Page 1 of 32
PE31.1 | Childhood Tuberculosis Clinical Spectrum — SDL Guide
Learning Objectives
- Describe the epidemiology and risk factors for tuberculosis in children and adolescents in India
- Explain the pathogenesis of primary tuberculosis complex and progression to active disease
- Enumerate the clinical types of pulmonary tuberculosis in children with their distinguishing features
- Identify the major forms of extrapulmonary tuberculosis and their clinical presentations
- Recognise the complications of childhood tuberculosis and factors that worsen outcomes
INSTRUCTIONS
India carries the world's largest TB burden, and children represent a significant and often overlooked segment of that burden. Childhood TB behaves differently from adult TB — primary infection usually begins in the lung parenchyma and hilar lymph nodes, and young children (<5 years) are at highest risk of disseminated and fatal disease. Understanding the clinical spectrum — from asymptomatic latent infection through primary complex to miliary TB and tuberculous meningitis — equips you to diagnose TB early, before irreversible complications occur. This module builds the clinical knowledge base; the companion SDL (pe24-tb-diagnosis) covers the diagnostic workflow.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 10 — Tuberculosis (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 254 — Tuberculosis (textbook)
- IAP Consensus Statement on Childhood Tuberculosis, 2020 (guideline)
- WHO Operational Handbook on Tuberculosis, Module 5 — Management of Tuberculosis in Children and Adolescents, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 3-year-old boy is brought to the OPD by his mother with a 6-week history of low-grade fever, poor appetite, and failure to gain weight. His mother mentions that the father was treated for 'chest TB' 4 months ago. On examination the child is thin (weight-for-age below −2 SD), has a BCG scar on the left arm, and you note mildly enlarged right-sided cervical lymph nodes that are firm and non-tender. His chest X-ray shows right hilar enlargement with a faint right lower lobe infiltrate. You suspect childhood tuberculosis — but how does this differ from adult TB, and what is the full spectrum of disease this child might develop?
WHY THIS MATTERS
Tuberculosis is the leading single-pathogen cause of infectious-disease mortality globally and in India. Children account for approximately 10–15% of the total TB burden in India, yet they are frequently under-diagnosed because their disease is paucibacillary and atypical. Children less than 5 years of age and adolescents are at highest risk for progression from infection to severe, disseminated disease. Unlike adults, children rarely have cavitary disease or are infectious; instead, they suffer primary complex, miliary spread, and meningitis — complications that carry high mortality and long-term sequelae. Recognising TB early — before complications set in — changes the outcome fundamentally.
RECALL
Before proceeding, activate the following prior knowledge:
• Mycobacterium tuberculosis is an obligate aerobe, acid-fast bacillus (AFB), transmitted via respiratory droplet nuclei (particles <5 µm that remain airborne); recall the Ziehl-Neelsen stain from Microbiology.
• Cell-mediated immunity (CMI) is the primary defence against intracellular pathogens: macrophages ingest bacilli, T-lymphocytes (CD4+) release IFN-γ, which activates macrophages to kill organisms; recall from Immunology/Physiology.
• Granuloma formation: activated macrophages → epithelioid cells → Langhans giant cells → central caseous necrosis = the hallmark TB lesion.
• BCG vaccine is given at birth in the Indian National Immunization Schedule (NIS); it protects primarily against severe childhood forms (miliary, TBM) rather than pulmonary TB in adults.
• Malnutrition impairs CMI; recall SAM criteria: weight-for-height <−3 SD, MUAC <11.5 cm (6–59 months), or bilateral pedal oedema.
Epidemiology of Childhood Tuberculosis
India has the world's highest TB burden, contributing approximately 26% of global TB cases according to the WHO Global TB Report. Children (<15 years) account for roughly 10–15% of all TB notifications in India, translating to hundreds of thousands of cases annually — a figure likely an underestimate given the diagnostic challenges in this age group. Childhood tuberculosis shares the same pathogen (Mycobacterium tuberculosis) and transmission route as adult TB, but the clinical expression and disease spectrum differ substantially because of the child's developing immune system and smaller airways.
