Page 13 of 20
PE30.7 | Endocrine Growth Deviation Referral — SDL Guide
Learning Objectives
- Define the clinical thresholds that distinguish a normal growth variant from a pathological deviation requiring investigation
- Accurately measure height and weight, plot on IAP/WHO charts, and calculate growth velocity
- Compute mid-parental height and interpret it in relation to the child's actual centile
- Differentiate familial short stature, constitutional delay of growth and puberty (CDGP), GH deficiency, hypothyroidism, Turner syndrome, chronic illness, and failure to thrive (FTT) using clinical features and growth pattern
- Apply evidence-based referral criteria to decide urgency of specialist referral and communicate effectively with the family
INSTRUCTIONS
Growth monitoring is among the most powerful screening tools available in paediatric practice. A single height measurement tells little; it is the pattern across time — the velocity, the centile trajectory, the relationship to parental heights and bone maturation — that reveals whether a child is thriving normally or labouring under a treatable disorder. Missing a case of GH deficiency or hypothyroidism in a school-age child means years of impaired stature and development that could have been corrected. This module builds the practical skill of systematically evaluating any child whose growth raises concern, from the consulting room measurement to the referral letter.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 16 (Growth and Development) and Ch. 17 (Endocrine Disorders) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 16 (Normal and Variant Stature) and Section XI (Growth Hormone Deficiency) (textbook)
- IAP Growth Charts 2015 (Khadilkar et al.) — standard reference for Indian children (guideline)
- Greulich & Pyle Atlas for Bone Age Assessment (wrist radiograph) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Priya, a 10-year-old girl, is brought to the outpatient clinic by her anxious parents. Her classmates have started calling her 'the shortest girl in class,' and her teacher has raised concerns. On measurement she is 118 cm — well below the 3rd centile on the IAP chart. You note that her mother is 152 cm and her father is 162 cm. Last year's school record shows she was 115 cm. She appears generally well, with no dysmorphic features immediately obvious. The parents ask: 'Is something wrong with her? Does she need injections?' You have 10 minutes to decide whether this child needs urgent referral, watchful waiting, or simple reassurance.
WHY THIS MATTERS
Growth disorders are among the most common reasons a child is brought to a paediatrician in India, yet they are also among the most frequently mismanaged — either over-investigated as normal variants or under-recognised when a treatable condition is present. The skill tested here is not memorising a list of diagnoses; it is the sequential clinical reasoning that separates the child who simply has short parents from the one with GH deficiency, hypothyroidism, or Turner syndrome. Because GH replacement and levothyroxine can restore near-normal adult height if started before growth plates fuse, a timely referral from a primary-care doctor or general paediatrician carries real, measurable benefit for the child's life. Conversely, unnecessary referrals burden tertiary centres and cause family anxiety. Mastering this triage skill is therefore a direct NMC competency: PE30.7 explicitly requires you to identify deviations and plan appropriate referral.
RECALL
Before proceeding, activate what you already know. Recall the three phases of postnatal growth: rapid infancy (25 cm in year 1), slower childhood (5–7 cm/yr), and the pubertal growth spurt (8–12 cm/yr girls, 9–13 cm/yr boys). Recall that growth hormone, thyroid hormone, sex steroids, insulin, and adequate nutrition all act on the growth plate. Recall the WHO/IAP growth chart structure — centile lines representing 3rd, 15th, 50th, 85th, 97th percentiles, and that a healthy child's measurement tracks along roughly the same centile line from year to year. Recall from your nutrition modules that failure to thrive (FTT) is defined by weight falling across centile lines and is distinct from short stature. Recall the causes of hypothyroidism (PE30.1) and Turner syndrome (PE30.5) from your endocrine cluster — both present commonly with growth failure.
