sequence: treat the most reversible life threats first, in the order of the ABCDE framework, without waiting for a definitive diagnosis. The child whose airway is obstructed needs it cleared before anything else — even if you suspect meningitis. The child with a BGL of 30 mg/dL needs dextrose before an LP is contemplated. In practice, the first three to five minutes of paediatric emergency management are almost always the same regardless of the final diagnosis, because the ABCDE interventions buy time for all subsequent diagnostic and specific therapeutic steps. Only after the child is stabilised — airway patent, saturation maintained, IV access established, BGL treated if low — does the search for a specific cause drive individualised treatment.
1. Airway and positioning:
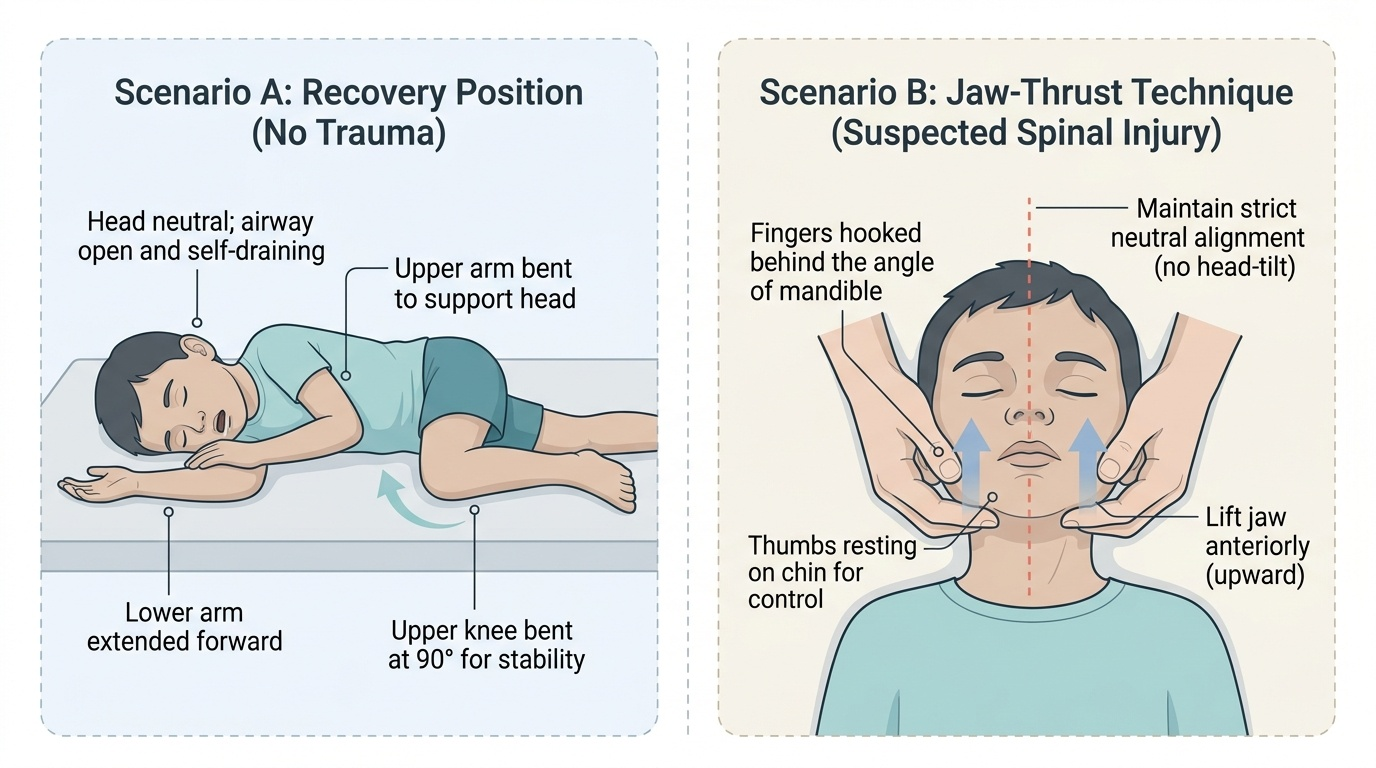
• Unconscious child (no trauma suspected): place in recovery position (left lateral, with upper arm and leg bent forward to stabilise) — this prevents airway obstruction from tongue fall and aspiration of vomit.
