Page 31 of 48
PE27.10 | Cerebral Palsy — SDL Guide
Learning Objectives
- Define cerebral palsy and recognise its core clinical features — non-progressive motor disorder with onset in the developing brain
- Classify cerebral palsy by motor type (spastic, dyskinetic, ataxic, mixed) and functional severity using the GMFCS
- Identify the common prenatal, perinatal, and postnatal causes of cerebral palsy with emphasis on birth asphyxia
- List the common comorbidities of CP including epilepsy, intellectual disability, and sensory impairments
- Outline the multidisciplinary management approach including physiotherapy, spasticity management, and family counselling
INSTRUCTIONS
Cerebral palsy (CP) is the most common cause of physical disability in childhood, affecting approximately 2–3 per 1,000 live births globally. In India, birth asphyxia and perinatal infections remain predominant causes in a setting where neonatal care is still being scaled up. Understanding CP is essential not only for the neurologist or physiatrist, but for every clinician who cares for children — because early recognition, accurate functional assessment using the GMFCS, appropriate referral for therapy, and management of life-altering comorbidities such as epilepsy and feeding difficulties all fall within general paediatric practice. This module equips you with a systematic framework for diagnosis, classification, and MDT-coordinated management.
References
- Ghai Essential Pediatrics, 9th Edition, Ch. 18 (Developmental Paediatrics) (textbook)
- Nelson Textbook of Pediatrics, 21st Edition, Ch. 616 (Cerebral Palsy) (textbook)
- IAP Guidelines on Cerebral Palsy Management (guideline)
- Rosenbaum P et al. A report: the definition and classification of cerebral palsy, Dev Med Child Neurol 2007 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Shreya is an 18-month-old girl brought by her parents for 'not walking yet.' Her birth history reveals she was born at term after a prolonged and difficult delivery with a poor APGAR score (APGAR 3 at 1 minute, 6 at 5 minutes), and she required bag-and-mask ventilation in the delivery room. Her parents were told she had 'birth-related brain injury.' Now at 18 months, she pulls to stand only with significant support and cannot walk. On examination, she is alert, makes eye contact, and babbles with a few words. Neurological examination reveals increased tone in both lower limbs, brisk knee jerks bilaterally, bilateral Babinski responses, and scissoring of the legs when held upright. Her upper limbs are less affected. The paediatrician suspects cerebral palsy. How would you classify her CP, and what is your management plan?
WHY THIS MATTERS
Cerebral palsy is the most common cause of childhood physical disability, with an estimated prevalence of 2–3 per 1,000 live births worldwide and potentially higher in India given the burden of preventable perinatal causes. As a practising clinician you will encounter children with CP in general outpatient clinics, inpatient wards, and community health settings. Your responsibilities include: recognising the condition early (before the family attributes persistent motor delay to 'slow development'), classifying it accurately to guide prognosis and therapy goals, identifying and managing life-altering comorbidities (epilepsy occurs in up to 35–40%, intellectual disability in ~50%), coordinating a multidisciplinary therapy team, and counselling parents about realistic expectations and available support. Understanding CP also has public health significance — the majority of Indian cases are preventable through better intrapartum care, neonatal resuscitation training, and reduction of kernicterus.
RECALL
Activate your prior knowledge before engaging with this module:
• Upper motor neuron (UMN) signs: spasticity (velocity-dependent increase in tone), brisk deep tendon reflexes, Babinski (extensor plantar response), clonus. These arise from lesions in the motor cortex or corticospinal tract.
• Lower motor neuron (LMN) signs: flaccidity, reduced/absent reflexes, fasciculations, muscle atrophy. CP is a UMN disorder (in spastic types).
• Developmental milestones: walking alone normally by 12–15 months; persistent inability to walk by 18 months warrants investigation.
• Primitive reflexes: Moro, asymmetric tonic neck reflex (ATNR), grasp — normally disappear by 4–6 months; persistence suggests CNS dysfunction.
• HIE and Sarnat classification: Grade I (mild — irritability, hyperalertness, resolves within 24 h), Grade II (moderate — seizures, tone abnormalities), Grade III (severe — coma, absent brainstem reflexes); Grade II–III HIE is the most important cause of CP in India.