When Growth Becomes a Clinical Problem: Indications for Assessment
Growth deviation becomes a clinical concern when a child's growth pattern departs from expected norms in a way that cannot be explained by parental stature alone. The most common presentations that bring children to clinical attention include short stature, tall stature, failure to gain weight appropriately (FTT), and disproportionate growth — and each has a distinct risk of underlying pathology. Understanding when to be concerned, rather than reassuring, is the first clinical skill in this domain.
Provided image
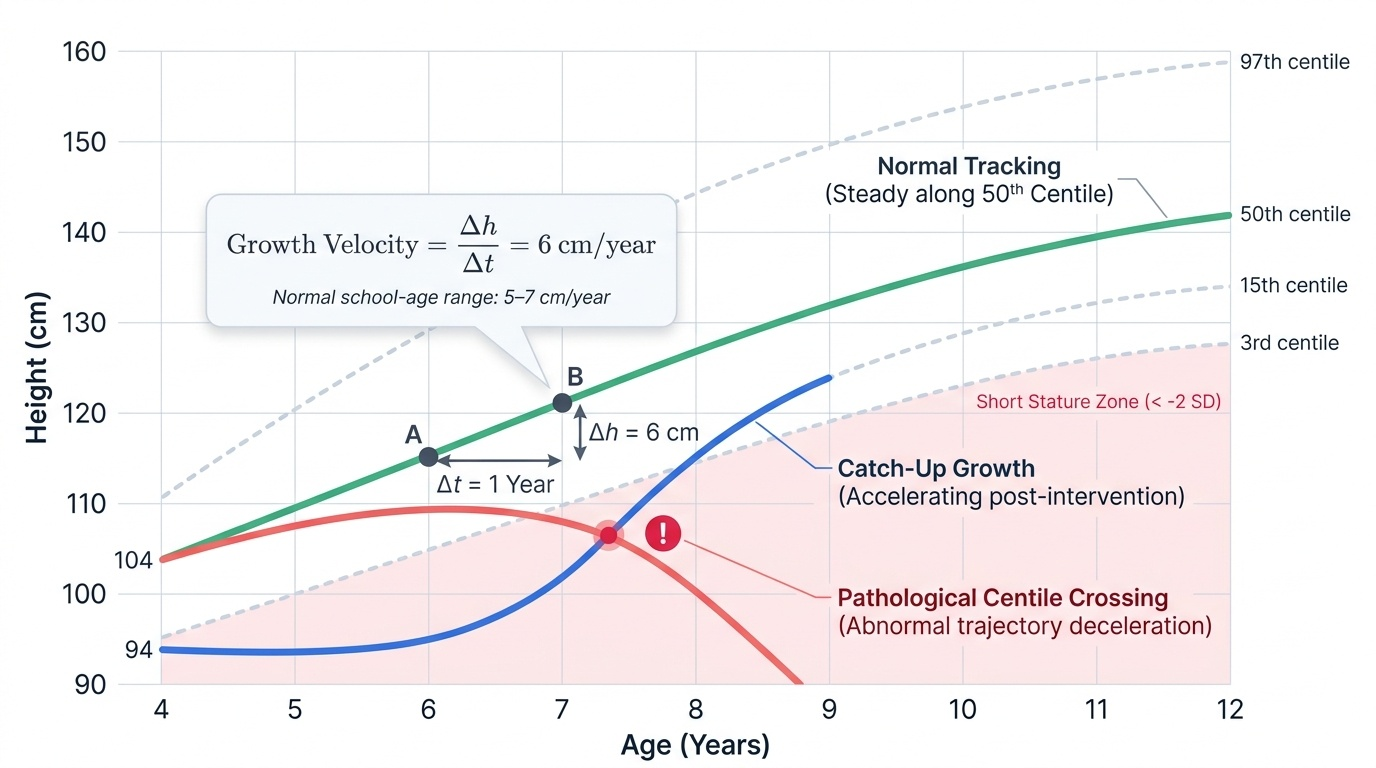
Short stature is technically defined as height below the 3rd centile (approximately −2 SD from the mean) for age and sex on an appropriate growth chart. However, the centile position alone is insufficient to determine pathology — a child with two short parents who is tracking steadily on the 2nd centile is almost certainly a normal variant, whereas a child who was on the 50th centile at age 4 and has fallen to the 10th centile by age 8 warrants urgent investigation regardless of absolute height. This distinction — between absolute position and centile trajectory — is the most important clinical concept in growth assessment.