Provided image
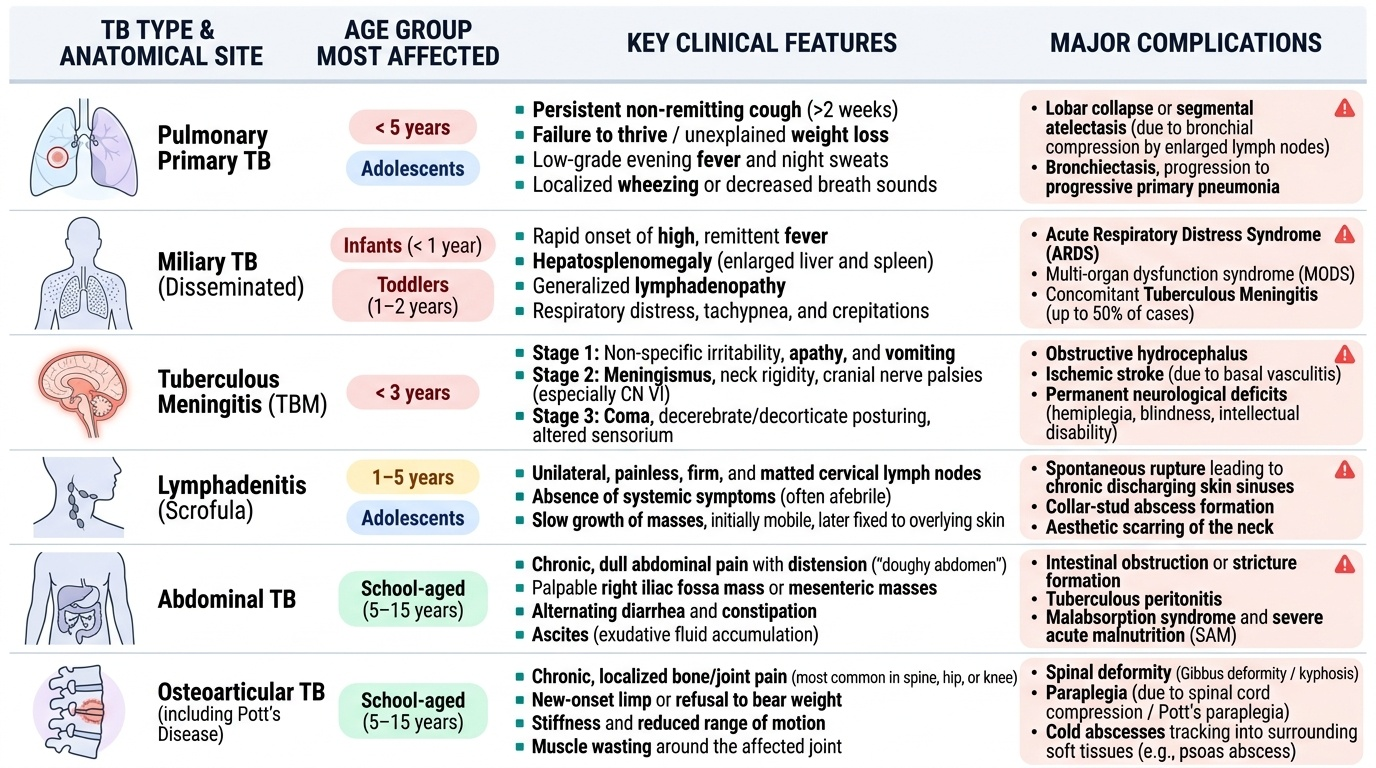
Risk is age-stratified: children under 5 years are at the greatest risk of rapid progression from primary infection to active and disseminated disease. The probability of developing disease after infection is ~50% in infants, ~25% in children 1–5 years, and ~10–15% in those 5–10 years. Adolescents (10–19 years) show an adult-like risk pattern, with an increased prevalence of cavitary pulmonary disease. Key risk factors for progression include:
• Close household contact with a smear-positive pulmonary TB case (the single greatest risk factor in children)
• Malnutrition — particularly SAM (weight-for-height <−3 SD or MUAC <11.5 cm), which impairs macrophage function and T-cell responses
• HIV co-infection — dramatically increases risk of TB reactivation and dissemination
• Age < 2 years (immature CMI)
• Measles (transient immunosuppression)
• Overcrowding, poor ventilation, and socioeconomic deprivation
India's BCG vaccination at birth (NIS) provides approximately 80% protection against severe childhood forms — miliary TB and tuberculous meningitis — but confers less protection against pulmonary TB in older children and adults. Contact history elicitation is therefore the single most important clinical act in any child presenting with unexplained fever, weight loss, or respiratory symptoms.
