Page 7 of 34
PE26.3 | Vitamin B12 Folate Deficiency Anaemia — SDL Guide
Learning Objectives
- Describe the pathophysiology of megaloblastic anaemia, explaining why B12 and folate deficiency produce identical haematological but different clinical pictures
- Identify the common causes of B12 and folate deficiency in Indian children, with emphasis on dietary and maternal risk factors
- Recognise the clinical features of megaloblastic anaemia including the neurological manifestations unique to B12 deficiency
- Interpret CBC, peripheral blood smear (macro-ovalocytes, hypersegmented neutrophils), and specific assays (serum B12, red cell folate) to confirm and distinguish the two deficiencies
- Apply the B12-before-folate treatment rule, prescribe appropriate therapy, and counsel on dietary sources of both vitamins
INSTRUCTIONS
Vitamin B12 and folate deficiency produce an identical haematological picture — macrocytic megaloblastic anaemia — but only B12 deficiency adds neurological damage. This distinction is clinically crucial because treating with folate alone in a B12-deficient child corrects the blood count while the nervous system continues to deteriorate. In India, B12 deficiency is predominantly nutritional: strictly vegetarian (especially vegan) mothers produce B12-depleted breast milk, and their exclusively breastfed infants develop deficiency in the first year of life, often with developmental regression as the first sign. This module builds the metabolic and clinical reasoning framework to diagnose and safely treat megaloblastic anaemia in paediatric practice.
References
- Ghai Essential Pediatrics, 9th ed, Ch 17 (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 484 (textbook)
- IAP Recommended Immunization Schedule and Guidelines, 2023 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
An 8-month-old infant is brought to the paediatric OPD with a 6-week history of progressive lethargy, poor feeding, and loss of milestones — he had started sitting without support at 7 months but now cannot do so. His mother is a strict lacto-vegetarian who has been exclusively breastfeeding since birth. On examination: pallor, mild jaundice, markedly hypotonic ('floppy infant'), and absent deep tendon reflexes. CBC: Hb 7.0 g/dL, MCV 112 fL, WBC normal, platelets normal. Peripheral smear: large oval red cells and one neutrophil with 7 nuclear lobes. You recognise this as megaloblastic anaemia. What causes it? How do you confirm whether this is B12 or folate deficiency? And critically — why does the order in which you prescribe treatment matter so much?
WHY THIS MATTERS
Megaloblastic anaemia due to B12 deficiency is the most important and potentially most dangerous nutritional anaemia in Indian infants because it combines a correctable haematological picture with a partially irreversible neurological injury. The neurological damage — subacute combined degeneration of the spinal cord — progresses silently while the anaemia is the visible problem, and if folate is administered first (correcting the CBC) while B12 deficiency is untreated, the nervous system continues to deteriorate even as the blood count normalises. In India, the strict vegetarian tradition — with little or no dairy, eggs, meat, or fish — means that maternal B12 stores are often marginal, and exclusively breastfed infants of such mothers are at high risk in the first year of life. Understanding this condition prevents the dangerous clinical error of treating megaloblastic anaemia blindly with folate.
RECALL
Review these foundations before proceeding:
• DNA synthesis pathway: both vitamin B12 (cobalamin) and folate (as 5,10-methylenetetrahydrofolate) are required for thymidylate synthesis — the conversion of deoxyuridine monophosphate (dUMP) to deoxythymidine monophosphate (dTMP), which is essential for DNA replication. When either vitamin is deficient, DNA synthesis slows while cytoplasmic RNA and protein synthesis continue normally — producing large cells with immature nuclei relative to their cytoplasm (megaloblasts).
• B12-specific pathway (not shared with folate): methylcobalamin is the cofactor for methionine synthase (homocysteine → methionine). Adenosylcobalamin is the cofactor for methylmalonyl-CoA mutase (methylmalonyl-CoA → succinyl-CoA). Deficiency of the latter leads to toxic accumulation of methylmalonyl-CoA, which disrupts myelin synthesis — the mechanism of neurological injury in B12 deficiency. Folate cannot substitute for adenosylcobalamin, which is why folate therapy does not prevent or reverse the neurological damage of B12 deficiency.