Growth velocity is the rate of height gain expressed in centimetres per year. It is calculated from at least two measurements taken 6–12 months apart, under standardised conditions. A growth velocity below 4–5 cm/year in a school-age child is a clinically significant red flag regardless of current centile position, because it indicates that the child is falling away from the normal growth trajectory. In contrast, a child who is short but growing at a normal velocity (5–7 cm/yr) is far more likely to have a normal variant (familial or constitutional) than a treatable endocrine cause.
Tall stature and accelerated growth also warrant assessment when they are disproportionate, associated with early puberty (precocious puberty causing bone-age advancement and ultimate short stature despite current tall appearance), or accompanied by dysmorphic features suggesting Marfan or Klinefelter syndromes.
Failure to thrive (FTT) must be distinguished from short stature from the outset. FTT is primarily a disorder of weight — it is defined by weight falling across two or more major centile lines downward over time, particularly when height is initially preserved. Short stature may be a consequence of prolonged FTT but is not synonymous with it. Confusing the two leads to a different (and wrong) investigative pathway.
- Short stature: height <3rd centile or >2 SD below mean for age and sex
- Growth velocity red flag: <4–5 cm/yr in school-age children (6–12 years)
- Centile deviation: crossing ≥2 major centile lines downward = always refer
- Tall stature: height >97th centile or >2 SD above mean; concern if crossing upward
- FTT: weight falling ≥2 centile lines; weight-for-height declines before height-for-age
Growth Physiology: Principles Governing Normal and Deviant Growth
To understand why a child is growing abnormally, you must first understand the hormonal and nutritional machinery that drives normal growth. Growth is not a passive process of time passing — it requires the coordinated action of the GH-IGF-1 axis, thyroid hormone, adequate substrate (nutrition), and the structural competence of the growth plate (epiphyseal cartilage). A deficiency in any of these produces characteristic patterns of growth failure that can be diagnosed clinically and biochemically.
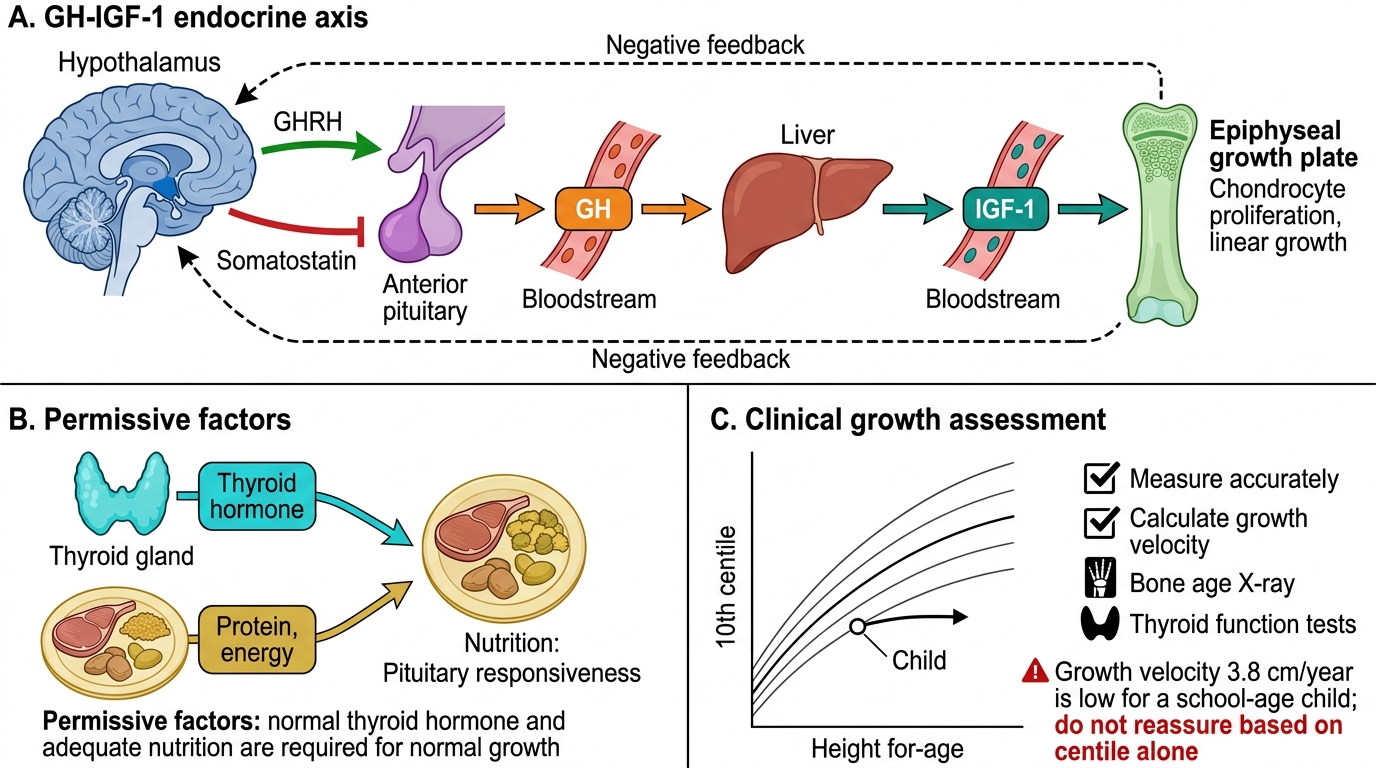