• Neurodevelopmental principle: the brain lesion causing CP is STATIC (non-progressive), even though the clinical picture may evolve as the child grows and spasticity changes.
Clinical Presentation: Recognising Cerebral Palsy
Cerebral palsy (CP) is defined as a group of permanent, non-progressive disorders of movement and posture development, attributed to non-progressive disturbances that occurred in the developing fetal or infant brain. The emphasis on 'non-progressive' is diagnostic — the underlying brain lesion does not advance, though the clinical manifestations may change as the child grows (muscle contractures develop, motor demands increase, comorbidities become apparent). CP presents as a primary motor disorder, but the brain lesion frequently also affects cognition, communication, sensation, and behaviour.
Provided image
The most common clinical presentation bringing a child to attention is global developmental delay — particularly delayed achievement of motor milestones — sometimes accompanied by abnormal tone or movements noticed by parents or a health worker. The paediatrician must maintain a high index of suspicion in any child with a history of perinatal risk factors (birth asphyxia, prematurity, neonatal jaundice, meningitis) combined with motor delay or abnormal neurological findings.
Key early clinical features (suggestive of CP in infancy):
• Persistence of primitive reflexes beyond the expected age (ATNR beyond 6 months, Moro beyond 5 months).
• Abnormal tone — generalised hypotonia initially ('floppy infant'), evolving to hypertonia in spastic types as myelination proceeds.
• Asymmetry of movement or hand preference before 12 months (suggests hemiplegia — normal children are not hand-preferent before 1 year).
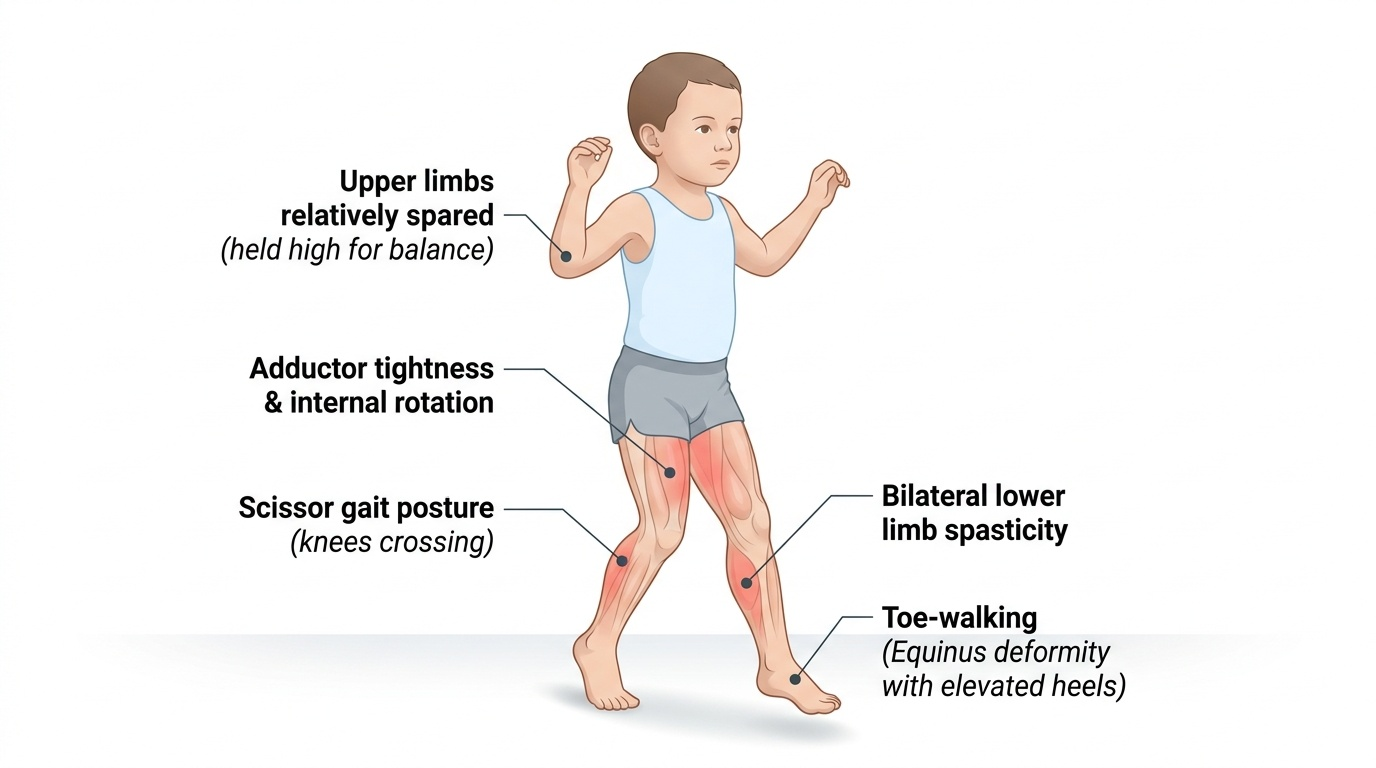
• Delayed or absent walking; scissoring of legs when held upright (adductor spasticity).
