Page 20 of 48
PE27.6 | Febrile Seizures — SDL Guide (Part 2)
Complications and Risk Assessment
Parents invariably ask two questions after their child's febrile seizure: 'Will this happen again?' and 'Will my child get epilepsy?' These are clinically important questions with evidence-based answers that differ between simple and complex febrile seizures. A structured assessment of recurrence and epilepsy risk factors allows individualised counselling. Understanding these risks also guides the decision about whether to prescribe rescue benzodiazepines for home use, whether to refer to a paediatric neurologist, and how urgently follow-up should be arranged. The answers require distinguishing among three distinct outcomes: recurrence of febrile seizures (common, not serious), development of afebrile epilepsy (uncommon, significant), and the rare but serious complication of prolonged febrile seizure causing acute brain injury (febrile status epilepticus).
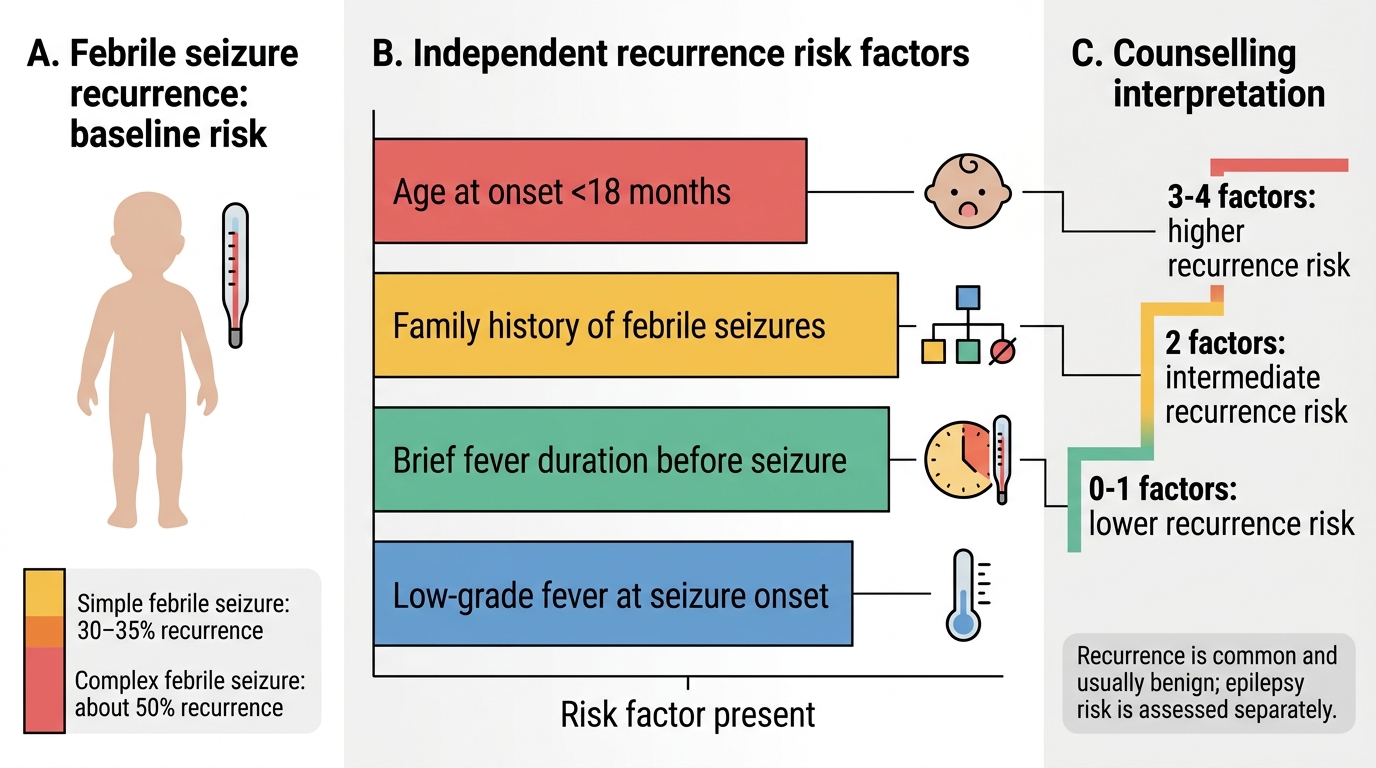
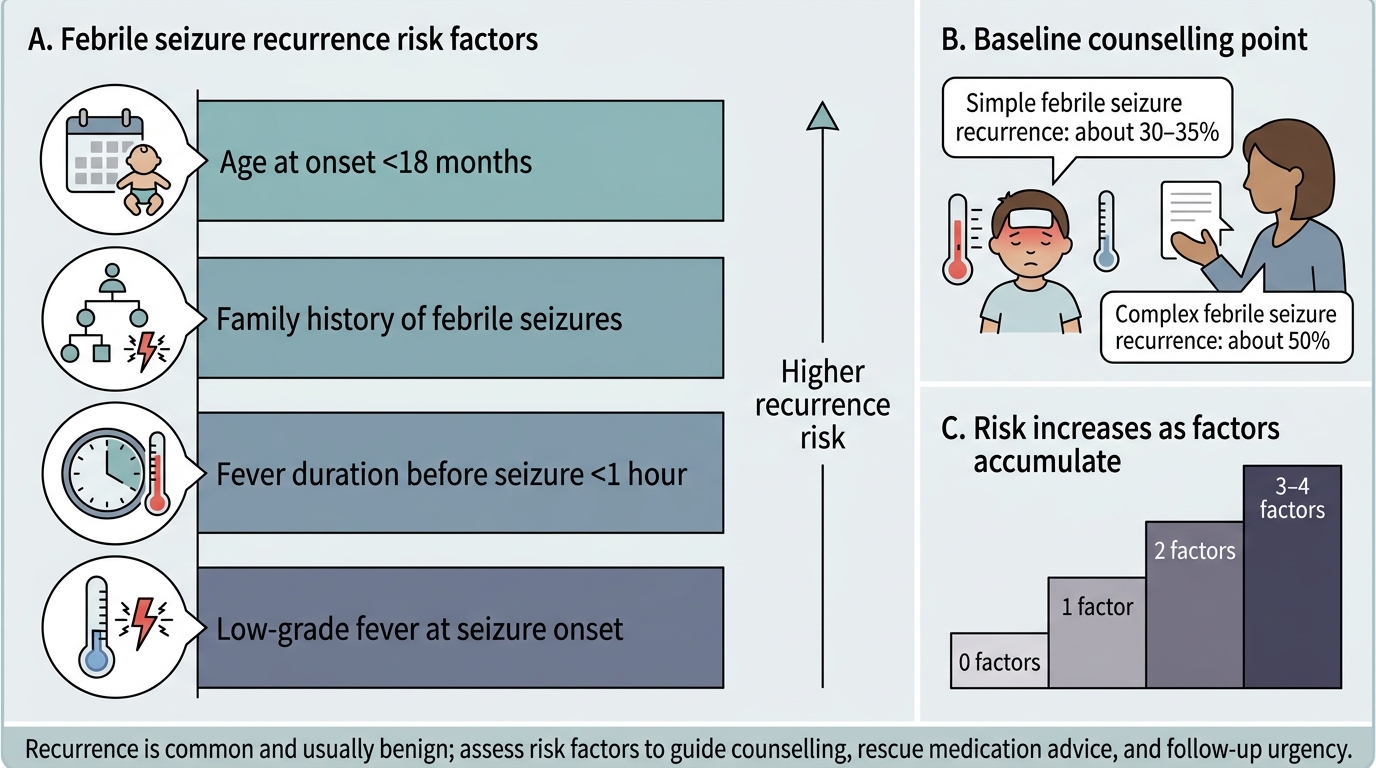
Recurrence risk:
Approximately 30–35% of children who have had one simple febrile seizure will have another. The risk is higher for complex febrile seizures (~50%). Four factors independently increase the risk of recurrence:
1. Age younger than 18 months at the time of the first febrile seizure
2. Family history of febrile seizures in a first-degree relative (parent or sibling)
3. Short duration of fever before the seizure (i.e., the seizure occurs early in the febrile illness, when the temperature is still rising rapidly — the most dangerous window)
4. Low-grade fever at the time of the seizure (the child has a low seizure threshold and triggers at lower temperatures)
Childen with all four factors have a ~70% recurrence risk; those with none have ~15%.
