Page 1 of 23
PE25.1 | Acute Otitis Media — SDL Guide
Learning Objectives
- Describe the etio-pathogenesis of acute otitis media including the role of common bacterial and viral pathogens
- Recognise the clinical features of AOM in infants and children including otoscopic findings
- Apply diagnostic criteria to differentiate AOM from otitis media with effusion
- Apply watchful waiting criteria and select appropriate first-line antibiotic therapy with correct weight-based dosing
- Identify indications for ENT referral and recognise suppurative complications of AOM
INSTRUCTIONS
Acute otitis media is one of the most common infections in childhood and a leading reason for antibiotic prescription in paediatric practice. Understanding when to treat and when to watch is a critical clinical decision that directly impacts antibiotic stewardship. This module will prepare you to diagnose AOM correctly using otoscopy and to manage it rationally according to current IAP and international guidelines.
References
- Ghai Essential Pediatrics, 9th ed., Ch 17 — Diseases of the Ear (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 654 — Otitis Media (textbook)
- IAP Guidelines on Management of Acute Otitis Media in Children (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 10-month-old infant is brought to the outpatient clinic at 10 PM with a high fever of 39.5°C and inconsolable crying since the afternoon. His mother reports he has been tugging at his right ear repeatedly and refused feeds. On examination, he appears irritable and the right tympanic membrane is bright red, bulging, and the light reflex is lost. How do you diagnose and manage this child, and is an antibiotic mandatory at this age?
WHY THIS MATTERS
Acute otitis media is the most common bacterial infection requiring antibiotic treatment in children under five years. In India, AOM contributes significantly to childhood morbidity, hearing impairment, and school absenteeism. Untreated or recurrent AOM can progress to chronic suppurative otitis media (CSOM), mastoiditis, and rarely to intracranial complications such as meningitis or brain abscess. Because AOM is often managed in primary care without specialist input, every final-year student must be able to diagnose it clinically using otoscopy, apply rational antibiotic guidelines, and recognise when watchful waiting is safe versus when immediate treatment is essential.
RECALL
Before proceeding, recall from your Year-1 anatomy studies that the Eustachian (pharyngotympanic) tube connects the middle ear to the nasopharynx. In infants and young children, this tube is shorter (approximately 18 mm vs 35 mm in adults), lies in a more horizontal plane, and has a flaccid, easily compressible cartilaginous support — properties that collectively allow nasopharyngeal secretions and pathogens to ascend into the middle-ear cleft far more readily than in older children or adults. Also recall from microbiology that the nasopharynx is normally colonised by Streptococcus pneumoniae, non-typeable Haemophilus influenzae, and Moraxella catarrhalis — the three principal bacterial causes of AOM. Understanding this anatomy-microbiology link is the foundation of AOM pathogenesis.
Clinical Presentation of AOM
The clinical presentation of acute otitis media varies with age, and recognising this variability prevents both over-diagnosis and missed diagnosis. In infants under 18 months, who cannot verbalise pain, the cardinal features are non-specific: otalgia (earache) manifests as persistent ear-pulling or tugging, inconsolable crying especially at night when supine, and refusal to feed (sucking increases middle-ear pressure and worsens pain). Systemic features include fever (often ≥38.5°C), irritability, and disturbed sleep. Hearing loss may be suspected if the infant fails to respond to sounds but is rarely formally tested acutely. In older children, otalgia is directly reported and is the most reliable symptom; it may be accompanied by a sensation of fullness or muffled hearing. Fever is present in approximately 50–70% of cases but its absence does not exclude AOM.
The definitive diagnosis of AOM requires otoscopy. The three essential otoscopic criteria for AOM are: (1) bulging of the tympanic membrane — the most specific sign, indicating pressure from suppurative middle-ear fluid; (2) erythema (redness) of the tympanic membrane — but note that erythema alone (seen with crying or fever) does not diagnose AOM; and (3) middle-ear effusion — evidenced by loss of the normal light reflex, obscured bony landmarks (handle of malleus, umbo), or visible fluid level/bubbles through the membrane. When the tympanic membrane perforates, otorrhoea (ear discharge) appears and relieves pain — paradoxically, the pain often improves after perforation, but this does not mean the infection has resolved.
Severity classification guides management:
- Severe AOM: otalgia ≥48 h, temperature ≥39°C, bilateral AOM, or otorrhoea
- Non-severe AOM: mild otalgia (<48 h), temperature <39°C, unilateral
Otorrhoea through a perforation or through a tympanostomy tube automatically qualifies as confirmed AOM requiring antibiotics.
