Page 17 of 23
PE25.6 | Lower Respiratory Infection — SDL Guide (Part 2)
Management: Severity-Stratified Treatment
Management of paediatric LRTI is stratified by entity and severity, and the treatment decisions at each tier follow directly from the IMNCI classification. The overarching principle is that the setting of care — home versus hospital — and the route of antibiotic delivery — oral versus intravenous — are determined by the severity classification, not by physician preference or family convenience. This structured approach has been shown to reduce LRTI mortality in resource-limited settings when consistently applied. A critical corollary of this structure is that antibiotic choice in children must always be weight-based — a fixed-dose prescription that ignores a child's weight is a dosing error regardless of the drug chosen. The same principle applies to fluid prescriptions, where the Holliday-Segar formula guides maintenance calculations. Keep this weight-based discipline in mind across every management decision in this section.
BRONCHIOLITIS — supportive care:
Bronchiolitis is a viral illness for which no specific antiviral treatment is routinely available or indicated. Management focuses on:
• Oxygen supplementation — indicated when SpO2 is below 92% on room air; aim SpO2 94–98%
• Hydration — nasogastric tube feeding or IV fluids at maintenance rate (using Holliday-Segar: 100/50/20 mL/kg/day) when oral feeding is inadequate due to tachypnoea
• Nasal suctioning — to clear secretions and improve feeding and breathing
• Monitoring — continuous SpO2 monitoring; watch for apnoea in young infants
• Bronchodilators (salbutamol) — a single trial may be given in older infants and wLRTI; if no objective improvement in work of breathing at 20 minutes, do not continue (IAP recommendation)
• Antibiotics, systemic corticosteroids, and nebulised epinephrine are NOT routinely recommended for uncomplicated viral bronchiolitis
WHEEZE-ASSOCIATED LRTI (wLRTI):
A trial of an inhaled bronchodilator (salbutamol) is appropriate; it may be continued only if there is an objective response. Antibiotic use depends on the presence of features suggesting bacterial co-infection (lobar consolidation on X-ray, marked neutrophilia, high fever).
PNEUMONIA — antibiotic choice by severity:
• Non-severe pneumonia (fast breathing, no indrawing, no danger signs): Oral amoxicillin 40 mg/kg/day in 3 divided doses for 5 days — weight-based dosing is mandatory. The child is discharged with instructions to return immediately if breathing worsens, cannot feed, or develops chest indrawing. Cotrimoxazole is no longer recommended as first-line in India due to high pneumococcal resistance.
• Severe pneumonia (chest indrawing): Admit to hospital. IV ampicillin 50 mg/kg/dose 6-hourly (or benzyl penicillin 50,000 U/kg/dose 6-hourly) PLUS IV gentamicin 7.5 mg/kg/day once daily. Step down to oral amoxicillin when the child tolerates oral feeds and fever resolves for 48 hours. Supplemental oxygen as needed.
• Very severe pneumonia (danger signs): Parenteral amoxicillin-clavulanate or ceftriaxone (for possible resistant organisms); oxygen; emergency referral if not improving.
EMPYEMA:
Hospital management with IV antibiotics covering S. aureus (cloxacillin 50 mg/kg/dose 6-hourly) and S. pneumoniae; pleural fluid drainage by needle aspiration (if small, free-flowing) or intercostal chest-tube drainage (if large or loculated). If fibrinopurulent, intrapleural fibrinolytics (urokinase) may be used. Decortication is reserved for organised empyema with trapped lung that fails conservative management.
PREVENTION: The pneumococcal conjugate vaccine (PCV13) and Hib vaccine (both in India's Universal Immunization Programme) are the most important preventive interventions. Additional measures include promotion of exclusive breastfeeding for 6 months, treatment of maternal and household tobacco smoking and indoor air pollution, and adequate nutrition.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
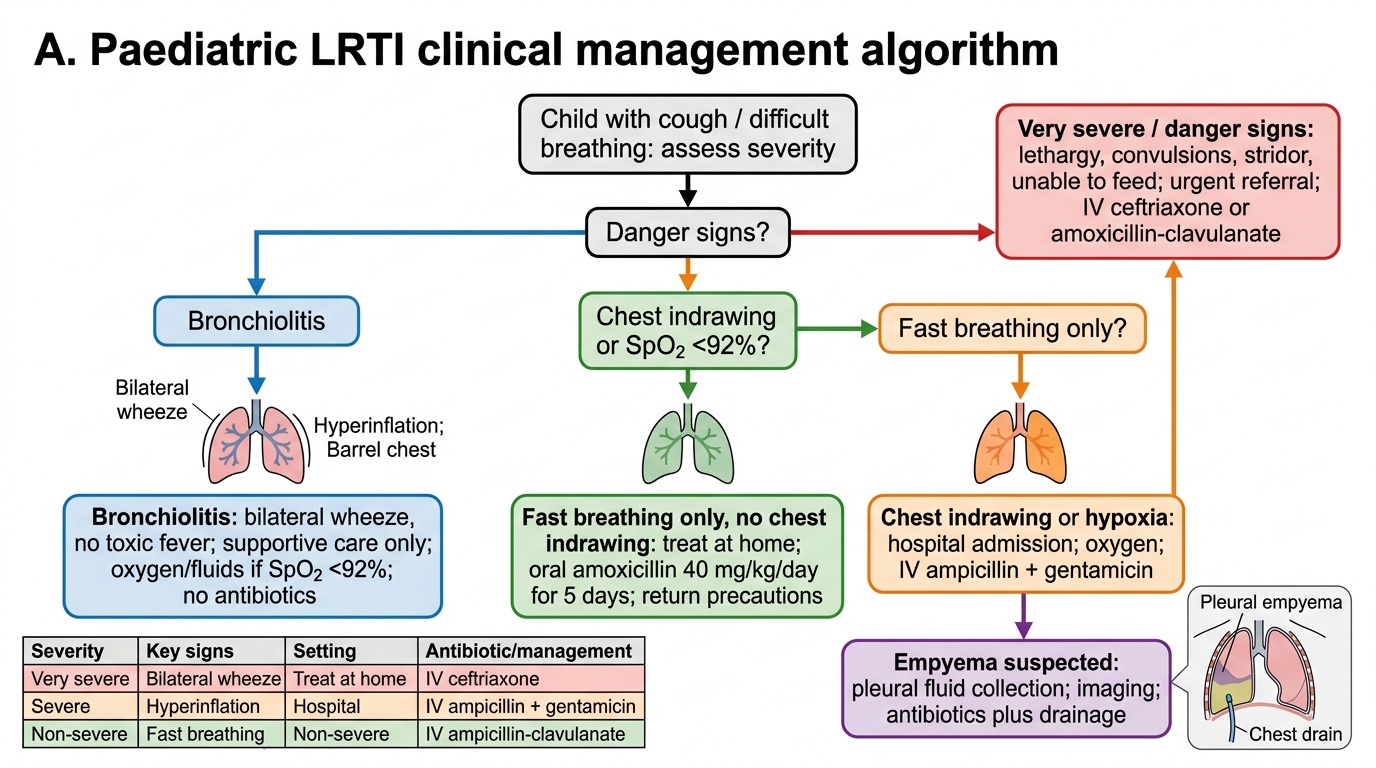
Paediatric LRTI Severity-Based Management Algorithm
| Severity | Key Signs | Setting | Antibiotic |
|---|---|---|---|