• Unconscious child with suspected spinal/head trauma: maintain spinal alignment — jaw-thrust manoeuvre without head extension, neutral spinal position; move as a unit using log-roll technique. Do NOT use standard head-tilt chin-lift if cervical injury is possible.
• Suction oropharynx if secretions/vomit visible.
• Apply oxygen by mask at 6–10 L/min if SpO₂ <95%.
2. Circulation — IV access and fluid:
Establish peripheral IV access (or intra-osseous if IV fails after 2 attempts in 90 seconds). Draw blood simultaneously for: BGL (urgent bedside), FBC, electrolytes, blood culture, and blood gas.
3. Hypoglycaemia treatment — DON'T MISS:
If BGL <45 mg/dL (or if BGL testing is unavailable and clinical suspicion is high): administer 10% dextrose 5 mL/kg IV as a slow bolus over 15 minutes. Do NOT use 50% dextrose in children — the high osmolarity causes vein sclerosis and is unnecessary when 10% is available. Recheck BGL after 15 minutes. If BGL normalises and consciousness improves, the cause was hypoglycaemia; maintain with dextrose-containing IV fluids.
4. Seizure control:
If the child is actively convulsing (or has convulsed and remains post-ictal/comatose):
• First-line: diazepam IV 0.3 mg/kg as a slow intravenous injection (over 2–3 minutes); maximum single dose 10 mg. Repeat once after 5 minutes if seizure persists.
• If IV access is unavailable: diazepam PR 0.5 mg/kg via rectal tube or syringe (without needle). This is the IMNCI community-level intervention that can be administered by trained health workers before hospital transfer.
• Second-line (if seizure persists after two diazepam doses): phenobarbitone 20 mg/kg IV over 20 minutes, or fosphenytoin/phenytoin per protocol.
• Monitor respiratory rate and oxygen saturation throughout — diazepam causes respiratory depression, particularly at higher doses or with rapid administration.
5. Empirical treatment for CNS infection:
If fever + altered consciousness + neck stiffness → empirical ceftriaxone 100 mg/kg/day (max 4 g/day) IV after blood culture, before LP if there is papilloedema or focal neurology. Do not delay antibiotics for LP — it can follow stabilisation.
6. Other emergency interventions by AEIOU-TIPS category:
• DKA: 0.9% saline resuscitation, insulin (specialist protocol)
• Organophosphate: atropine + pralidoxime
• Raised ICP: head elevation 30°, mannitol 0.5–1 g/kg IV, hyperventilation temporarily
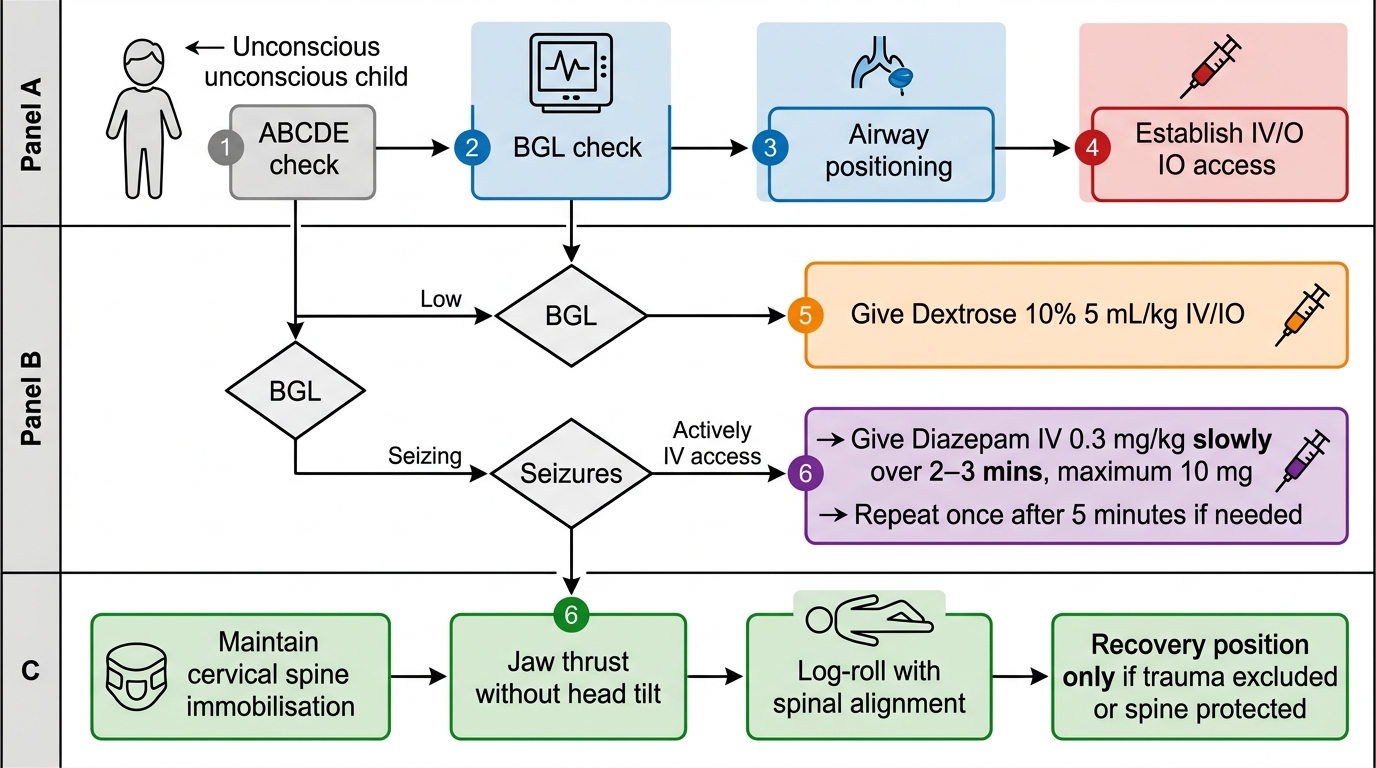