IMPORTANT clinical distinction: otitis media with effusion (OME, 'glue ear') presents with a retracted (not bulging) tympanic membrane, absent light reflex, and effusion — but WITHOUT the acute inflammatory signs (erythema, pain, fever). OME is not an infection requiring antibiotics.
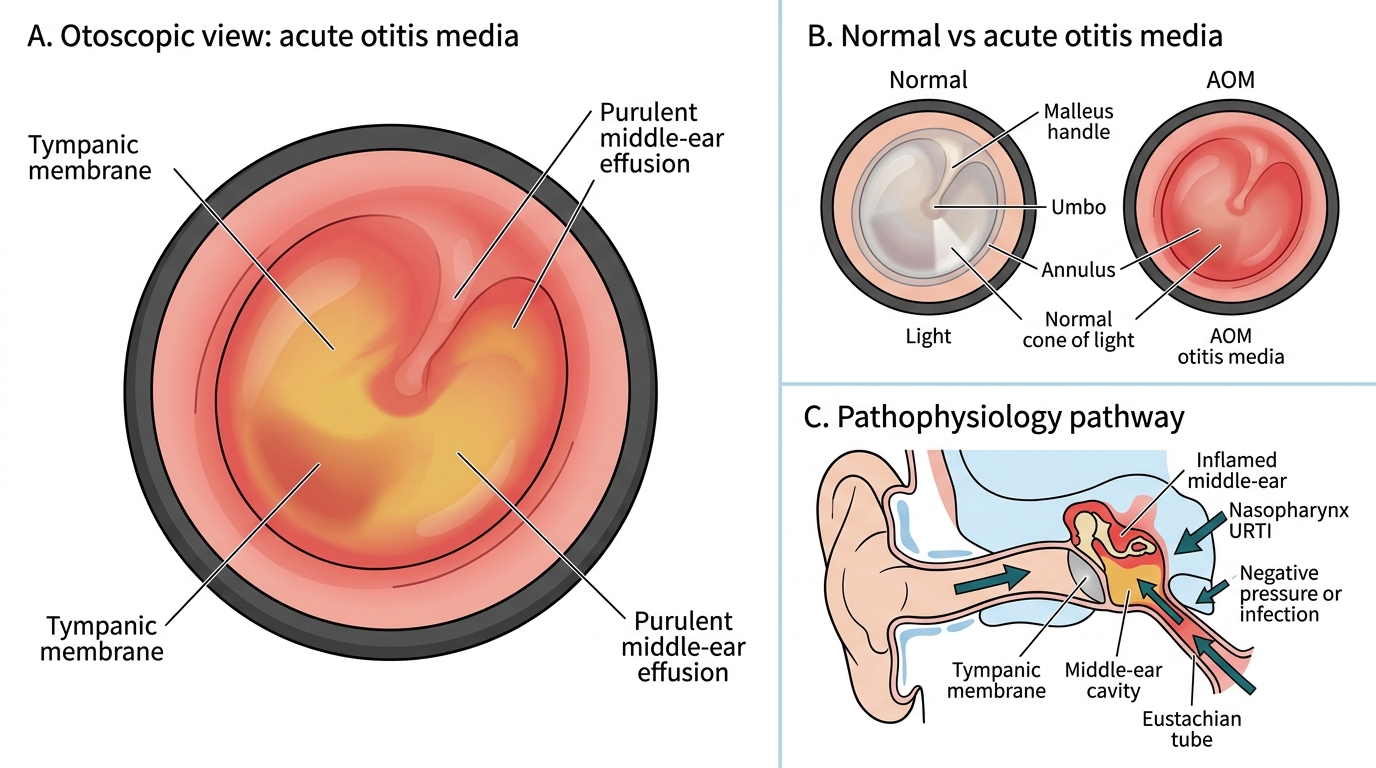
Acute Otitis Media: Otoscopic Appearance and Pathophysiology
Pathophysiology and Aetiology
The pathogenesis of AOM is best understood as a three-stage process: (1) Eustachian tube dysfunction, (2) middle-ear effusion, and (3) bacterial or viral superinfection. This sequence explains why AOM almost invariably follows or accompanies an upper respiratory tract infection (URTI).
During a viral URTI, mucosal oedema and increased secretions compromise Eustachian tube ventilation. The normal function of the Eustachian tube is to equalise middle-ear pressure with atmospheric pressure and to drain middle-ear secretions into the nasopharynx. When tube function fails, a negative middle-ear pressure develops, drawing secretions and nasopharyngeal flora into the middle-ear cleft. The warm, moist, nutrient-rich environment of the middle ear then allows bacterial proliferation, producing a suppurative middle-ear effusion and acute inflammation of the mucosal lining.