Risk of developing epilepsy:
• After a single simple febrile seizure: risk ~1–2% — marginally higher than the general population background risk of ~1%
• After complex febrile seizures, especially with multiple complex features: risk ~4–10%
• Risk factors for later epilepsy include: complex febrile seizure type, family history of afebrile epilepsy, pre-existing neurodevelopmental abnormality, and prolonged febrile seizure (especially with hippocampal signal change on MRI)
Important: Antipyretics do NOT prevent recurrence. Multiple randomised controlled trials (including the CHILD study) have demonstrated that aggressive antipyretic treatment (paracetamol, ibuprofen) during subsequent febrile illnesses does not reduce the probability of a recurrent febrile seizure. This is a critical counselling point — it relieves parents of the impossible burden of maintaining a fever-free state, which is neither achievable nor necessary.
Prolonged febrile seizure / febrile status epilepticus: the most serious immediate complication of febrile seizures is a seizure that does not stop spontaneously. Approximately 5% of febrile seizures last longer than 15 minutes. The FEBSTAT (Consequences of Prolonged Febrile Seizures in Childhood) study demonstrated that some children with prolonged febrile seizures develop acute hippocampal injury visible on MRI DWI immediately after the seizure, and a proportion develop mesial temporal sclerosis years later — the pathological substrate of temporal lobe epilepsy.
Recurrence Risk Factors for Febrile Seizures
Note: febrile seizures do NOT cause brain damage, intellectual disability, or death in the vast majority of children. This reassurance should be given explicitly, as parents often believe the opposite.
Recurrence Risk Factors for Febrile Seizures
SELF-CHECK
An 18-month-old child has a generalised tonic-clonic seizure lasting 2 minutes during a febrile illness. He recovers fully within 20 minutes. His temperature is 39°C, no meningeal signs. This is his first seizure. Which investigation is MOST appropriate?
A. Lumbar puncture to exclude meningitis
B. Urgent MRI brain
C. No investigations — reassure and observe
D. EEG to rule out epilepsy
Reveal Answer
Answer: C. No investigations — reassure and observe
This is a classic simple febrile seizure (generalised, <15 min, single episode) in an 18-month-old with no signs of meningitis (no neck stiffness, no petechiae, no bulging fontanelle, rapid recovery). In a child aged 12–18 months and above with a typical simple febrile seizure and clear clinical recovery, no investigations are routinely indicated. Lumbar puncture is not routine and is reserved for children with meningeal signs, prolonged post-ictal state, complex seizure in an ill-looking child, or age <12 months (where signs of meningitis may be subtle). EEG is not indicated in simple febrile seizures. MRI is reserved for complex features or focal neurology.
Diagnosis and Investigations
The diagnosis of a febrile seizure is entirely clinical — based on a careful history from witnesses, age of the child, presence of fever, seizure type and duration, and clinical examination showing the absence of meningeal signs and focal neurological deficits. There is no diagnostic investigation specific to febrile seizures; investigations are performed only to exclude dangerous mimics (meningitis, encephalitis) or to identify the source of fever. A common error is to reflexively order a battery of tests after any convulsive episode — this is costly, unnecessary, and exposes the child to painful procedures without benefit. The correct approach is to use the clinical history and examination to determine whether the seizure is truly a simple febrile seizure (in which case the investigation burden is minimal) or whether features are present that mandate investigation. The distinction rests primarily on the clinical assessment of meningism, seizure type, post-ictal duration, age, and immunisation status.