Emergency Algorithm for the Unconscious Child
SELF-CHECK
A 4-year-old is actively seizing. You have peripheral IV access. His BGL is 72 mg/dL. What is the correct first-line anticonvulsant dose?
A. Diazepam IV 0.1 mg/kg over 2–3 minutes
B. Diazepam IV 0.3 mg/kg over 2–3 minutes (max 10 mg)
C. Diazepam IV 0.5 mg/kg as a rapid push
D. Phenobarbitone 20 mg/kg as first-line
Reveal Answer
Answer: B. Diazepam IV 0.3 mg/kg over 2–3 minutes (max 10 mg)
First-line IV anticonvulsant for an actively seizing child in hospital is diazepam 0.3 mg/kg IV slow injection (over 2–3 minutes), maximum single dose 10 mg. It may be repeated once after 5 minutes. The 0.5 mg/kg dose applies to the rectal (PR) route when IV is unavailable. Phenobarbitone is second-line after two diazepam doses have failed. Rapid IV push risks respiratory depression.
Interpreting the Findings: Differentiating Causes from the Clinical Pattern
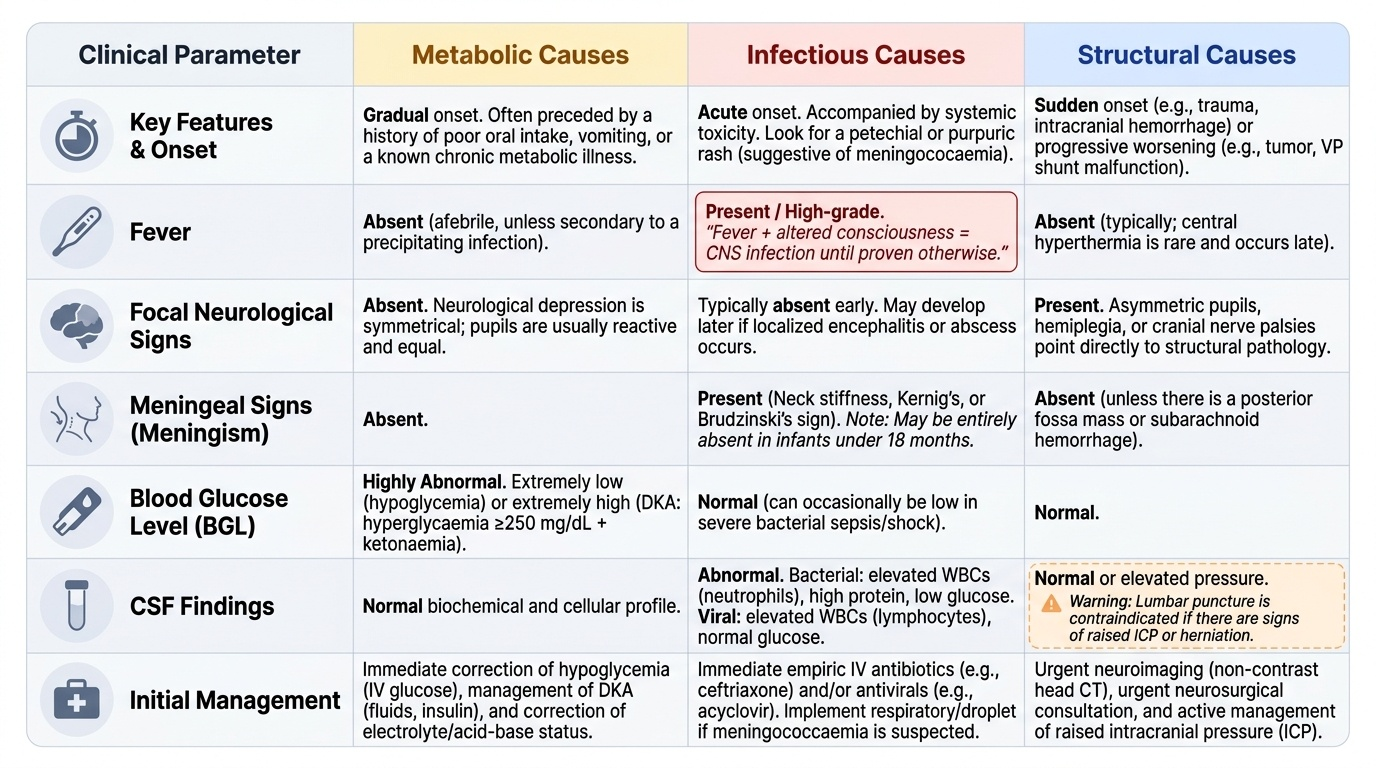
Once the immediate life threats have been addressed — airway secured, BGL checked and treated if low, seizures controlled — the next task is clinical interpretation to guide targeted management. The differential diagnosis of coma in a child is broad, but a structured approach to the pattern of findings usually narrows the field within minutes. The key variables to assess in parallel are: (1) the presence or absence of fever, which sharply divides infectious from non-infectious causes; (2) focal neurological signs (asymmetric pupils, hemiplegia, cranial nerve palsies), which point toward structural pathology; (3) signs of meningeal irritation (neck stiffness, Kernig's, Brudzinski's), which localise to the meninges or posterior fossa; (4) the metabolic context (BGL, electrolytes, acid-base status), which identifies reversible biochemical causes; and (5) the history of access to medications, agricultural chemicals, or a fall, which raises toxic or traumatic causes. Combining these five axes generates a provisional diagnosis within the first five minutes of assessment, directing the next investigation and the specific first-line treatment. No single finding is pathognomonic, but the combination of fever + meningism + altered consciousness is bacterial meningitis until proven otherwise, and the combination of low BGL + seizure + altered consciousness is hypoglycaemia until proven otherwise — both require immediate treatment without waiting for confirmatory tests.