• MCV >100 fL = macrocytic anaemia; the previous SDL established the three-category MCV framework — this SDL covers the macrocytic branch.
Clinical Presentation: The Macrocytic Anaemic Child
The clinical presentation of megaloblastic anaemia in children reflects the combined effects of anaemia and, in B12 deficiency, neurological dysfunction. Because megaloblastic anaemia develops slowly, children adapt remarkably well to falling haemoglobin, and many are not brought for evaluation until the anaemia is severe or the neurological features become alarming.
Provided image
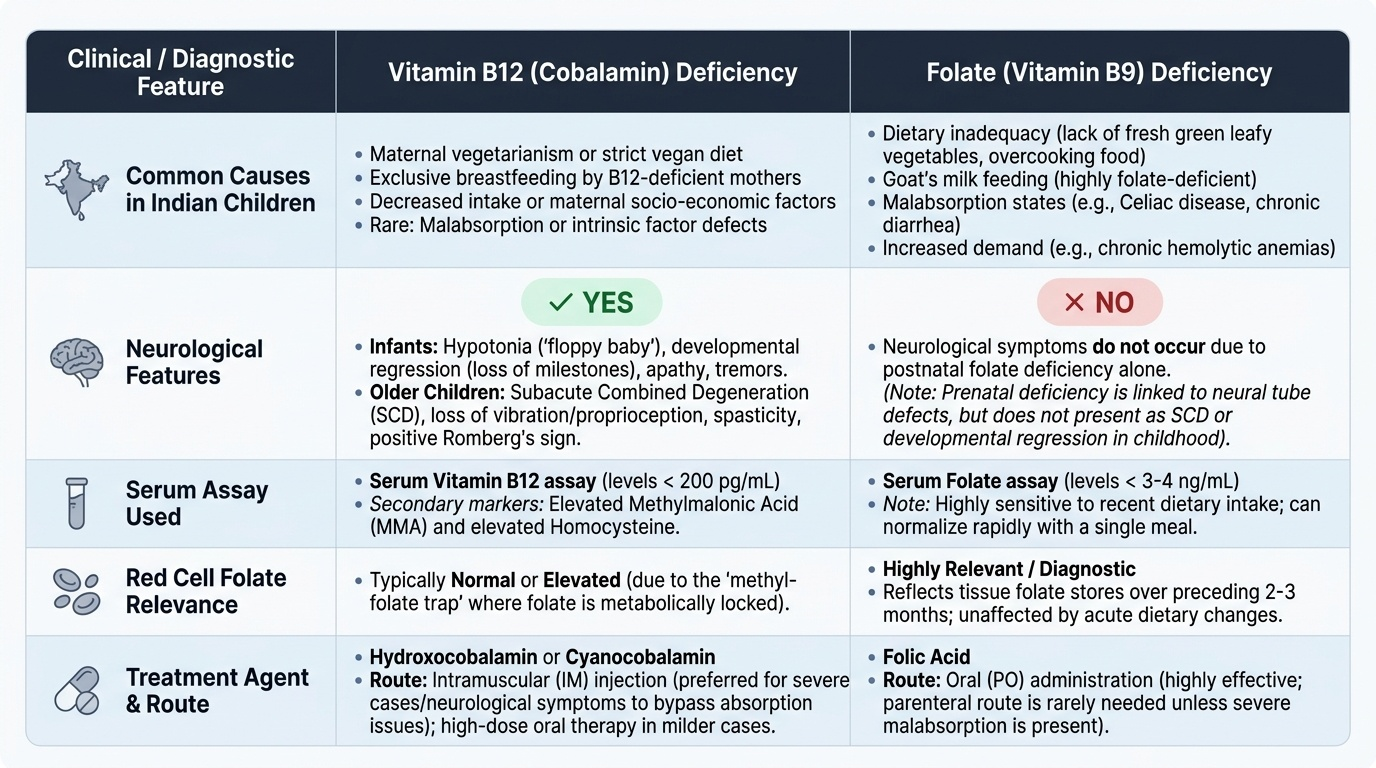
The haematological symptoms and signs are identical regardless of whether B12 or folate is the deficient vitamin: pallor (typically more severe than in IDA because macrocytic anaemia can reach very low haemoglobin levels before compensation fails), fatigue, irritability, anorexia, and failure to thrive. In severe cases, tachycardia, flow murmur, and signs of high-output cardiac failure occur as in any severe anaemia. A distinctive feature on examination is mild jaundice — not from liver disease but from intramedullary haemolysis (ineffective erythropoiesis causes premature destruction of megaloblastic precursors within the bone marrow, releasing unconjugated bilirubin). The combination of pallor and mild jaundice in a macrocytic anaemia should immediately prompt consideration of megaloblastic disease.