The core diagnostic question is: is this a febrile seizure, or is the seizure caused by CNS infection (meningitis/encephalitis)? The following clinical features would favour CNS infection over simple febrile seizure and mandate urgent LP:
• Neck stiffness, Kernig's sign, or Brudzinski's sign
• Bulging fontanelle in an infant
• Petechial or purpuric rash (suggests meningococcal disease)
• Altered consciousness not explained by postictal state (prolonged >1 hour without improvement)
• Complex seizure features (focal, prolonged, recurrent) in an ill-looking child
• Age <12 months (especially <6 months): meningeal signs are unreliable in very young infants; a lower threshold for LP is appropriate
Lumbar puncture (LP) — indications and contraindications:
| Indication for LP | Indication against routine LP |
|---|---|
| Age <12 months with first febrile seizure (if not fully immunised or ill) | Typical simple febrile seizure, age ≥18 months, fully immunised, recovered baseline |
| Signs of meningism | Rapid full recovery to normal baseline |
| Prolonged postictal state | Previously vaccinated (Hib, PCV, MenC reduces bacterial meningitis risk significantly) |
| Clinical suspicion of CNS infection | Identified peripheral source of fever (AOM, pharyngitis) |
EEG: Not indicated after a simple febrile seizure. EEG findings are often abnormal transiently after any seizure (postictal slowing) and do not predict recurrence or epilepsy risk. EEG may be considered after a complex febrile seizure or if there is clinical concern about an underlying epilepsy syndrome, but it is not a routine investigation.
MRI brain: Not routine for simple febrile seizures. Indicated for:
• Complex febrile seizure, especially prolonged (>15 min) — to assess for hippocampal injury (DWI) or structural pathology
• Focal seizure features suggesting a structural lesion
• Suspected encephalitis
Blood investigations: Glucose, electrolytes — only if the seizure is prolonged or the child appears ill; low glucose (hypoglycaemia) or low sodium (hyponatraemia) can trigger seizures and are treatable. Routine blood tests are not indicated for simple febrile seizures.
Source of fever: Identify and treat the precipitating infection — ear examination, throat, urine dipstick (in infants where UTI may be silent).
CLINICAL PEARL
Antipyretics control fever discomfort but do NOT prevent febrile seizure recurrence. This is one of the most important pieces of parental counselling you will give. Multiple RCTs have confirmed that aggressive paracetamol/ibuprofen use during fever does not lower the probability of a child re-seizing. Parents should be told explicitly: 'Giving paracetamol will not stop the seizure from happening — you cannot keep your child seizure-free by monitoring their temperature constantly.' This releases them from exhausting and futile fever-vigilance behaviour. The second equally important pearl: Febrile seizures are NOT caused by meningitis, and a child with a simple febrile seizure who looks well after recovery does NOT need a lumbar puncture.
Management
Management of a febrile seizure encompasses acute seizure management, investigation (as outlined above), identification and treatment of the fever source, and most importantly, comprehensive parental education and counselling. The vast majority of febrile seizures are self-terminating and do not require pharmacological intervention during the episode itself; the challenge is managing the episode safely while reassuring the family and avoiding unnecessary interventions. Effective management is less about drugs and more about communication — a family who understands what febrile seizures are, why antipyretics do not prevent them, and what to do if a seizure recurs is far better equipped than a family sent home with a prescription and inadequate explanation. This section therefore gives equal weight to the pharmacological rescue plan and the non-pharmacological parental education plan.
Acute management during the seizure:
Most simple febrile seizures stop spontaneously within 1–3 minutes. The priority is safety — not seizure termination — for the first five minutes:
• Lay the child on their side (recovery position) to protect the airway from secretions or vomiting
• Do NOT put anything in the mouth
• Clear the area of hazards; cushion the head gently
• Time the seizure from onset
• Do NOT restrain the child's movements — this can injure the child and does not stop the seizure
• Observe and time — if the seizure is still continuing at 5 minutes, it is unlikely to self-terminate and drug therapy is indicated
When to give benzodiazepine (seizure ≥5 minutes):
• Rectal diazepam: 0.5 mg/kg (weight-based) is the community/pre-hospital first-line agent; easily administered by trained parents or paramedics without intravenous access. Maximum dose typically 10 mg.
• Buccal midazolam (0.2–0.3 mg/kg) — preferred over rectal diazepam in many settings; equally effective and more socially acceptable; increasingly the standard first-line pre-hospital/community agent.
• Intravenous lorazepam (0.1 mg/kg, max 4 mg) — hospital first-line when IV access is available; onset ~2 minutes, duration of action ~12–24 hours.
• If the seizure continues after two benzodiazepine doses despite adequate airway management, manage as status epilepticus (see PE27.8 SDL).
Antipyretics:
• Paracetamol (15 mg/kg oral/rectal) or ibuprofen (7.5–10 mg/kg oral, ≥3 months) to provide fever comfort and reduce the child's distress.