The growth hormone (GH) axis begins in the hypothalamus, which pulses growth hormone-releasing hormone (GHRH) into the pituitary portal circulation. This stimulates the anterior pituitary somatotrophs to release GH in pulsatile bursts, predominantly during slow-wave sleep. GH acts on the liver (and other tissues) to generate insulin-like growth factor-1 (IGF-1), which is the principal anabolic mediator at the growth plate — stimulating chondrocyte proliferation and hypertrophy. GH also has direct anabolic effects on muscle and adipose tissue. Disruption at any point — hypothalamic, pituitary, or target organ — can cause GH deficiency (GHD), which presents with slow growth velocity, increased body fat, and normal body proportions.
Thyroid hormone (T3/T4) is a permissive factor: it is required for normal GH secretion from the pituitary and for the response of growth plate cartilage to GH/IGF-1. Hypothyroidism in childhood therefore causes growth failure that mimics GH deficiency but also includes characteristic features such as delayed bone age, weight gain (rather than the lean phenotype of GHD), constipation, bradycardia, dry skin, and goitre. Congenital hypothyroidism, if untreated after neonatal screening, causes severe growth and developmental retardation (cretinism).
Nutrition provides the substrate: adequate protein and energy are required for normal GH secretion and IGF-1 generation. Malnutrition — whether from inadequate intake (poverty, neglect), malabsorption (coeliac disease, chronic diarrhoea), or chronic disease with increased catabolism — suppresses the GH-IGF-1 axis and produces growth failure that is disproportionate (weight affected earlier and more severely than height in acute malnutrition; height affected in chronic/stunting).
Bone age reflects skeletal maturation independent of chronological age. It is assessed by comparing a left-hand wrist radiograph with the Greulich and Pyle atlas. A bone age significantly behind chronological age (>2 years delay) indicates either constitutional delay (as in CDGP, where bone maturation will eventually catch up) or pathological hypothyroidism/GHD. A bone age advanced ahead of chronological age suggests precocious puberty or hyperthyroidism. Bone age is essential for predicting adult height and for counselling families about expected growth trajectory.
