Page 14 of 32
PE31.10 | Exanthematous Illnesses — SDL Guide (Part 2)
Complications of Major Exanthems
Knowing the specific complications of each exanthem is essential for risk-stratification, parent counselling, and timely referral decisions. Complications account for the majority of morbidity and mortality in these illnesses, and the ability to anticipate them — rather than merely react to them — defines high-quality paediatric care. Several of these complications are preventable through vaccination, adequate nutrition, and early recognition of warning signs. The pattern of complications differs strikingly between exanthems: measles is the most dangerous in immunocompromised and vitamin-A-deficient children; rubella's chief danger is to the fetus of a susceptible pregnant woman; varicella's complications are more common in adolescents, adults, and immunocompromised hosts; and scarlet fever's major preventable complication is acute rheumatic fever. Understanding which children are at highest risk allows the clinician to target surveillance and intervention appropriately.
Measles complications are the most serious and include:
- Pneumonia — the most common cause of death in measles, caused by the measles virus itself (giant cell pneumonia, especially dangerous in malnourished and immunocompromised children) or secondary bacterial pneumonia (Staphylococcus, Streptococcus)
- Encephalitis — occurs in 1–2 per 1000 cases; presents 2–6 days after rash onset with seizures and altered consciousness; mortality 15%, permanent neurological sequelae in 25%
- Subacute Sclerosing Panencephalitis (SSPE) — a rare but universally fatal late complication. A slow virus disease caused by persistent defective measles virus in the brain, occurring 7–10 years after the original measles infection. Presents with progressive cognitive decline, myoclonic jerks, and death within 1–3 years of diagnosis. Incidence is approximately 1 per 10,000 measles cases; more common when measles occurs before age 2 years
- Corneal ulceration and blindness — particularly in vitamin A deficient children; the leading infectious cause of blindness in developing countries
- Otitis media — common secondary bacterial complication
- Croup (laryngotracheobronchitis) — the barking cough may progress to true croup with stridor
Rubella complications in children are mild (encephalitis, thrombocytopenia rarely). The critical danger is Congenital Rubella Syndrome (CRS) when infection occurs in a pregnant woman, especially in the first trimester. CRS features include:
- Sensorineural hearing loss (most common — 60–90% of CRS cases)
- Congenital heart defects — patent ductus arteriosus (PDA) and pulmonary artery stenosis (PAS) are characteristic
- Cataracts and other ocular defects (glaucoma, microphthalmia)
- Microcephaly and developmental delay
- Risk is highest when infection occurs in the first 8–10 weeks of gestation (up to 90% risk of major defects); drops to 10–20% by 16 weeks; rare after 20 weeks
Chickenpox complications include:
- Secondary bacterial superinfection — Group A Streptococcus and Staphylococcus aureus can invade scratched lesions, causing cellulitis, impetigo, necrotising fasciitis, or septicaemia. This is the most common complication in healthy children
- Pneumonia — primary varicella pneumonia is more common and severe in adolescents/adults and immunocompromised children; can be life-threatening
- Encephalitis/cerebellar ataxia — cerebellar ataxia is the most common neurological complication in children and is usually benign and self-limiting; encephalitis is rarer but more serious
- Reye syndrome — associated with aspirin use during chickenpox (and influenza); causes hepatic failure and encephalopathy; aspirin is absolutely contraindicated in chickenpox
- Congenital varicella syndrome — if primary infection occurs in the first 20 weeks of pregnancy: skin scarring, limb hypoplasia, eye defects, neurological abnormalities
- Neonatal varicella — if mother develops chickenpox within 5 days before to 2 days after delivery, the neonate is at risk of severe disseminated varicella because maternal antibodies have not been transferred
Parvovirus B19 complications: aplastic crisis in haemolytic anaemias; fetal hydrops in pregnancy.