• CRITICAL: These do NOT prevent seizure recurrence during the current or subsequent febrile illnesses — this must be communicated explicitly to parents.
No routine prophylactic AEDs:
• Continuous prophylactic AEDs (phenobarbitone, valproate) modestly reduce febrile seizure recurrence, but their side-effects (sedation, behavioural effects) outweigh benefits for simple febrile seizures.
• IAP guidelines and AAP guidelines do NOT recommend prophylactic AEDs for simple febrile seizures.
• In selected children with multiple complex febrile seizures, prolonged febrile seizures, or those at high risk of subsequent epilepsy, a brief course of intermittent diazepam at the time of febrile illness (0.3 mg/kg/8 h during fever) may reduce recurrence but does not prevent later epilepsy; discuss with a specialist.
Parental education (essential — this is the intervention):
• "Your child has had a febrile seizure — not epilepsy. It was caused by the fever, not by any damage to the brain."
• "Febrile seizures do not cause brain damage, learning disability, or death."
• "There is a 30–35% chance it may happen again during a future febrile illness. If it does, place your child on their side, time it, and bring them to hospital if it lasts more than 5 minutes."
• "Giving fever medication will make your child more comfortable but will NOT prevent the seizure from recurring."
• Provide written first-aid instructions; consider prescribing rectal diazepam or buccal midazolam for home use in children with recurrent or prolonged febrile seizures.
• Follow-up with the paediatrician within 2–4 weeks for reassessment and to answer questions.
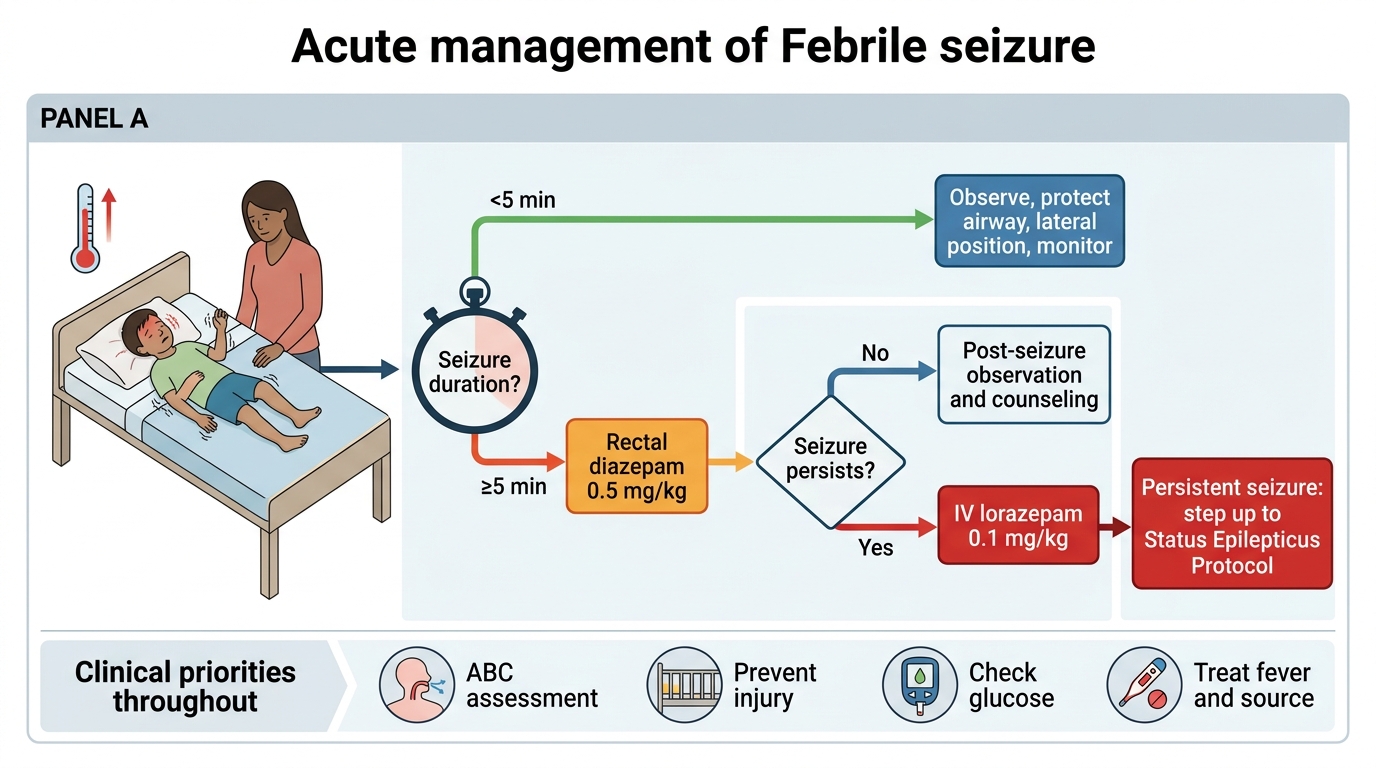
Acute Management Algorithm for Febrile Seizure
SELF-CHECK
Parents of a 2-year-old who just had a 2-minute simple febrile seizure ask: 'Should we give paracetamol every time he gets a fever to prevent another seizure?' The BEST evidence-based response is:
A. Yes — paracetamol prevents febrile seizures by controlling the fever
B. Use ibuprofen instead of paracetamol — it is more effective
C. Antipyretics reduce fever discomfort but do not prevent febrile seizure recurrence
D. Give diazepam prophylactically during every febrile illness
Reveal Answer
Answer: C. Antipyretics reduce fever discomfort but do not prevent febrile seizure recurrence
