Page 11 of 20
PE30.6 | Puberty Disorders — SDL Guide (Part 2)
Management of Precocious and Delayed Puberty
Management depends on the type and cause. The overarching goals in precocious puberty are to halt premature sexual development, protect adult height (by slowing bone-age advancement), and treat any underlying pathology. In delayed puberty, the goal is to confirm constitutional vs pathological delay, treat the cause, and where appropriate initiate sex-hormone replacement to complete puberty and avoid the psychological burden of absent puberty.
Provided image
Management of central (GnRH-dependent) PP:
First-line treatment is a GnRH analogue (GnRHa) — triptorelin or leuprolide — given as a depot injection every 4 weeks (or histrelin implant). GnRHa works by continuously stimulating the GnRH receptor, desensitising it and switching off LH/FSH secretion → sex steroids fall → puberty halts. This treatment preserves adult height (by slowing bone-age advancement), prevents early menarche, and relieves the psychosocial burden of early puberty. Treatment is continued until the appropriate pubertal age (~10–11 years in girls, ~11–12 in boys), at which point GnRHa is stopped and puberty resumes naturally. CNS causes (tumour, hamartoma) are treated on their own merit — not all hypothalamic hamartomas require neurosurgery.
Management of peripheral (GnRH-independent) PP:
Treat the underlying cause: ovarian cyst (many regress spontaneously), CAH (hydrocortisone to suppress excess adrenal androgens), adrenal/ovarian tumour (surgical). GnRHa is NOT effective for peripheral PP because the HPG axis is already suppressed.
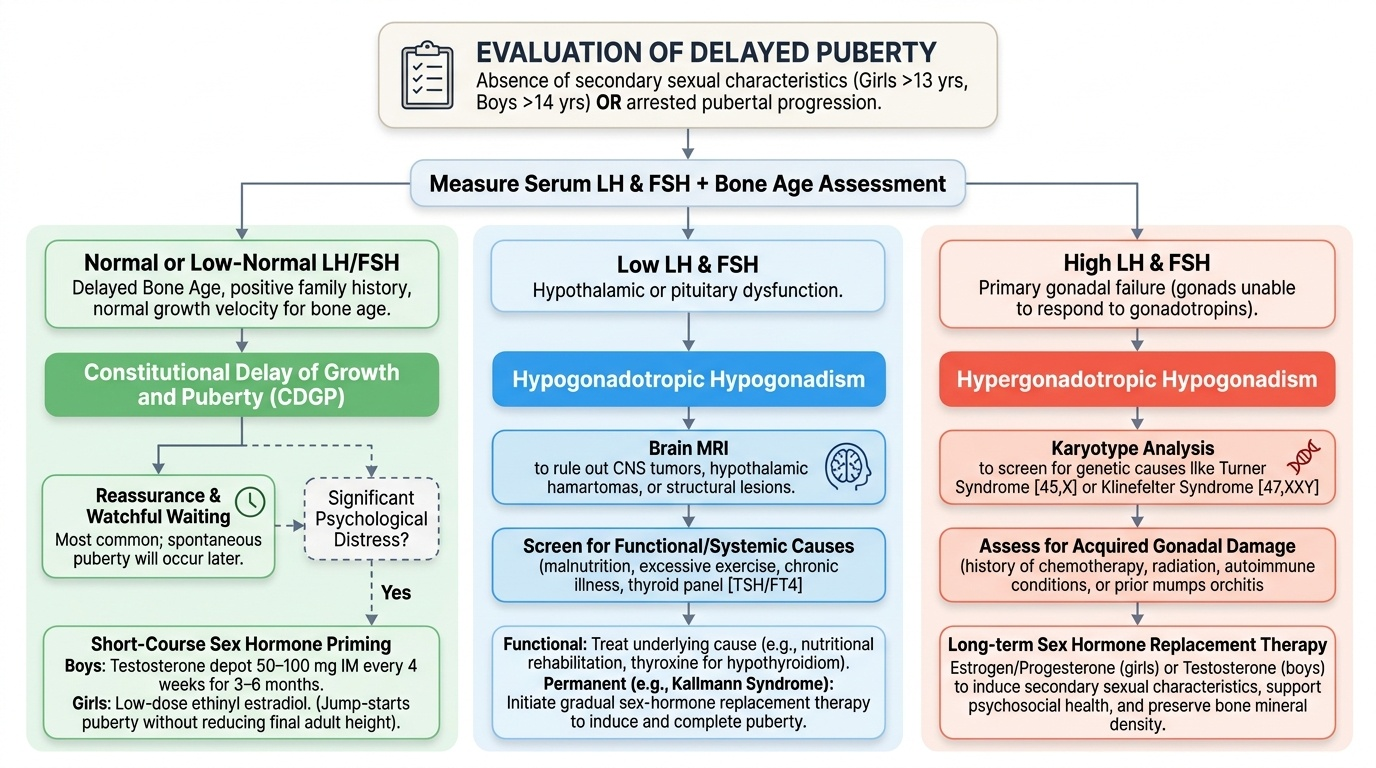
Management of constitutional delay of growth and puberty (CDGP):
The most common cause of delayed puberty requires reassurance and watchful waiting — these children will enter puberty spontaneously, just later. The key is to confirm CDGP by ruling out pathological causes (normal LH/FSH, delayed bone age, positive family history, no systemic illness). Where psychological distress is significant, a short course of low-dose sex hormone priming (testosterone depot 50–100 mg IM every 4 weeks for 3–6 months in boys; low-dose ethinyl estradiol in girls) can jump-start puberty — it does not affect final adult height.