Pathogenesis and Primary Complex
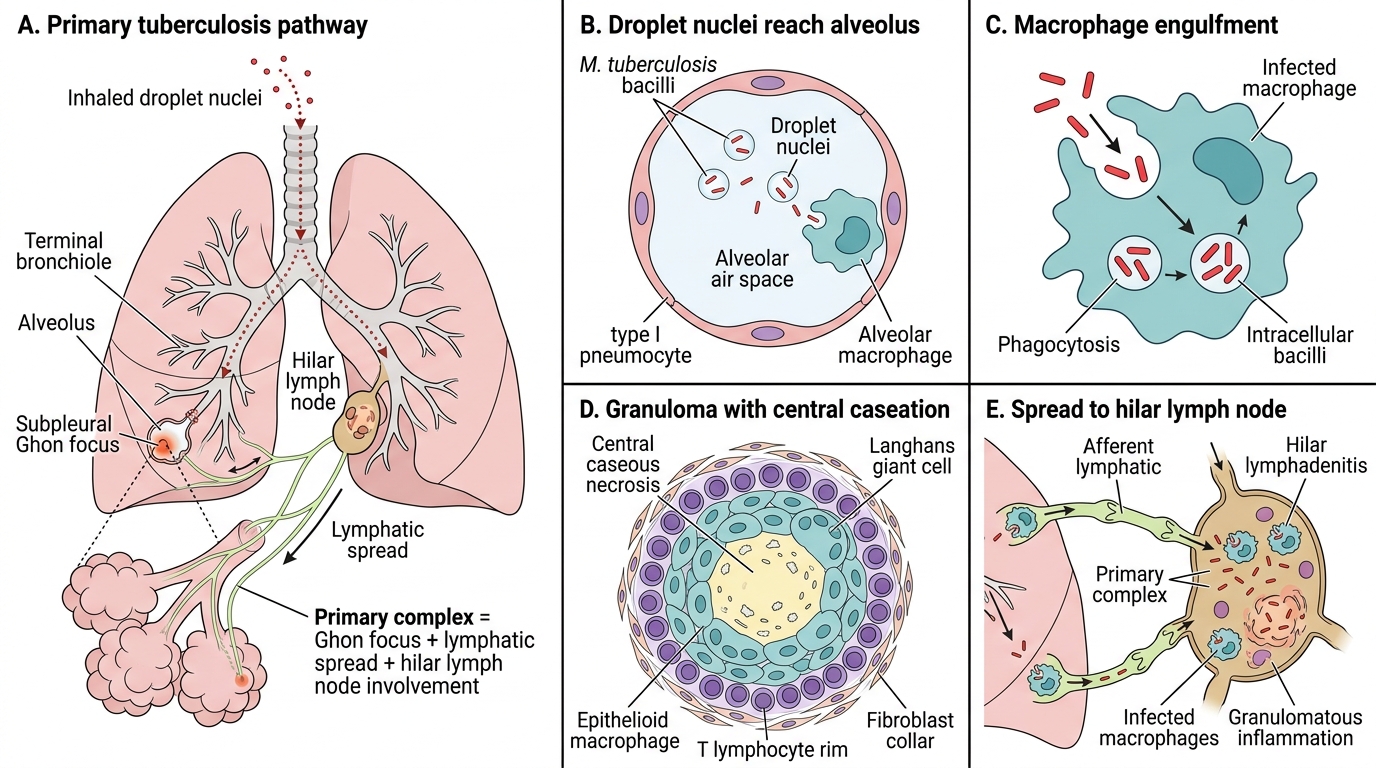
The pathogenesis of childhood tuberculosis begins with inhalation of droplet nuclei containing M. tuberculosis. Unlike adults who are often re-exposed, most children experience primary infection — their first encounter with the organism — and the resulting lesion is the primary complex, which is the pathological cornerstone of paediatric TB.