Provided image
Metabolic causes (hypoglycaemia, DKA, hyponatraemia, hepatic encephalopathy, inborn errors of metabolism) present with:
• Gradual onset, often in a context of poor intake, vomiting, or chronic illness
• No focal neurological signs early
• Metabolic acidosis on blood gas, electrolyte abnormalities
• BGL either very low (hypoglycaemia) or very high (DKA hyperglycaemia >250 mg/dL + ketonaemia)
• Consciousness improves with metabolic correction
Infectious causes (bacterial meningitis, viral encephalitis, cerebral malaria, septic encephalopathy) present with:
• Fever + altered consciousness (both together = CNS infection until proven otherwise)
• Meningism (neck stiffness, Kernig's, Brudzinski's signs) — may be absent in infants <18 months
• Petechial/purpuric rash = meningococcaemia (immediate ceftriaxone + isolation)
• Photophobia, Bulging anterior fontanelle in infants
• CSF: turbid, elevated WBC, low glucose, high protein (bacterial); clear, lymphocytic, normal/mildly low glucose (viral)
Structural causes (traumatic brain injury, space-occupying lesion, stroke) present with:
• Focal neurological signs: asymmetric pupil response, hemiplegia, cranial nerve palsies
• Unilateral fixed dilated pupil = uncal herniation — neurosurgical emergency
• Decorticate posturing (arms flexed, legs extended) = upper midbrain/diencephalon lesion
• Decerebrate posturing (arms extended, legs extended) = lower midbrain/pons lesion — ominous
• CT head is the definitive investigation for structural causes; do NOT delay treatment for CT if the child is deteriorating
Toxic causes (organophosphate, benzodiazepine, anticonvulsant overdose, alcohol) present with:
• Miosis (organophosphate: pin-point pupils + salivation + bronchospasm — SLUDGE symptoms)
• Absent gag reflex, flaccid tone with benzodiazepines
• History of access to medications or agricultural chemicals
• Specific antidotes: atropine + pralidoxime for organophosphate; flumazenil for benzodiazepine (used cautiously)
Serial monitoring: GCS should be reassessed every 15–30 minutes in the acute phase. Falling GCS = active deterioration requiring reassessment of the ABCDE and escalation. Improving GCS after dextrose = hypoglycaemia confirmed; improving after antibiotics = infection. If consciousness does not improve despite normalisation of glucose and absence of seizures, a structural cause must be excluded by imaging.