GH-IGF-1 Axis and Growth Assessment
SELF-CHECK
A 7-year-old girl has a growth velocity of 3.8 cm/yr. Her height is on the 10th centile. Her mother and father are on the 15th and 20th centile respectively. What is the most important next step?
A. Reassure the family — height is consistent with mid-parental height
B. Request bone age and thyroid function tests, and calculate growth velocity formally
C. Prescribe growth hormone empirically and review in 6 months
D. Repeat height measurement in 3 months only
Reveal Answer
Answer: B. Request bone age and thyroid function tests, and calculate growth velocity formally
Although the current centile is close to mid-parental height, a growth velocity of 3.8 cm/yr is below the red-flag threshold of 4–5 cm/yr for a school-age child. This indicates she is falling away from her trajectory. The centile position alone does not exclude pathology — pathological growth failure often begins as a velocity problem before manifesting as centile crossing. Bone age and TFTs are the first-line investigations to exclude hypothyroidism and assess constitutional delay. Reassurance without investigation at this velocity is inappropriate. GH is never empirical.
The Structured Approach: Plotting, Growth Velocity, and Mid-Parental Height
The clinical evaluation of a child with suspected growth deviation follows a structured, sequential approach. Deviation in any step can invalidate the entire assessment — a single inaccurate height measurement or an incorrectly selected growth chart can lead to wrong conclusions. The following procedure should be followed systematically in every child referred for growth concern.
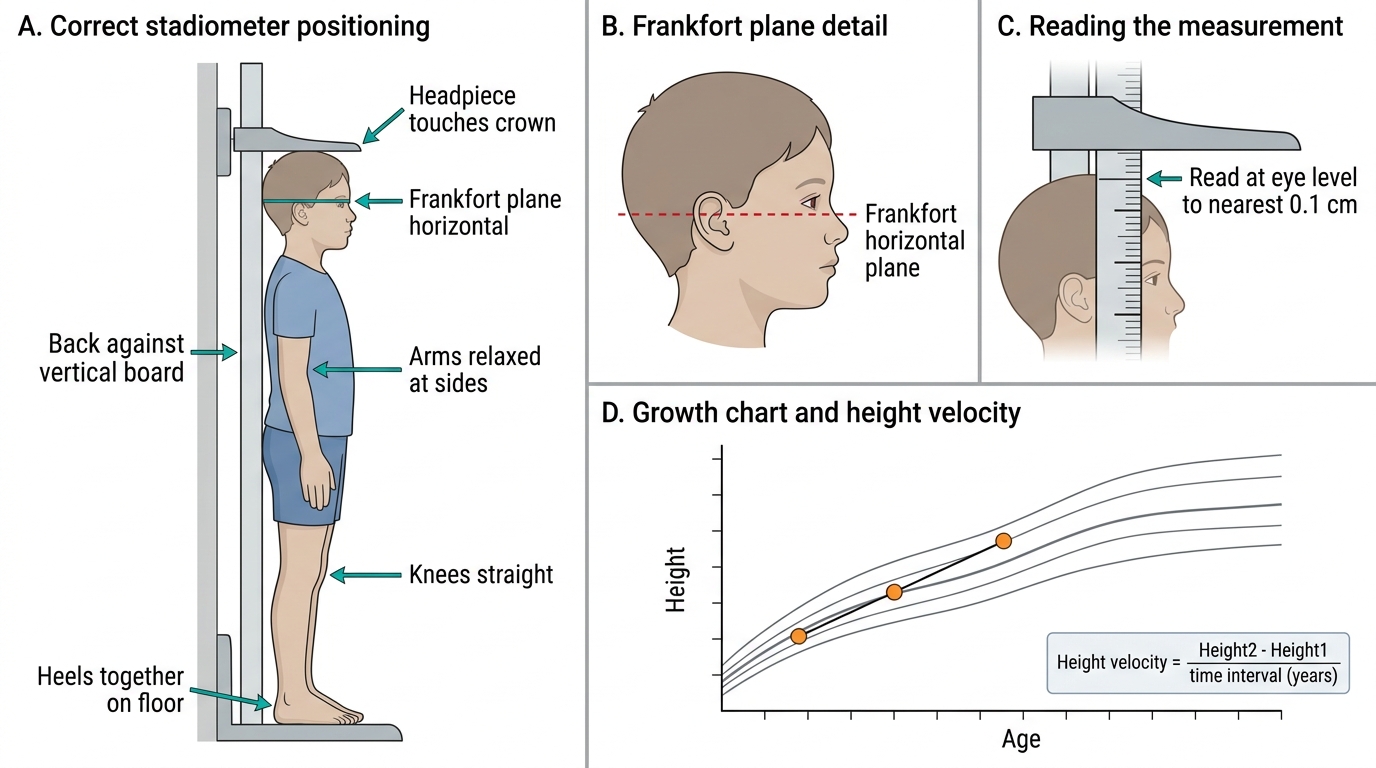
Step 1 — Accurate measurement. Height must be measured with a calibrated stadiometer (not a tape measure or door-frame mark) with the child standing barefoot, heels together and touching the backboard, knees straight, looking forward (Frankfort plane). Weight is measured without shoes or excess clothing on a calibrated scale. Head circumference is measured in children under 3 years. Note that home or school measurements are often unreliable and should not substitute for clinic-based measurement.
