Page 5 of 20
PE30.3-4 | Diabetes Mellitus — SDL Guide (Part 2)
Management: Insulin Therapy, DKA Protocol, and Long-term Care
The management of Type 1 DM rests on exogenous insulin, dietary management, blood glucose monitoring, and education. Insulin is the only treatment option for T1DM — it is not a sign of disease severity but the mandatory and life-saving replacement for a missing hormone. Children with T1DM are started on a basal-bolus insulin regimen: a long-acting insulin (glargine or detemir) once daily as the background (basal), and rapid-acting insulin (aspart, lispro, or regular) given with each meal (bolus). The starting total daily dose is typically 0.5–1 U/kg/day, split approximately 50% basal and 50% bolus. Dose adjustments are guided by pre-meal and post-meal glucose monitoring (target: pre-meal 80–130 mg/dL, post-meal <180 mg/dL). Injection sites must be rotated to prevent lipohypertrophy, which impairs insulin absorption.
DKA Management Protocol (paediatric-specific — critically different from adults):
The single most important principle: avoid rapid fluid administration to prevent cerebral oedema, which is the main cause of DKA mortality in children.
- Airway and resuscitation: If shocked (absent pulses, prolonged CRT) → 10 mL/kg isotonic saline (0.9% NaCl) IV bolus over 30 minutes, maximum 20–30 mL/kg; avoid unnecessary extra fluid boluses.
- Fluid deficit replacement: Calculate the deficit (usually 5–10% dehydration in DKA). Replace the deficit PLUS maintenance over 48 hours (NOT 24 hours — this slower rehydration reduces cerebral oedema risk). Use isotonic saline (0.9% NaCl ± KCl); switch to 0.45% NaCl only after initial fluid administration.
- Insulin infusion: Start regular insulin (soluble insulin) at 0.05–0.1 U/kg/hour IV infusion. Do NOT give an insulin bolus in children. Begin insulin 1–2 hours AFTER starting IV fluids (this allows volume restoration before the insulin-driven shift of glucose and potassium intracellularly). Target glucose fall: 50–100 mg/dL/hour.
- Potassium: All children in DKA have total body potassium depletion despite possibly normal serum K on admission. Add 40 mEq/L of KCl to IV fluids once urine output is confirmed and serum K <5.5 mEq/L. Monitor K every 2–4 hours.
- Bicarbonate: Routine bicarbonate is NOT recommended in paediatric DKA — it can worsen CNS acidosis. Give only for life-threatening acidosis (pH <6.9) with haemodynamic compromise.
- Transition to subcutaneous insulin: When DKA resolves (pH >7.3, HCO3 >15, eating) → transition to subcutaneous insulin. Give first subcutaneous dose 30 minutes BEFORE stopping the insulin infusion (overlap prevents relapse).
Cerebral oedema is the most feared complication of paediatric DKA — risk is greatest in young children and new-onset cases. Warning signs: severe headache, bradycardia, rising blood pressure (Cushing's triad), deteriorating consciousness. Treatment: mannitol 0.5–1 g/kg IV (or 3% saline 2.5–5 mL/kg) immediately, reduce fluid rate, call neurosurgery/ICU.
Hypoglycaemia (glucose <70 mg/dL) is the most common acute complication in established DM: give 15 g fast-acting glucose orally (if conscious) → recheck in 15 minutes. If unconscious: glucagon 0.5–1 mg IM or IV dextrose 0.2–0.5 g/kg (2 mL/kg of 10% dextrose).
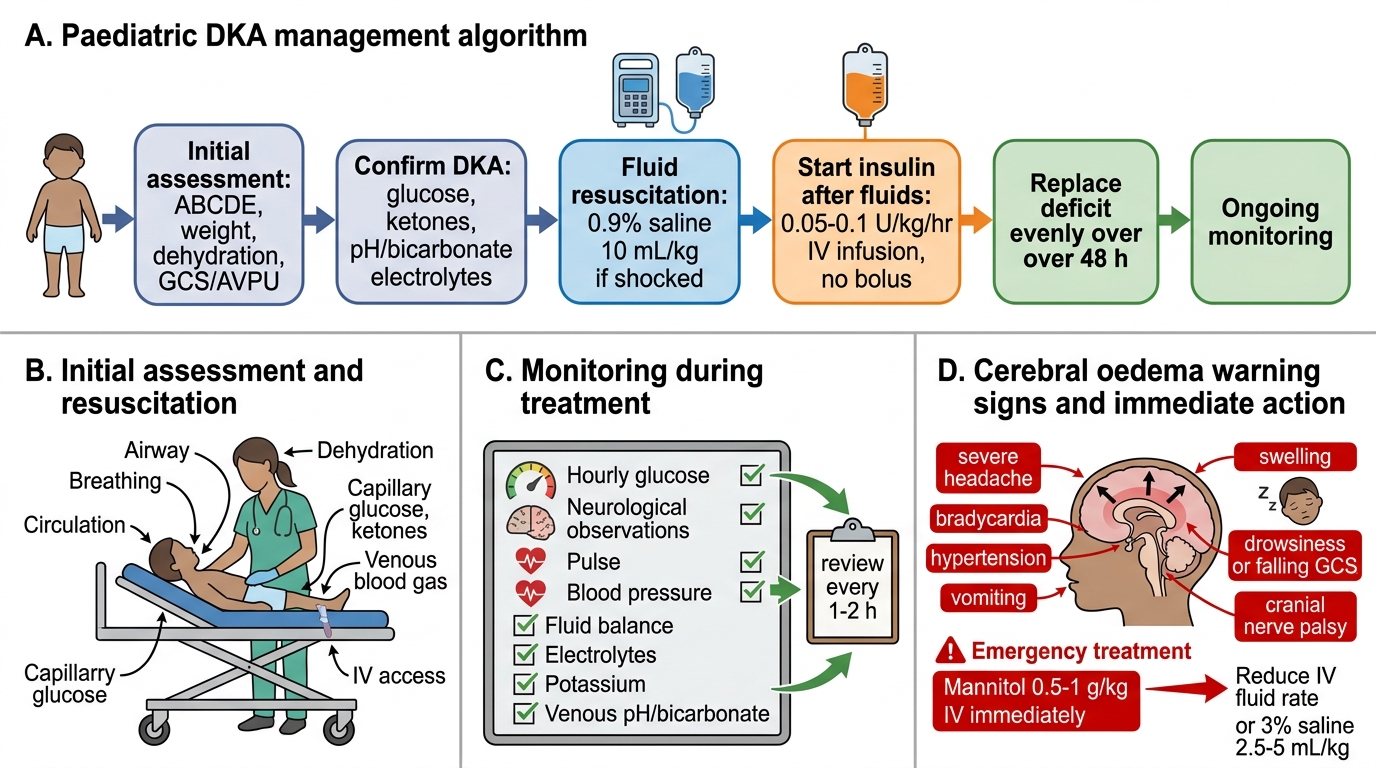
Paediatric DKA Management Algorithm
SELF-CHECK
A child with DKA has been on IV fluids for 4 hours. Nursing calls because the child has developed a severe headache, and on your review his heart rate has dropped from 120 to 68 bpm and blood pressure has risen. He is becoming increasingly drowsy. What is the MOST likely complication and the immediate treatment?