• Persistent fisting of hands beyond 3 months, abnormal thumb position.
• Feeding difficulties — poor suck, aspiration risk (bulbar involvement).
CP subtypes by presenting motor pattern:
Spastic CP (70–80% of all CP): The most common type, arising from damage to the motor cortex or corticospinal tract. Characterised by increased tone (velocity-dependent), brisk reflexes, Babinski response, and clonus. Subtypes by limb distribution: Spastic hemiplegia (one side of body; arm often more than leg; early hand preference; may not present until child attempts to reach or walk) → Spastic diplegia (both legs mainly, arms less affected; typical of prematurity/PVL; scissors gait) → Spastic quadriplegia (all four limbs severely affected; most often from severe global HIE or major structural malformation; highest comorbidity burden).
Dyskinetic CP (~10–15%): Damage primarily to the basal ganglia; presents with involuntary movements — choreoathetosis (writhing, purposeless movements that worsen with voluntary action) or dystonia (sustained abnormal postures). A classic cause is kernicterus (unconjugated bilirubin toxicity to the basal ganglia in the neonatal period), which classically produces a triad: choreoathetoid CP, high-frequency sensorineural hearing loss, and upward gaze palsy. Children with dyskinetic CP may have near-normal intelligence despite severe motor disability.
Ataxic CP (~5%): Damage to the cerebellum; characterised by hypotonia, intention tremor, dysmetria, and wide-based ataxic gait. Often a genetic or prenatal cause.
Mixed CP: Features of more than one type, most commonly spastic + dyskinetic.
Pathophysiology and Aetiology
The pathophysiology of CP is defined by a static, non-progressive brain lesion occurring during the period of active brain development — a window that extends from early fetal life through the first 2–3 years of postnatal life. The nature and location of the brain lesion determines the motor type of CP: cortical and subcortical white matter injury causes spastic CP, basal ganglia damage produces dyskinetic CP, and cerebellar insults lead to ataxic CP. Understanding the timing and mechanism of the insult enables the clinician to identify the cause, counsel about recurrence risk, and sometimes implement prevention strategies.
Prenatal causes:
Brain malformations (cortical dysplasia, lissencephaly, pachygyria, schizencephaly) result from disruption of neuronal proliferation and migration during the first and second trimesters. Congenital infections (TORCH — toxoplasmosis, rubella, CMV, herpes) can cause periventricular calcification, cortical damage, and subsequent CP. Prenatal stroke (arterial or venous) causes focal lesions that manifest as hemiplegia. Genetic mutations affecting brain structural development account for a significant proportion of CP in term infants without identifiable perinatal asphyxia.
Perinatal causes (most common in India):
Hypoxic-ischaemic encephalopathy (HIE): The leading cause of CP in term infants in low-resource settings. Intrapartum asphyxia leads to failure of oxidative phosphorylation → neuronal energy failure → excitotoxic glutamate release → neuronal necrosis. The anatomical pattern of injury depends on severity: moderate HIE preferentially affects the parasagittal (watershed) cortex → spastic quadriplegia or diplegia; severe HIE damages the basal ganglia and thalami → dyskinetic CP, as well as deep grey matter structures.