Bacterial causes account for approximately 70% of AOM:
- Streptococcus pneumoniae — the single most common bacterial cause (30–40% of cases); most virulent, least likely to resolve spontaneously; main driver of severe and complicated AOM. Serotype coverage by PCV10/PCV13 has reduced pneumococcal AOM but non-vaccine serotypes persist.
- Non-typeable Haemophilus influenzae (NTHi) — second most common (20–30%); causes milder disease, more likely to cause bilateral AOM and OME, and is the principal organism in beta-lactamase-mediated treatment failure.
- Moraxella catarrhalis — third major pathogen (15–20%); most likely to resolve spontaneously (~75% without antibiotics); frequently beta-lactamase positive.
Viral pathogens (respiratory syncytial virus, rhinovirus, adenovirus, parainfluenza, influenza) are identified in approximately 25–40% of AOM, either as sole causative agents or as co-infectors that impair mucosal defence.
Risk factors for AOM include:
- Age <2 years (immature immune system, horizontal Eustachian tube)
- Attendance at daycare (increased exposure to respiratory pathogens)
- Bottle-feeding in supine position (reflux of milk into middle ear)
- Passive smoke exposure (ciliary dysfunction)
- Craniofacial anomalies (e.g., cleft palate — direct Eustachian tube dysfunction)
- Indigenous/disadvantaged populations (higher colonisation rates)
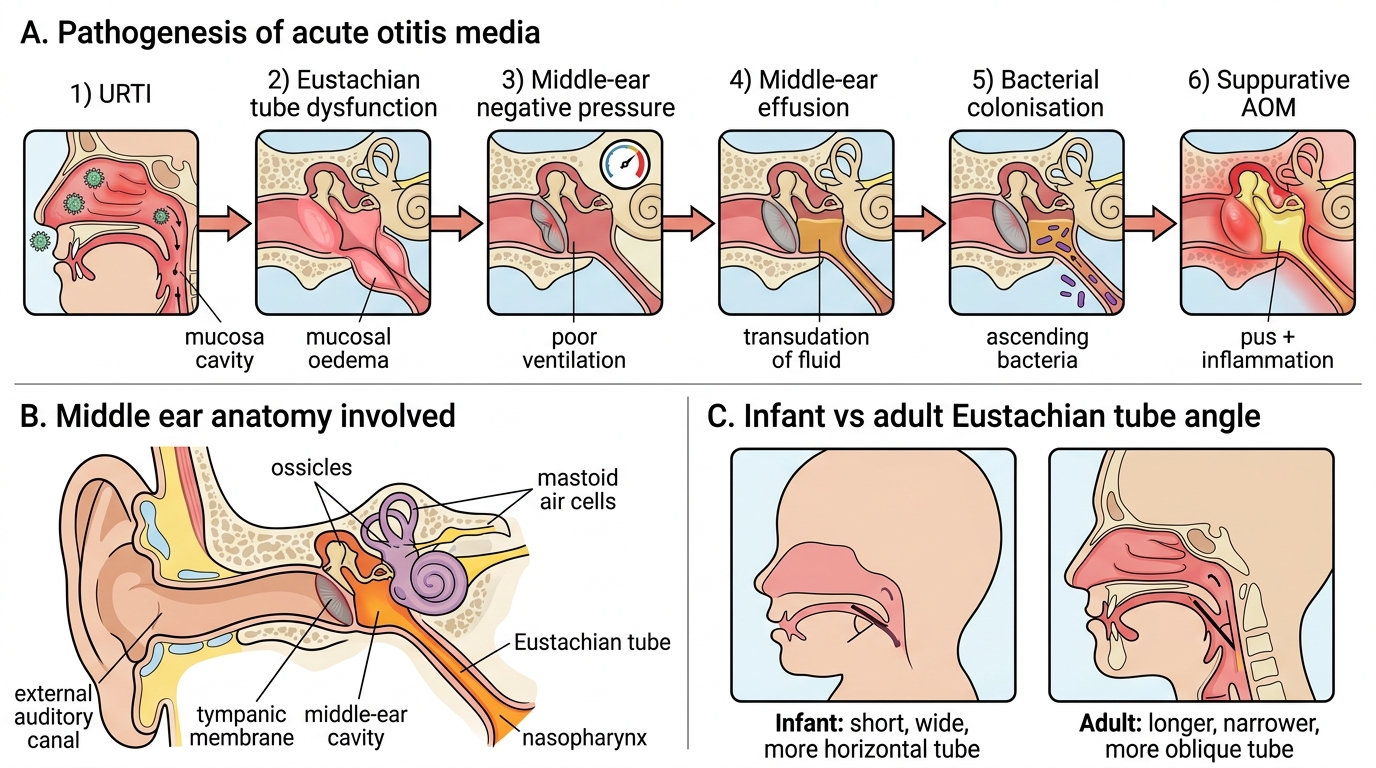
Pathogenesis of Acute Otitis Media
Diagnosis and Investigation
The diagnosis of AOM is primarily clinical, based on the history of acute onset of otalgia and fever combined with otoscopic examination of the tympanic membrane. There are no routine blood tests or imaging required for uncomplicated AOM, and the diagnostic skill every clinician must master is confident interpretation of the tympanic membrane appearance under direct visualisation. The ability to differentiate a bulging, inflamed membrane from a retracted non-infected membrane — and to distinguish both from a normal pearly-grey landmark-preserving membrane — forms the foundation of rational AOM management and antibiotic stewardship. The three criteria that must ALL be simultaneously present for a diagnosis of AOM have been operationalised by both IAP and the American Academy of Pediatrics to ensure that the diagnosis is not made on history alone or on isolated tympanic membrane erythema without effusion. Each criterion plays a different diagnostic role: acute onset establishes temporal relevance, middle-ear effusion confirms the anatomical site of infection, and inflammatory signs confirm that the effusion is not simply a residual glue-ear effusion. This three-part framework should be applied systematically for every child presenting with ear symptoms, especially in infants where the history is indirect and parent-reported. The following diagnostic framework should be applied:
Diagnostic criteria (all three must be met for AOM):
1. Acute onset (within 48 h) of signs and symptoms