The neurological features unique to B12 deficiency (absent in folate deficiency) are among the most clinically important findings:
• In infants: hypotonia (floppy baby), developmental regression (loss of previously attained milestones), poor interaction, absent or reduced deep tendon reflexes, irritability
• In older children: posterior column signs — loss of vibration sense and proprioception, broad-based gait, Romberg's sign positive; corticospinal signs — upper motor neurone pattern with spasticity and brisk reflexes in established cases; subacute combined degeneration (SCD) is the term for involvement of both the dorsal columns and the lateral corticospinal tracts
• Neuropsychiatric: irritability, mood changes, cognitive regression
In Indian infants, developmental regression is often the presenting complaint — the parents report that a child who had been developing normally has stopped making progress or lost skills. This should immediately raise the possibility of B12 deficiency in a breastfed infant of a vegetarian mother, even before the blood count is reviewed.
Pathophysiology: Why B12 and Folate Deficiency Produce the Same Blood Picture but Different Complications
The haematological similarity between B12 and folate deficiency arises from their shared role in DNA synthesis, while the neurological distinction arises from a B12-specific metabolic pathway that folate cannot substitute for. Understanding these two separate mechanisms is the key to understanding why the treatment sequence matters so much clinically.
Shared mechanism — impaired DNA synthesis and megaloblastic haematopoiesis: both B12 and folate are required for the synthesis of thymidine monophosphate (dTMP) from deoxyuridine monophosphate (dUMP). Folate, in its active form 5,10-methylenetetrahydrofolate (5,10-MTHF), provides the methylene group for this reaction. Vitamin B12 is required to release folate from its stored form (5-methylTHF) by accepting the methyl group — converting it to methyl-B12, which then donates the methyl group to homocysteine to regenerate methionine. When B12 is absent, folate becomes trapped as 5-methylTHF (the 'methylfolate trap'), and even an adequate folate intake cannot be converted to the active 5,10-MTHF needed for DNA synthesis. Thus B12 deficiency causes a functional folate deficiency even when folate stores are adequate. The resulting slowing of DNA replication produces megaloblasts — large, abnormally shaped erythroid and myeloid precursors with nuclear-cytoplasmic asynchrony (large, immature-looking nucleus relative to abundant cytoplasm). These megaloblasts are inefficiently destroyed in the bone marrow (ineffective erythropoiesis) rather than completing maturation, leading to jaundice and, paradoxically, low reticulocytes despite active marrow activity.
B12-specific mechanism — myelin toxicity: adenosylcobalamin is the cofactor for methylmalonyl-CoA mutase, which converts methylmalonyl-CoA to succinyl-CoA in the Krebs cycle. When B12 is deficient, methylmalonyl-CoA accumulates. Methylmalonyl-CoA is a structural mimic of malonyl-CoA and is inappropriately incorporated into fatty acid synthesis, producing abnormal odd-chain fatty acids that disrupt myelin sheath integrity. This is the mechanism of subacute combined degeneration of the spinal cord — an irreversible process unless treated early. Folate supplementation corrects the haematological picture but does not address this pathway — hence the critical rule: confirm B12 status and treat B12 deficiency before or alongside folate.