Step 2 — Select the correct chart. Use WHO growth charts (2006) for children under 5 years — these represent the growth of optimally-fed, healthy children and are the international standard. Use IAP Growth Charts 2015 for Indian children aged 5–18 years — these incorporate Indian population data and are the recommended standard by the Indian Academy of Pediatrics. Using an adult or Western chart for an Indian child may misclassify normal as abnormal.
Step 3 — Plot and identify the centile. Plot the current measurement on the appropriate chart. Record the age precisely (use a calendar to calculate age in completed months). Then retrieve any previous growth records (school health records, immunisation cards, child health registers, old clinic notes) and plot those historical points. The resulting pattern across time is far more informative than any single measurement.
Step 4 — Calculate growth velocity. Growth velocity (cm/yr) = (current height − previous height) ÷ time interval in years. For example, if a child was 115 cm at 9.5 years and is 118 cm at 10.5 years, velocity = (118 − 115) ÷ 1 = 3 cm/yr — well below the 5–7 cm/yr expected for a 10-year-old. Growth velocity requires a minimum 6-month interval; shorter intervals introduce measurement error. A 12-month interval is ideal for school-age children.
Step 5 — Calculate mid-parental height (MPH) and target range. MPH represents the genetic growth potential the child has inherited. It is calculated as:
• Boys: MPH (cm) = (father's height + mother's height + 13) ÷ 2
• Girls: MPH (cm) = (father's height + mother's height − 13) ÷ 2
The target height range = MPH ± 8.5 cm (representing the 3rd–97th centile range within which the child should eventually fall). A child growing well below the lower limit of the target range warrants investigation, even if both parents are also short — it suggests an additional pathological process on top of genetic potential.
Step 6 — Request bone age when indicated. If growth velocity is low, height is significantly below MPH target, or the child is significantly short without explanation, request a left-hand wrist X-ray for bone age assessment using the Greulich and Pyle atlas. A bone age ≥2 years behind chronological age is significant and narrows the differential considerably.
Key facts to memorise:
• Minimum measurement interval for reliable growth velocity: 6 months (12 months ideal)
• MPH formula for boys: (F + M + 13)/2; for girls: (F + M − 13)/2; target range ±8.5 cm
• Bone age >2 years delayed = significant (GHD, hypothyroidism, CDGP all possible)
Correct Stadiometer Technique and Growth Chart Plotting