Periventricular leukomalacia (PVL): The predominant lesion in preterm infants; ischaemic necrosis of periventricular white matter, particularly the fibres subserving the lower limbs (which run closest to the ventricles). PVL is the characteristic substrate for spastic diplegia in preterm infants.
Kernicterus: Unconjugated bilirubin crosses the blood-brain barrier in the setting of severe neonatal hyperbilirubinaemia and deposits in the basal ganglia (globus pallidus especially), cochlear nuclei, and oculomotor nuclei. This produces the classic kernicterus triad: choreoathetoid (dyskinetic) CP + high-frequency sensorineural hearing loss + upward gaze palsy (from oculomotor nucleus damage). Kernicterus is entirely preventable through phototherapy and exchange transfusion.
Postnatal causes:
Bacterial meningitis, viral encephalitis, cerebral malaria, non-accidental head injury, and near-drowning can all produce permanent motor deficits during the postnatal period (up to age 2–3 years) that are classified as CP.
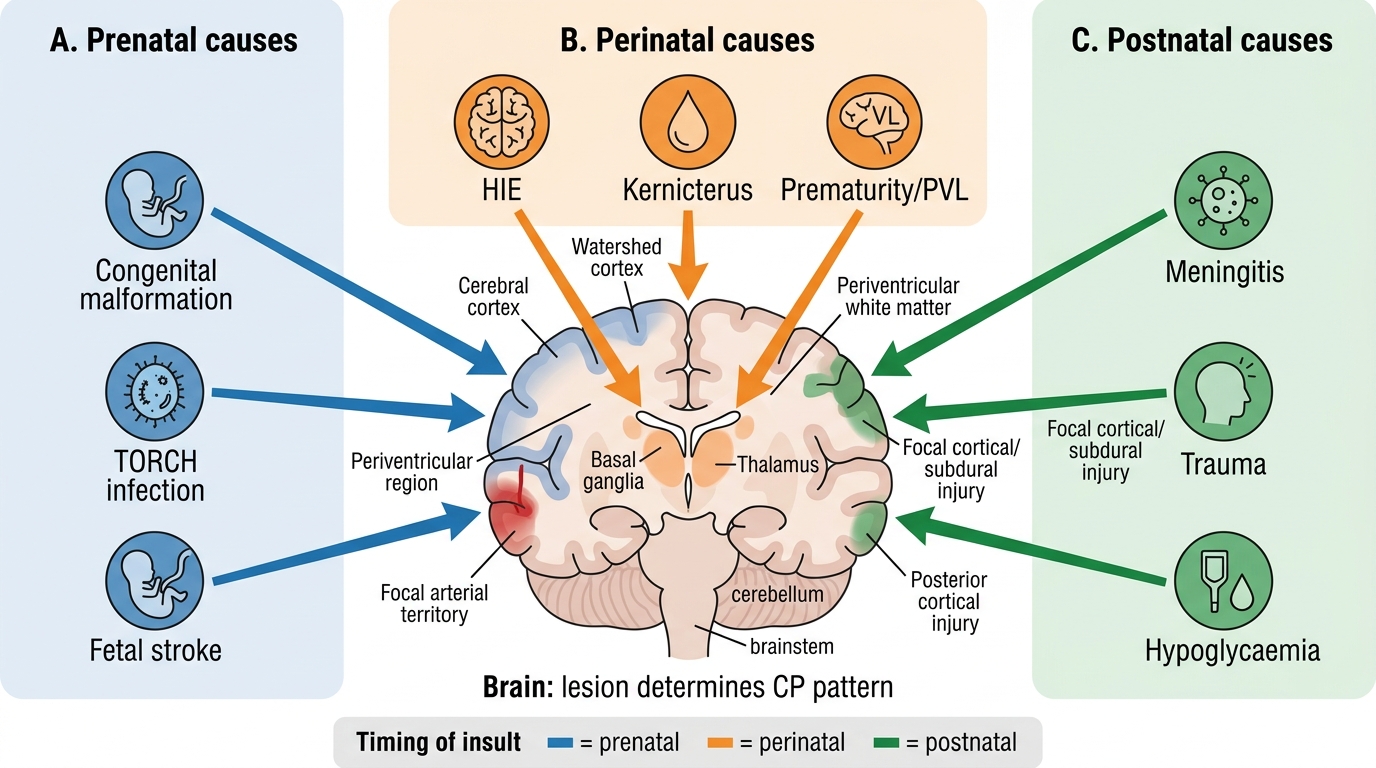
Causes of Cerebral Palsy by Timing of Brain Insult
Classification, Investigation and Diagnosis
Cerebral palsy is diagnosed clinically, based on a combination of risk-factor history, abnormal neurological examination, and developmental assessment. There is no single diagnostic test for CP; rather, the clinical diagnosis is supported by neuroimaging (MRI brain) to identify the underlying lesion and by screening investigations to detect treatable mimics and comorbidities. The functional severity is classified using the Gross Motor Function Classification System (GMFCS), which is the international standard and directly informs prognosis and therapy goal-setting.