Common causes of B12 deficiency in Indian children:
• Nutritional (dietary) — most common: strictly vegetarian or vegan mothers producing B12-deficient breast milk; exclusively breastfed infants of such mothers develop clinical deficiency by 4–12 months; older children on strict vegetarian diets
• Malabsorption: Crohn's disease, small bowel bacterial overgrowth, surgical resection of terminal ileum (the site of B12-intrinsic factor complex absorption), fish tapeworm (Diphyllobothrium — rare in India)
• Inherited: intrinsic factor deficiency (congenital or autoimmune — juvenile pernicious anaemia, rare in children), transcobalamin II deficiency
Common causes of folate deficiency in Indian children:
• Goat's milk — important paediatric cause: goat's milk is markedly folate-deficient; infants fed exclusively on goat's milk develop megaloblastic anaemia of infancy (folate deficiency type)
• Increased demand: haemolytic anaemias (thalassaemia, sickle cell, G6PD) — high red cell turnover rapidly depletes folate stores; pregnancy in adolescents
• Malabsorption: coeliac disease, tropical sprue, Crohn's disease, antiepileptic drugs (phenytoin, valproate — inhibit folate absorption/metabolism)
• Dietary inadequacy: in severely malnourished children; during parenteral nutrition without folate supplementation
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
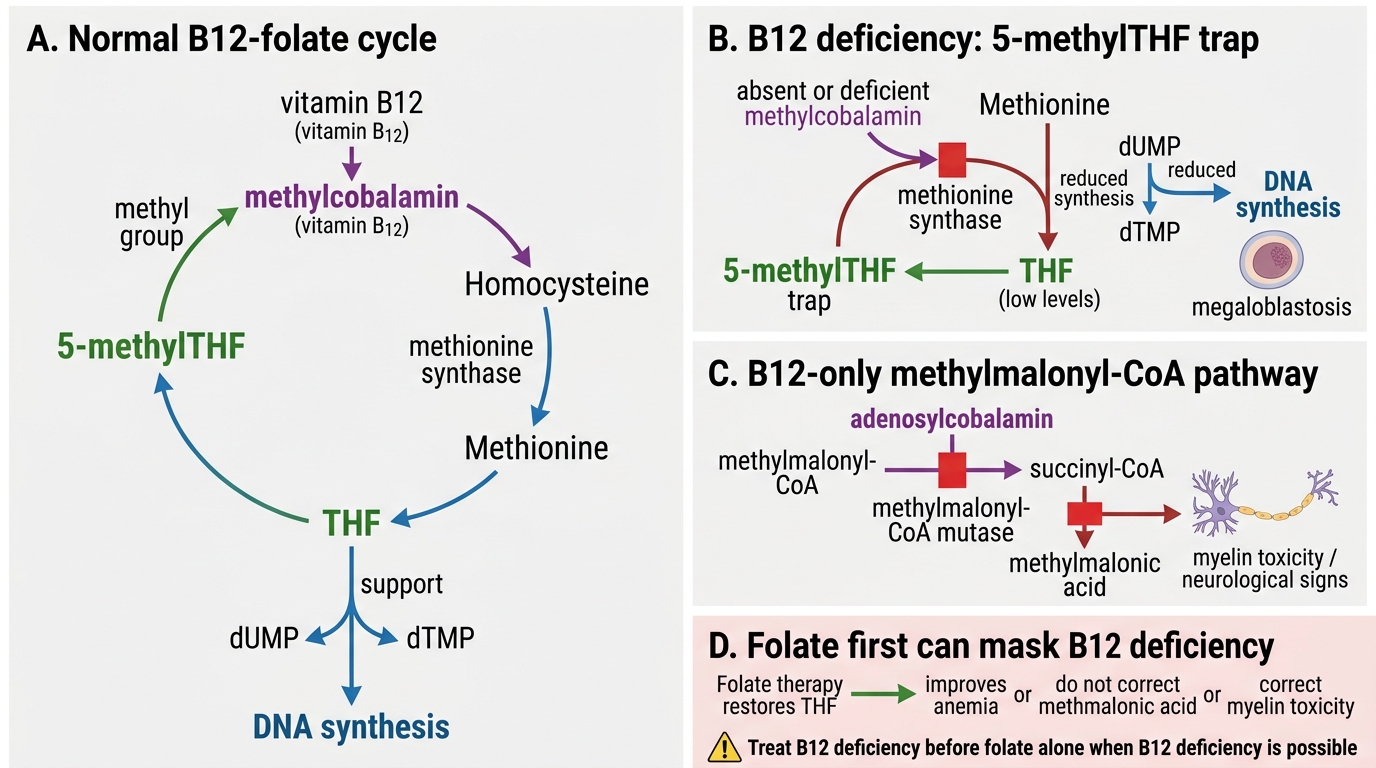
Vitamin B12-Folate Interaction in DNA Synthesis and Neurological Disease
SELF-CHECK
A 10-month-old breastfed infant of a strictly vegetarian mother presents with macrocytic anaemia and developmental regression. Which investigation finding would MOST specifically confirm vitamin B12 deficiency (rather than folate deficiency) as the cause?