Management of hypogonadism:
Hypogonadotrophic hypogonadism: treat the cause (e.g. thyroxine for hypothyroidism, nutrition for malnutrition); sex hormone replacement for permanent hypogonadism (Kallmann syndrome). Hypergonadotrophic hypogonadism (gonadal failure): sex hormone replacement (testosterone in boys, oestrogen-progesterone cycling in girls) to complete puberty and maintain adult physiology; fertility options discussed at appropriate age.
SELF-CHECK
A 15-year-old boy has no pubic hair and testicular volume of 3 mL (Tanner G1). His LH is 18 IU/L and FSH is 24 IU/L (both elevated). Bone age is 15.5 years. Karyotype is 47,XXY. What is the diagnosis and management direction?
A. Constitutional delay of growth and puberty — reassure and wait
B. Hypogonadotrophic hypogonadism — brain MRI
C. Klinefelter syndrome (hypergonadotrophic hypogonadism) — testosterone replacement therapy
D. Central precocious puberty — GnRH analogue
Reveal Answer
Answer: C. Klinefelter syndrome (hypergonadotrophic hypogonadism) — testosterone replacement therapy
47,XXY karyotype with elevated LH and FSH (the pituitary is trying hard to stimulate the failing testis), small testes, absence of secondary sexual development, and appropriate bone age = Klinefelter syndrome, a primary (hypergonadotrophic) hypogonadism. This is NOT constitutional delay (CDGP has normal/low-normal LH/FSH and delayed bone age). Management: testosterone replacement therapy to complete puberty, build muscle mass, prevent osteoporosis, and support sexual function. Genetic counselling and fertility options (sperm retrieval attempts) are also discussed.
Self-Assessment and Case Application
Apply the full clinical framework to the following scenarios, practising the same thought process you will use with a real patient: identify the abnormal finding → classify the timing disorder → interpret the investigations → determine the management. This stepwise approach prevents premature closure — a common error where students diagnose 'precocious puberty' without distinguishing central from peripheral, then choose the wrong treatment. Developing a reliable clinical reasoning pattern now — before you face these presentations alone — is the purpose of this self-assessment. The two cases below represent the two most common referral scenarios you will encounter: a girl with early breast development sent by a concerned school nurse, and an adolescent boy who has never started puberty and is increasingly withdrawn. Notice how the LH/FSH result is the pivot point in Case 1 (central vs peripheral PP) and how the bone age is the pivot point in Case 2 (CDGP vs pathological delay). Train yourself to identify that pivot before looking for the answer.
Case 1 — Precocious puberty: A 6-year-old girl has breast development (Tanner B2–B3), sparse pubic hair (PH2), and height 120 cm (>95th centile for age 6). Bone age on wrist X-ray is 9.5 years. LH = 7 IU/L, FSH = 5 IU/L (both pubertal). Serum estradiol is elevated.
• Diagnosis: Central (GnRH-dependent) precocious puberty
• Next step: Brain MRI (she is below 6 years at onset — higher probability of CNS pathology even in girls; also mandatory given age)
• Management: GnRH analogue (triptorelin or leuprolide) to halt progression and protect adult height
• Refer to paediatric endocrinologist
Case 2 — Delayed puberty: A 14.5-year-old boy has testicular volume 3 mL bilaterally (Tanner G1), no pubic hair, and height 155 cm (50th centile). Bone age is 12 years. LH and FSH are low-normal. His father says he entered puberty at 17 years of age.
• Diagnosis: Constitutional delay of growth and puberty (CDGP) — most likely, given delayed bone age, normal/low-normal LH/FSH, positive family history
• Differential to exclude: Check TFTs (hypothyroidism), FBC (chronic anaemia), U+E (renal disease), Kallmann (anosmia?)
• Management: Reassurance; if psychosocial distress significant → short course low-dose testosterone priming; spontaneous puberty expected by age 16–17
SMR clinical skill check: When performing Tanner staging in clinical practice, always ensure privacy, explain the procedure to the child and obtain assent, use appropriate body language, and have a chaperone. Document the stage (e.g. 'Breast B3, Pubic hair PH2') — not just a narrative description.
CLINICAL PEARL
Three critical rules for puberty disorders:
1. Age thresholds are fixed: Precocious puberty = <8 years in girls, <9 in boys. Delayed = no breast development by 13 (girls), no testicular enlargement by 14 (boys). These numbers are examined; do not mix them up.
2. Always do brain MRI in boys with precocious puberty — 50% have a CNS cause. In girls, MRI is recommended for onset <6 years or neurological features.
3. CDGP diagnosis is by exclusion — you must rule out thyroid disease, chronic illness, hypogonadism, and CNS pathology before concluding 'constitutional delay'. The positive finding (delayed bone age + normal LH/FSH + family history) supports it, but exclusion comes first.