Provided image
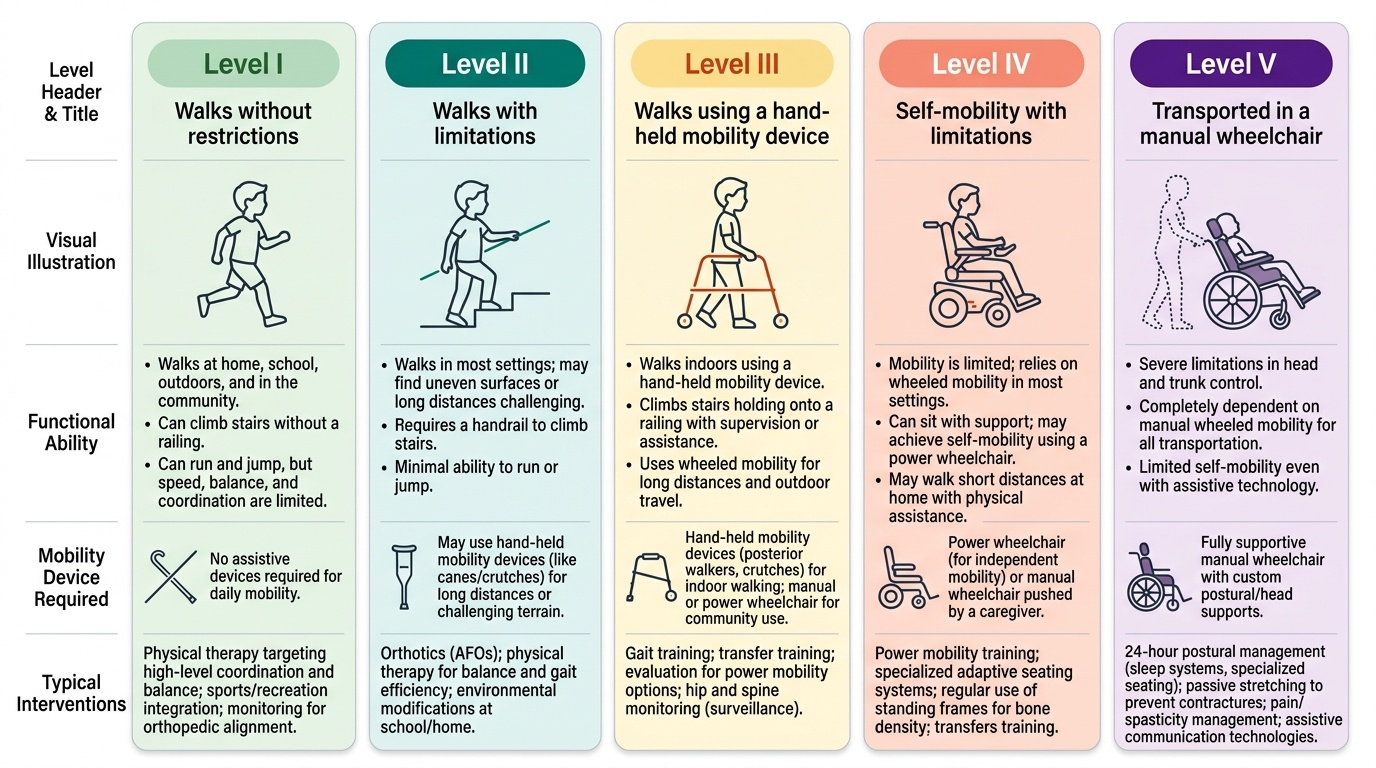
GMFCS (Gross Motor Function Classification System): A validated, 5-level ordinal scale describing a child's functional mobility. It is age-banded (2–4, 4–6, 6–12, and 12–18 years) and is the most clinically practical tool for communicating prognosis to families and planning interventions. Children at GMFCS Level I walk independently with minimal limitations; those at Level V are completely dependent in mobility and require wheelchair and postural support.