A. MCV >100 fL on CBC
B. Hypersegmented neutrophils on peripheral smear
C. Low serum B12 (<200 pg/mL) with elevated serum methylmalonic acid
D. Macro-ovalocytes on peripheral smear
Reveal Answer
Answer: C. Low serum B12 (<200 pg/mL) with elevated serum methylmalonic acid
MCV >100 fL and hypersegmented neutrophils confirm megaloblastic anaemia but do NOT distinguish B12 from folate deficiency — both produce these findings. Macro-ovalocytes similarly occur in both. A low serum B12 combined with elevated methylmalonic acid (MMA) is B12-specific: MMA accumulates when adenosylcobalamin-dependent methylmalonyl-CoA mutase is impaired — a pathway unique to B12. Elevated homocysteine occurs in both B12 and folate deficiency. Elevated MMA with normal homocysteine and normal folate clinches B12 deficiency.
Investigations: Confirming and Distinguishing B12 from Folate Deficiency
The investigation of suspected megaloblastic anaemia follows a stepwise approach: first confirm the macrocytic megaloblastic picture from the CBC and smear, then use specific assays to determine whether the cause is B12 deficiency, folate deficiency, or both. This distinction cannot be made clinically or from the CBC alone — specific vitamin assays are mandatory before treatment begins, because the treatment sequence depends entirely on which vitamin is deficient. Ordering both serum B12 and red cell folate at the same time is strongly recommended rather than sequentially, because the results together determine whether to treat B12 alone, folate alone, or both concurrently. Deferring the specific assay until after an empirical folate course has been given is a clinical error that can mask B12 deficiency while neurological deterioration continues.
Provided image
CBC findings in megaloblastic anaemia:
• MCV >100 fL (macrocytosis), often markedly elevated (120–140 fL in severe deficiency)
• Haemoglobin reduced — may be severely low (4–6 g/dL) because disease develops slowly and compensation continues until late
• Pancytopenia in severe cases — not just anaemia but also leucopenia and thrombocytopenia, because megaloblastic changes affect all marrow cell lines
• Reticulocyte count is low-normal or reduced despite severe anaemia — reflecting ineffective erythropoiesis (marrow activity is high but output is low due to intramedullary destruction)