Multiple RCTs have shown that antipyretics (both paracetamol and ibuprofen) do not reduce febrile seizure recurrence despite controlling fever. The pathophysiology involves cytokine-mediated neuronal excitability changes and intrinsic seizure threshold reduction that are not abolished by temperature lowering alone. Parents should be reassured that antipyretics are given for comfort and general fever management, NOT as seizure prevention. Prophylactic diazepam during febrile illnesses modestly reduces recurrence in high-risk children but is not standard for all children with febrile seizures due to sedation risk and poor parent adherence.
Self-Assessment
Test your understanding with the following case-based questions:
Case A: A 14-month-old girl is brought in after a 20-minute generalised convulsion with fever (40°C). She is now drowsy and has mildly stiff neck. Temperature is 40.2°C. She has received all her vaccinations. Her eyes are deviated to the right.
Q1. This is most likely: (a) simple febrile seizure, or (b) complex febrile seizure? Which criterion(ia) make it complex?
Answer: Complex — THREE complex features: (i) duration ≥15 minutes (prolonged); (ii) focal eye deviation; (iii) neck stiffness raises concern for meningitis. In this context, lumbar puncture is mandatory despite full vaccination.
Case B: A 2-year-old boy has a 90-second generalised tonic-clonic seizure with fever. He recovers fully in 20 minutes. Neurological examination is normal. No meningeal signs. This is his second febrile seizure in 8 months.
Q2. Should he be started on prophylactic anti-epileptic medication?
Answer: No. This is a recurrent simple febrile seizure. IAP and AAP guidelines do not recommend prophylactic AEDs for simple febrile seizures because the side-effects of daily AED therapy outweigh the modest benefit of reducing recurrence. The family should be educated and provided with rectal diazepam or buccal midazolam for home use if a seizure occurs and lasts >5 minutes.
Q3. What is the most important counselling message to give this family?
Answer: "Febrile seizures do not cause brain damage or epilepsy in the vast majority of children. Giving paracetamol or ibuprofen during fever will not prevent another seizure. If a seizure occurs, place your child on their side, time it, and use the rectal diazepam we have prescribed only if it lasts more than 5 minutes."
Key summary points:
• Febrile seizures: fever ≥38°C + seizure, age 6 months–5 years, no CNS infection.
• Simple = generalised + <15 min + single in 24 h. Complex = focal OR ≥15 min OR recurrent.
• No routine LP in typical simple febrile seizure in child ≥12 months with no meningeal signs.
• Antipyretics do NOT prevent recurrence.
• No prophylactic AEDs for simple febrile seizures.
• Recurrence ~30–35%; epilepsy risk ~1–2% (simple), ~4–10% (complex).