2. Presence of middle-ear effusion (shown by: bulging tympanic membrane, limited or absent tympanic membrane mobility on pneumatic otoscopy, otorrhoea, or air-fluid level behind the membrane)
3. Signs and symptoms of middle-ear inflammation (erythema OR marked otalgia)
Pneumatic otoscopy is the gold-standard diagnostic tool: a sealed speculum delivers a puff of air that moves the tympanic membrane. Normal membrane = brisk mobility; AOM = reduced or absent mobility due to the pressure of the effusion; OME = sluggish mobility. Every final-year student must practise this technique.
Tympanometry provides an objective measure of tympanic membrane compliance and middle-ear pressure: a flat (type B) tympanogram confirms middle-ear effusion; negative pressure (type C) suggests Eustachian tube dysfunction without full effusion. Tympanometry is especially useful in young infants where otoscopy is difficult, but it cannot distinguish AOM from OME alone.
Comparison of ear findings (key differential):
| Feature | Normal | AOM | OME (Glue Ear) |
|---|---|---|---|
| Tympanic membrane position | Neutral | Bulging | Retracted |
| Tympanic membrane colour | Pearly grey | Red/yellow | Amber/grey |
| Light reflex | Present (cone of light) | Absent | Absent or distorted |
| Landmarks | Visible (malleus, umbo) | Obscured | Obscured |
| Mobility (pneumatic) | Brisk | Reduced/absent | Reduced |
| Symptoms | None | Otalgia, fever, acute | Hearing loss, no pain |
Microbiological culture (tympanocentesis fluid) is not required for routine AOM but is indicated in: (a) neonates (<28 days) with AOM, (b) immunocompromised children, (c) failure of two antibiotic courses, or (d) suspected suppurative complications. Mastoid imaging (CT) is reserved for suspected mastoiditis — do not routinely order imaging for uncomplicated AOM.
SELF-CHECK
A 14-month-old with 2-day fever and ear-pulling has a bulging, erythematous right tympanic membrane on otoscopy. His temperature is 38°C and he has unilateral AOM with mild irritability. According to IAP/AAP guidelines, what is the most appropriate initial management?
A. Immediate high-dose amoxicillin 80-90 mg/kg/day for 10 days
B. Watchful waiting for 48-72 hours with analgesics, antibiotics only if worsening
C. Amoxicillin-clavulanate as first-line due to likely beta-lactamase resistance
D. Immediate tympanocentesis and culture to guide antibiotic therapy
Reveal Answer
Answer: B. Watchful waiting for 48-72 hours with analgesics, antibiotics only if worsening
This is non-severe, unilateral AOM in a child ≥6 months (temperature <39°C, mild symptoms, unilateral, <48 h of otalgia). IAP and AAP guidelines permit watchful waiting for 48-72 hours in children ≥6 months with non-severe unilateral AOM, provided adequate follow-up is ensured. Analgesics (paracetamol or ibuprofen) are given for pain relief. Antibiotics are started if there is no improvement or worsening at 48-72 hours. Amoxicillin-clavulanate is reserved for treatment failure, not first-line. Tympanocentesis is not routine.