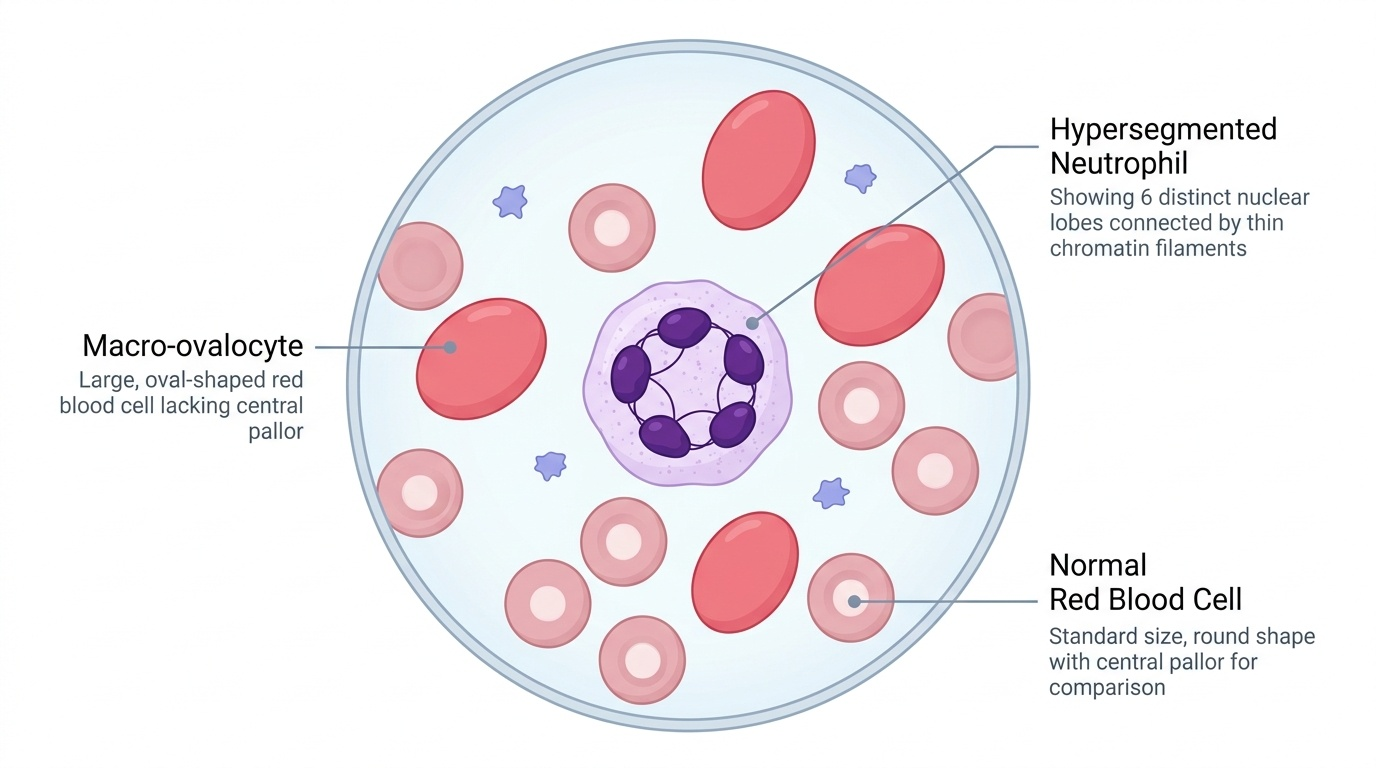
Peripheral blood smear — the diagnostic cornerstone:
• Macro-ovalocytes (macro-oval cells): large, oval-shaped RBCs with no central pallor, distinct from the round macrocytes of liver disease; their presence on smear is highly specific for megaloblastic haematopoiesis
• Hypersegmented neutrophils (HSN): neutrophils with ≥5 nuclear lobes, or any neutrophil with ≥6 lobes; even a single 6-lobed neutrophil is diagnostic; this finding precedes the anaemia and is the most sensitive early indicator of megaloblastic change
• Anisocytosis and poikilocytosis; teardrop cells; nucleated RBCs in severe cases
Specific assays:
• Serum B12 (cobalamin): <200 pg/mL = deficient; 200–300 pg/mL = borderline; >300 pg/mL = normal. Serum B12 can be falsely normal in early deficiency — elevated serum homocysteine and methylmalonic acid (MMA) are more sensitive functional markers
• Serum methylmalonic acid (MMA): elevated specifically in B12 deficiency (adenosylcobalamin pathway); normal in folate deficiency — the most specific B12 marker available
• Red cell folate: the preferred measure of folate stores (more stable than serum folate, which reflects recent intake); <150 ng/mL = depleted
• Serum homocysteine: elevated in both B12 and folate deficiency (both required for homocysteine → methionine conversion); not specific for either
| Parameter | B12 Deficiency | Folate Deficiency | Both |
|---|---|---|---|
| MCV | ↑↑ | ↑↑ | ↑↑ |
| Hyperseg. neutrophils | Present | Present | Present |
| Serum B12 | ↓ | Normal | ↓ |
| Red cell folate | Low (functional trap) or normal | ↓ | ↓ |
| Serum MMA | ↑↑ | Normal | ↑↑ |
| Serum homocysteine | ↑ | ↑ | ↑↑ |
| Neurological signs | Present | Absent | Present |
CLINICAL PEARL
Hypersegmented neutrophils (HSN) are the earliest and most sensitive indicator of megaloblastic change — they appear in the peripheral blood 2–4 weeks before the MCV rises above 100 fL and 4–6 weeks before haemoglobin falls. In any child with suspected B12 or folate deficiency, deliberately scan the smear for neutrophil lobe counts before concluding the CBC is 'normal macrocytosis'. A single neutrophil with 6 or more lobes is diagnostic of megaloblastic change.