SELF-CHECK
A 2-year-old with fever and GCS 9 is brought in. She has a stiff neck and non-blanching petechiae on the legs. What is the single most important immediate action?
A. Perform lumbar puncture immediately to confirm diagnosis
B. Order urgent CT brain before any treatment
C. Administer empirical ceftriaxone IV immediately after blood cultures, before LP
D. Check blood glucose and give 10% dextrose first
Reveal Answer
Answer: C. Administer empirical ceftriaxone IV immediately after blood cultures, before LP
Non-blanching petechiae + fever + meningism = meningococcal disease until proven otherwise. Empirical ceftriaxone 100 mg/kg/day IV must be given immediately after blood cultures. LP is not done first: papilloedema or focal signs contraindicate LP until CT excludes raised ICP, and even without these signs, antibiotic delay for LP confirmation is not justified when clinical suspicion is this high. BGL should still be checked, but antibiotics are the priority here given the very specific clinical syndrome.
Applied Practice and Supervised Scenarios
Emergency skills are learned through repeated structured practice — reading about positioning does not create muscle memory for the moment a child is deteriorating in front of you. This section outlines the supervised practice scenarios you should complete, either in a simulation laboratory or at the bedside under direct supervision, before considering this competency achieved.
Provided image
Scenario A — Positioning the unconscious child (no trauma):
Practice placing a mannequin or a cooperative subject in the recovery position: left lateral decubitus, lower arm extended forward, upper arm bent at elbow resting on the surface, upper knee bent forward to act as a stabiliser. Verify the airway is open (head neutral, no obstruction). Practice inserting a Guedel airway (correct sizing: length = corner of mouth to ear lobe).
Scenario B — Positioning with suspected spinal trauma:
Practice jaw-thrust without head-tilt: two-handed grip, fingers behind the angle of the mandible, thumbs on the chin, lifting the jaw anteriorly without extending the neck. Practice log-roll technique with a partner to maintain spinal alignment while turning the child to recovery position or to apply a cervical collar.
Scenario C — Blood glucose check and dextrose administration:
In a simulated IV environment: check capillary BGL using glucometer; draw up 10% dextrose at 5 mL/kg for a specified child weight (e.g., 15 kg child = 75 mL 10% dextrose); administer via peripheral IV over 15 minutes. Document result and intervention. Verbally state what concentration NOT to use (50% dextrose is contraindicated in children).
Scenario D — IV/PR diazepam for a convulsing child:
For IV route: draw up diazepam 0.3 mg/kg for a specified weight (e.g., 12 kg = 3.6 mg; round to 4 mg); dilute in 10 mL normal saline; administer slowly over 2–3 minutes; state maximum dose (10 mg) and monitoring parameters (respiratory rate, SpO₂).
For PR route: draw up diazepam 0.5 mg/kg for specified weight; attach a small catheter to the syringe (no needle); advance 5 cm into rectum; inject and hold buttocks together for 30 seconds.
Documentation checklist after any emergency intervention:
Time of intervention, drug/dose/route, response (GCS before and after), BGL before and after, any adverse effects noted (respiratory depression, hypotension). This documentation is legally required and serves as the clinical handoff to the next team.