| Non-severe pneumonia | Fast breathing only, no indrawing | Home | Oral amoxicillin 40 mg/kg/day × 5d |
| Severe pneumonia | Chest indrawing | Hospital admission | IV ampicillin + gentamicin |
| Very severe / danger signs | Lethargy, convulsions, stridor, unable to feed | Urgent referral | IV ceftriaxone/amoxicillin-clavulanate |
| Bronchiolitis | Bilateral wheeze, barrel chest, no fever/toxic | Hospital if SpO2 <92% | Supportive only — no antibiotics |
| Empyema | Dullness, absent BS, unresponsive fever | Hospital | IV cloxacillin + drainage |
SELF-CHECK
A 2.5-year-old child presents with fever, cough, and breathing rate of 42 per minute. There is no chest indrawing. Auscultation reveals decreased breath sounds over the right lower zone with dullness to percussion. There are no danger signs. What is the IMNCI classification and what investigation is most important next?
A. Non-severe pneumonia — discharge with oral amoxicillin; no investigation needed
B. Severe pneumonia — admit and start IV ampicillin; chest X-ray to assess for empyema
C. Non-severe pneumonia — chest X-ray and ultrasound to rule out parapneumonic collection before deciding setting of care
D. Bronchiolitis — salbutamol trial and supportive care
Reveal Answer
Answer: B. Severe pneumonia — admit and start IV ampicillin; chest X-ray to assess for empyema
A respiratory rate of 42/min in a 1–5 year old meets the IMNCI threshold (≥40/min = fast breathing for this age). However, the finding of dullness to percussion and decreased breath sounds suggests a parapneumonic effusion or evolving empyema — a significant complication that upgrades the severity. While the IMNCI classification initially shows severe pneumonia (fast breathing + possible consolidation), the physical signs of a pleural collection require admission. A chest X-ray is essential to assess consolidation extent and any pleural collection; ultrasound confirms and localises effusion. Starting IV ampicillin covers the most likely pathogen (S. pneumoniae). Option A is incorrect because the physical signs of a pleural collection demand admission and investigation, not home treatment.
Self-Assessment
Use these structured questions to consolidate your understanding of the LRTI spectrum, IMNCI classification, and management principles before proceeding to the formal assessments. The most frequently examined points are the age-specific fast-breathing thresholds, the definition of chest indrawing, and the distinction between supportive bronchiolitis management and antibiotic-based pneumonia treatment. Attempt each question from memory before reviewing your notes, paying particular attention to the age-specificity of the IMNCI thresholds — a threshold off by even 10 breaths per minute represents a different severity tier and a different clinical decision. If you find that you are uncertain about a threshold, return to the IMNCI section and memorise it explicitly; these numbers are too important to leave approximate. Precision with these thresholds is not pedantry — it is the difference between safe and unsafe clinical practice.
Aetiology and pathophysiology:
• Name the single most common viral cause of bronchiolitis, and explain its pathophysiological mechanism of air-trapping.
• Why is Streptococcus pneumoniae the most important bacterial target for the pneumococcal vaccine in children?
• Describe the three pathological stages of empyema progression and explain why stage affects management difficulty.
IMNCI classification:
• Without looking at your notes, state the fast-breathing respiratory rate threshold for: a 1-month-old, a 9-month-old, and a 3-year-old.
• What is the definition of chest indrawing and why does it indicate severe (rather than non-severe) pneumonia?
• List four IMNCI general danger signs that require urgent referral.
Management:
• A 10-month-old with bronchiolitis has SpO2 88%. Describe your immediate management steps.
• What is the weight-based amoxicillin dose for non-severe pneumonia, and what is the duration of treatment?
• When should you suspect empyema in a child already admitted with pneumonia, and what drainage modality is appropriate in the exudative stage?