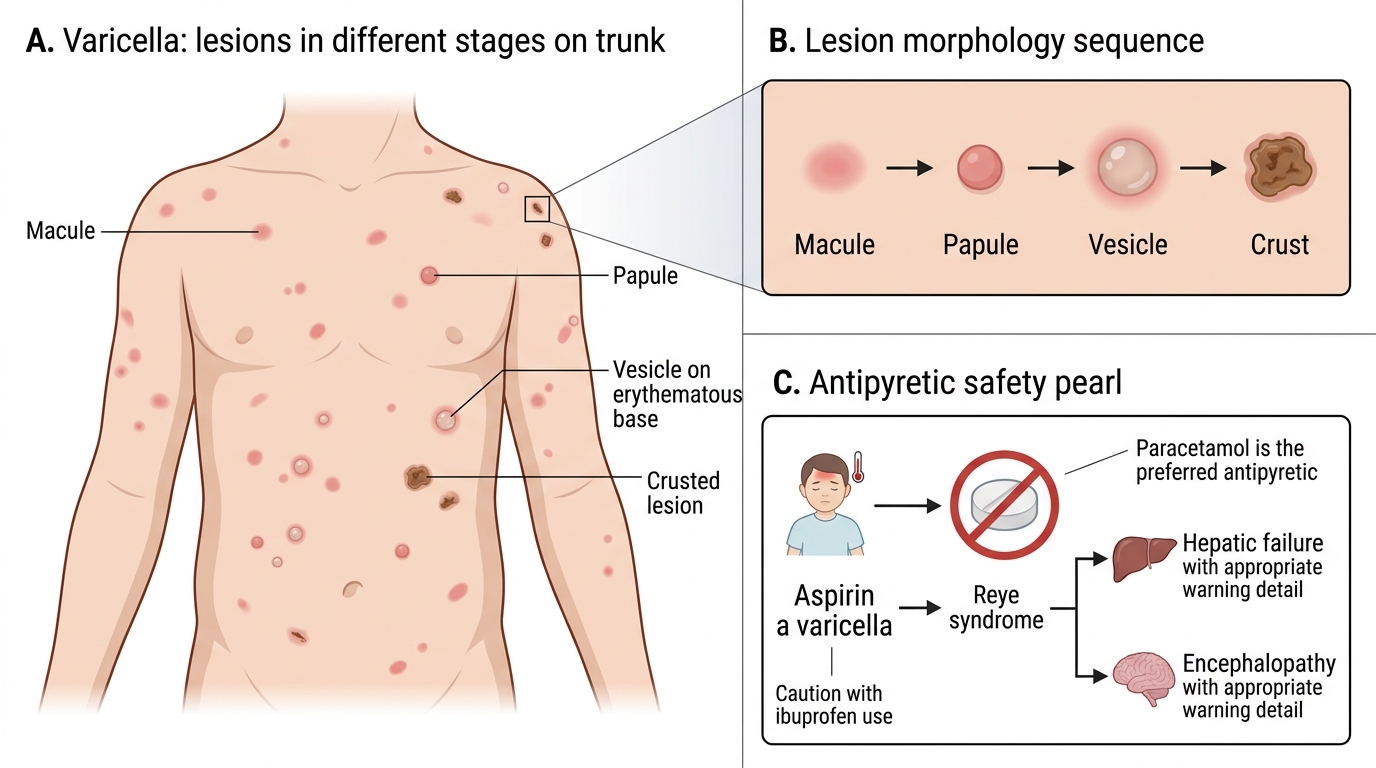
Varicella Lesion Morphology and Aspirin Safety Pearl
CLINICAL PEARL
Never give aspirin to a child with chickenpox or influenza — it is associated with Reye syndrome, a rare but life-threatening condition causing hepatic failure and encephalopathy. Use paracetamol for fever in children. Similarly, ibuprofen should be used with caution in varicella as it has been linked to secondary necrotising soft-tissue infections (GAS). Paracetamol is the antipyretic of choice in childhood exanthems.
SELF-CHECK
A 5-year-old boy had chickenpox 10 days ago. He now presents with worsening vomiting and lethargy following administration of aspirin for fever. His liver enzymes are markedly elevated. What is the most likely diagnosis, and what caused it?
A. Bacterial septicaemia due to chickenpox skin superinfection
B. Reye syndrome due to aspirin use during varicella
C. Viral hepatitis — direct varicella hepatic involvement
D. Measles encephalitis — unrelated to the aspirin use
Reveal Answer
Answer: B. Reye syndrome due to aspirin use during varicella
Reye syndrome is a rare but life-threatening condition characterised by non-inflammatory hepatic failure and encephalopathy. It occurs predominantly in children who receive aspirin during viral illnesses, particularly chickenpox (varicella) and influenza. The mitochondrial dysfunction caused by aspirin in the context of viral illness leads to fatty liver, hyperammonaemia, and cerebral oedema. Aspirin is absolutely contraindicated in these two illnesses in children under 16 years. Paracetamol should be used instead.