A. Hypoglycaemia — give IV dextrose bolus
B. Hyponatraemia — increase sodium in IV fluids
C. Cerebral oedema — give mannitol 0.5–1 g/kg IV immediately and reduce fluid rate
D. Hypokalaemia — add more potassium to IV fluids
Reveal Answer
Answer: C. Cerebral oedema — give mannitol 0.5–1 g/kg IV immediately and reduce fluid rate
This is the classic presentation of cerebral oedema complicating paediatric DKA: severe headache + Cushing's triad (bradycardia + hypertension) + deteriorating consciousness. This is a neurosurgical emergency. Mannitol 0.5–1 g/kg IV (or 3% hypertonic saline 2.5–5 mL/kg) must be given immediately. Simultaneously reduce the IV fluid rate to decrease the osmotic gradient driving cerebral oedema. This is the leading cause of death from DKA in children and must be anticipated and acted on instantly.
Complications and Self-Assessment
The complications of diabetes mellitus in children span acute and chronic. Among the acute complications, DKA (discussed in management) is the most dangerous. Hypoglycaemia is the most frequent acute complication in children on insulin — young children cannot reliably communicate symptoms (sweating, tremor, palpitation), making hypoglycaemia unawareness particularly dangerous in this age group. Nocturnal hypoglycaemia can occur silently. Chronic complications begin to manifest after approximately 5 years of poorly controlled diabetes: microvascular — diabetic nephropathy (microalbuminuria is the earliest sign; screen annually), diabetic retinopathy (screen after 5 years' duration or at puberty), and peripheral neuropathy; macrovascular — atherosclerosis begins in childhood in uncontrolled DM. The good news is that tight glycaemic control (HbA1c <7.0–7.5% in children per ISPAD) significantly delays and reduces all chronic complications — the DCCT trial demonstrated this definitively.
Psychosocial complications — depression, diabetes distress, disordered eating — are common in adolescents with T1DM and should be actively screened for. The child and family need structured education (sick-day rules, hypoglycaemia management, injection technique, self-monitoring), and school teachers should be informed about the condition.
Self-assessment case: An 8-year-old boy, 24 kg, presents with DKA (glucose 420 mg/dL, pH 7.15, HCO3 8 mEq/L, moderate dehydration 7%). Approximate management: (a) Fluid deficit = 7% × 24 kg = 1,680 mL; maintenance ≈ 1,400 mL/24h (Holliday-Segar: 100 mL/kg for first 10 kg = 1000 mL + 50 mL/kg for next 10 kg = 500 mL + 20 mL/kg for remaining 4 kg = 80 mL = 1,580 mL/24h ÷ 2 = ~790 mL/12h; but over 48h = total fluid 1680+1580×2=5040 mL, given as 105 mL/h). (b) Insulin: 0.05–0.1 U/kg/hr = 1.2–2.4 U/hr of regular insulin. (c) Monitor glucose hourly, K every 2–4h, watch for cerebral oedema. This is a referral case — stabilise and transfer to a centre with paediatric ICU.
CLINICAL PEARL
The three cardinal rules for paediatric DKA management that differ from adults:
1. Fluid over 48h, NOT 24h — slower rehydration is the primary prevention of cerebral oedema, the leading DKA killer in children.
2. Insulin dose is 0.05–0.1 U/kg/hour — NOT the adult 0.1 U/kg/hr; lower starting dose in young children reduces hypoglycaemia and osmotic swings.
3. Never miss cerebral oedema — headache + bradycardia + hypertension + declining consciousness in a child receiving DKA treatment = mannitol NOW. Do not wait for imaging; treat immediately.