After inhalation, bacilli settle in the subpleural parenchyma of the mid- and lower lung zones (where ventilation is greatest), where alveolar macrophages engulf them. In immunologically naïve individuals, the bacilli survive inside macrophages and multiply. A localised inflammatory focus develops — the Ghon focus (also called the primary focus or primary lesion): a small area of caseous pneumonitis typically 1–2 cm in diameter. From the Ghon focus, bacilli spread via lymphatics to the regional hilar lymph nodes, which enlarge — constituting the primary complex (Ranke complex): Ghon focus + hilar/mediastinal lymphadenopathy + lymphangitis connecting them.
The lymphadenopathy in childhood TB is disproportionately prominent compared to adults; enlarged hilar nodes can cause airway compression, leading to obstructive collapse or hyperinflation of segments — a distinctly paediatric complication. Approximately 2–4 weeks after infection, CMI develops: sensitised T-lymphocytes release IFN-γ, macrophages become bactericidal, and granuloma formation walls off the organisms. In most immunocompetent children, the primary complex heals by fibrosis and calcification — a Ghon's focus seen on CXR in adulthood. Latent TB infection (LTBI) ensues: the Mantoux test (TST) becomes positive, but the child has no symptoms of active disease.
In a minority, especially those under 5 or who are immunocompromised, the primary infection does not heal:
• The Ghon focus enlarges → progressive primary pneumonia with lobar consolidation
• Lymph node compression of the bronchus → collapse-consolidation (segmental lesion)
• Bacillaemia occurs early in primary infection → haematogenous dissemination → miliary TB or TBM
• Pleural seeding → primary TB pleural effusion
Formation of Ghon Focus and Primary Complex
SELF-CHECK
A 2-year-old unvaccinated child who is a household contact of a smear-positive TB case has a Mantoux test of 12 mm induration with no symptoms, no fever, and a normal chest X-ray. The MOST appropriate interpretation is:
A. Active pulmonary tuberculosis — start treatment immediately
B. Latent TB infection (LTBI) — consider isoniazid preventive therapy
C. BCG reaction — no action required
D. False positive — repeat the test in 6 weeks
Reveal Answer
Answer: B. Latent TB infection (LTBI) — consider isoniazid preventive therapy
A TST ≥10 mm in an immunocompetent child in contact with TB is positive and, in the absence of symptoms and radiological evidence of active disease, represents LTBI. This child should receive isoniazid preventive therapy (IPT) per NTEP/IAP guidelines. BCG reaction typically causes ≤15 mm in infants <2 years but the interpretation threshold in this high-risk contact remains ≥10 mm. The test is not false-positive in a high-risk setting, and starting full treatment without evidence of active disease is inappropriate.
Pulmonary Tuberculosis in Children
Pulmonary tuberculosis in children encompasses a spectrum from asymptomatic primary infection to life-threatening miliary disease. The forms are recognised by their CXR correlates and clinical severity.