GMFCS Level Summary:
• Level I: Walks without restrictions; limitations in more demanding gross motor skills.
• Level II: Walks with limitations (uneven surfaces, stairs difficult); may use handrail; no wheeled mobility in community.
• Level III: Walks using hand-held mobility device (walker, crutches) indoors; wheeled mobility outdoors.
• Level IV: Powered wheelchair or attendant-propelled; limited self-mobility; supported sitting.
• Level V: Transported in wheelchair; limited ability to maintain anti-gravity head/trunk position; full support required.
Diagnosis — investigations:
• MRI brain: Investigation of choice; identifies the underlying structural lesion (PVL in preterm, cortical–subcortical injury in term HIE, basal ganglia signal in kernicterus, cortical malformations). Guides aetiology and prognosis. A normal MRI does not exclude CP.
• Metabolic screen: Tandem mass spectrometry, urine organic acids — to exclude treatable metabolic disorders mimicking CP.
• Karyotype/chromosomal microarray: If dysmorphic features suggest a genetic syndrome.
• EEG: If clinical or subclinical seizures suspected.
• Ophthalmological assessment: Visual field defects (hemiplegia), cortical visual impairment (severe HIE), strabismus (common).
• Hearing assessment (BERA/OAE): Mandatory — sensorineural hearing loss in kernicterus and postnatal meningitis.
• Developmental/psychometric assessment: Bayley, DASII for infants; IQ testing in older children to quantify intellectual comorbidity.
Common comorbidities of CP (must actively screen for all):
• Epilepsy: Up to 35–40%; most common in quadriplegic and cortical forms; less common in dyskinetic or purely diplegic CP.
• Intellectual disability: Present in ~50% overall; highest in spastic quadriplegia; may be absent in pure dyskinetic CP.
• Communication disorders: Dysarthria, AAC (Augmentative and Alternative Communication) needs.
• Sensory impairments: Visual (strabismus, cortical VI, field defects), Hearing (sensorineural — especially kernicterus).
• Feeding difficulties and dysphagia: Significant in quadriplegic CP; aspiration risk; NG tube or gastrostomy may be needed.
• Behavioural and psychiatric: ADHD, anxiety, autism features.
• Orthopaedic: Scoliosis, hip dislocation (from spasticity), limb length discrepancy, joint contractures.
SELF-CHECK
A 3-year-old boy born at 28 weeks gestation has bilateral increased tone in the lower limbs, brisk patellar reflexes, and walks with a scissor gait. Cognitive development appears near-normal. MRI brain shows periventricular leukomalacia. Which type of cerebral palsy best describes this child?
A. Spastic hemiplegia — the most common type of CP in preterm infants
B. Spastic diplegia — predominantly lower limbs affected, typical of periventricular leukomalacia in prematurity
C. Dyskinetic CP — periventricular leukomalacia classically causes choreoathetosis
D. Ataxic CP — cerebellar involvement is expected with prematurity
Reveal Answer
Answer: B. Spastic diplegia — predominantly lower limbs affected, typical of periventricular leukomalacia in prematurity
Periventricular leukomalacia (PVL) damages the white matter fibres subserving the lower limbs (which run closest to the ventricles in preterm brains), producing spastic diplegia — predominantly lower limb spasticity with relative sparing of the upper limbs and cognition. Dyskinetic CP and kernicterus are associated with basal ganglia lesions, not PVL. Ataxic CP arises from cerebellar lesions. Spastic hemiplegia is typically unilateral and more common in term infants with focal cortical/subcortical injury.