Provided image
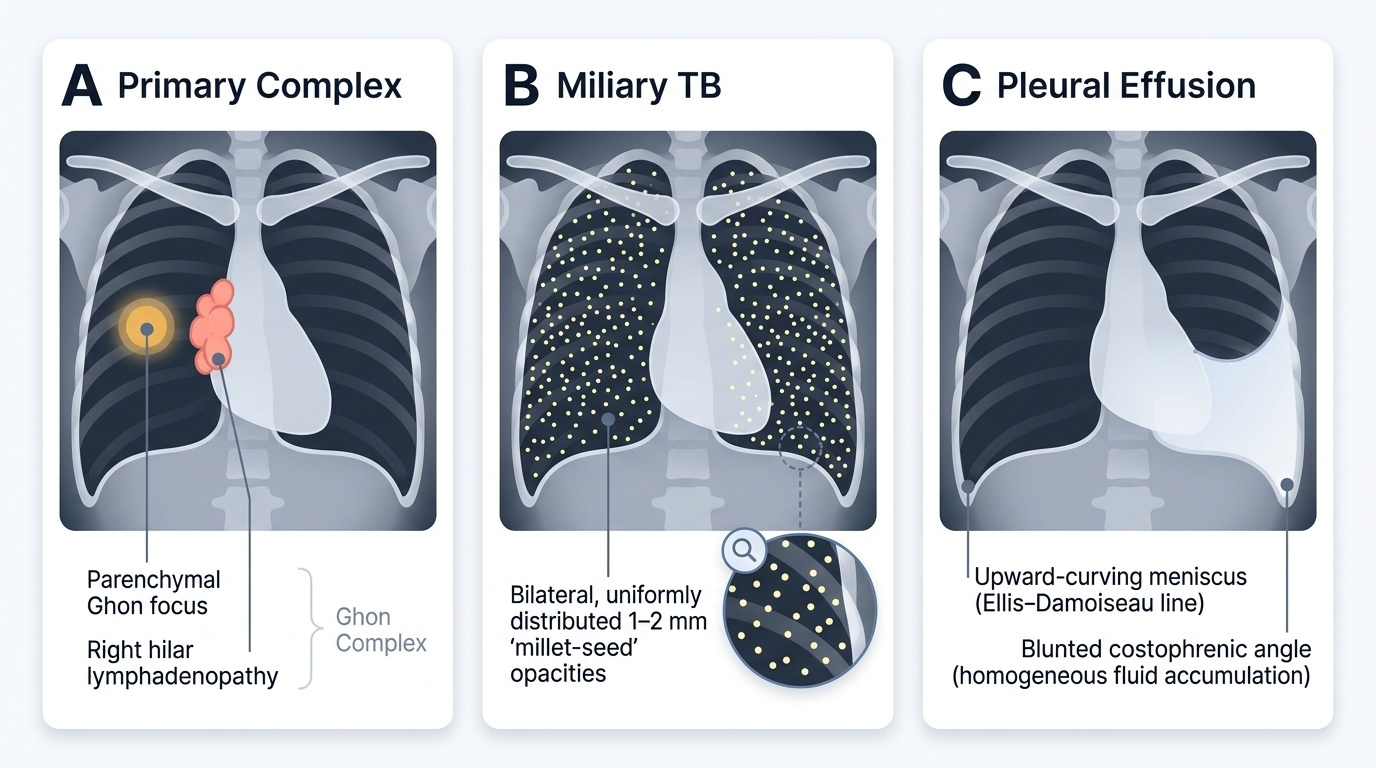
1. Primary complex (uncomplicated): Most common form. The child may be asymptomatic or have mild, non-specific symptoms — low-grade fever, poor weight gain, mild cough, lethargy. Physical examination may be unremarkable. CXR shows the hallmark: a parenchymal opacity (Ghon focus) with ipsilateral hilar/mediastinal lymphadenopathy. The majority resolve with treatment without sequelae.
2. Progressive primary tuberculosis: Occurs when the Ghon focus enlarges progressively instead of healing. The child has persistent fever, productive cough, and signs of consolidation — dullness, bronchial breath sounds, crepitations. CXR shows lobar or segmental consolidation, distinguishable from bacterial pneumonia by its chronicity (>2 weeks without response to antibiotics) and lymphadenopathy. Airway compression by enlarged lymph nodes can cause wheeze, stridor, or segmental collapse — the 'epituberculosis' pattern.
3. Miliary tuberculosis: Results from massive haematogenous dissemination during primary infection or reactivation, most common in children under 2 years. Clinically the child is acutely ill: high fever, tachypnoea, hepatosplenomegaly, and constitutional wasting. The CXR appearance is pathognomonic: bilateral, uniformly distributed, 1–2 mm millet-seed nodules (hence the name) throughout both lung fields. Choroidal tubercles on fundoscopy are diagnostic of miliary TB but may require dilated fundoscopy to detect. Miliary TB carries significant mortality without prompt treatment.
4. Primary tuberculous pleural effusion: A hypersensitivity reaction to TB antigen in the pleural space; occurs more in older children and adolescents. The child presents with pleuritic chest pain, fever, and dyspnoea. CXR shows unilateral effusion; pleural fluid is an exudate (lymphocyte predominant), and AFB smear is often negative — ADA (adenosine deaminase) elevation is diagnostically helpful.