Management and Prevention
Management of exanthematous illnesses rests on three pillars: accurate diagnosis to guide specific therapy, supportive care to prevent complications, and prevention through vaccination to eliminate disease at the population level. For most exanthems, management is predominantly symptomatic — adequate hydration, antipyretics (paracetamol exclusively in children, never aspirin), and infection control to prevent spread. However, a subset of clinical situations demands specific, time-critical intervention: measles in a vitamin-A-deficient or malnourished child requires prompt supplementation to prevent blindness and death; varicella in an immunocompromised child requires systemic acyclovir to prevent disseminated disease; and scarlet fever requires a full ten-day course of penicillin to prevent acute rheumatic fever. The clinician must rapidly identify which child requires escalation beyond supportive care, and which preventive measures — vaccine, immunoglobulin, or post-exposure prophylaxis — are needed for exposed contacts.
Measles management:
- Supportive care: adequate hydration, antipyretics (paracetamol — not aspirin), nutritional support, treatment of secondary bacterial infections with appropriate antibiotics
- Vitamin A supplementation: WHO and IAP recommend vitamin A for ALL children with measles in India (given the background prevalence of deficiency). Dose by age:
- >12 months: 200,000 IU oral on day 1 and day 2
- 6–12 months: 100,000 IU on day 1 and day 2
- <6 months: 50,000 IU on day 1 and day 2
- An additional dose is given 4 weeks later if there is ophthalmological involvement (xerophthalmia/corneal ulceration)
- Isolation: respiratory isolation for 4 days after rash onset
- Post-exposure prophylaxis: MMR vaccine within 72 hours of exposure, OR normal human immunoglobulin (0.25 mL/kg IM, maximum 15 mL) within 6 days for susceptible immunocompromised contacts and unvaccinated infants <6 months
Rubella management:
- Symptomatic only — no specific antiviral therapy
- Paracetamol for fever; adequate rest
- Key intervention: identify and protect susceptible pregnant women (screen for rubella IgG at antenatal booking; if non-immune and exposed, offer immunoglobulin for symptomatic relief only — it does NOT reliably prevent CRS)
- Post-partum MMR vaccination for rubella-non-immune mothers
Varicella (Chickenpox) management:
- Healthy children with uncomplicated disease: symptomatic treatment — calamine lotion for pruritus, paracetamol for fever, trimmed fingernails to reduce scratching, bathing with antiseptic soap to prevent secondary infection
- Acyclovir is indicated for:
- Immunocompromised children (malignancy, HIV, high-dose steroids): oral acyclovir 20 mg/kg/dose (max 800 mg) 5 times daily for 7 days, or IV acyclovir 10–15 mg/kg 8-hourly for severe disease
- Secondary cases in a household (more severe than index case)
- Adolescents and adults (more severe disease)
- Neonatal varicella: IV acyclovir 10 mg/kg 8-hourly for 10 days
- Varicella-zoster immunoglobulin (VZIG): for post-exposure prophylaxis in susceptible immunocompromised individuals, neonates of mothers who developed chickenpox within 5 days before to 2 days after delivery, and susceptible pregnant women
- Secondary bacterial infection: treat with appropriate antibiotics (flucloxacillin/cloxacillin for Staphylococcus; amoxicillin-clavulanate for Streptococcus)
Scarlet fever management:
- Penicillin V (oral) or amoxicillin for 10 days is the treatment of choice
- For penicillin-allergic patients: erythromycin or azithromycin
- Benzathine penicillin G single IM dose if compliance is uncertain
- Adequate treatment prevents rheumatic fever (but does NOT reliably prevent post-streptococcal glomerulonephritis)
HFMD management:
- Supportive only: adequate hydration, paracetamol, topical anaesthetic mouthwashes for oral pain
- Most cases are self-limiting within 7–10 days
Prevention — National Immunization Schedule (India):
- MMR vaccine (Measles-Mumps-Rubella): first dose at 9–12 months, booster at 16–24 months
- MR vaccine (Measles-Rubella): given under India's MR campaign; routine schedule as MMR
- Varicella vaccine: IAP recommends at 15 months (first dose), second dose at 4–6 years (two-dose schedule)
- A child who has received two doses of MMR has >97% protection against measles; two doses of varicella vaccine provide >95% protection against disease and near-complete protection against severe disease
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
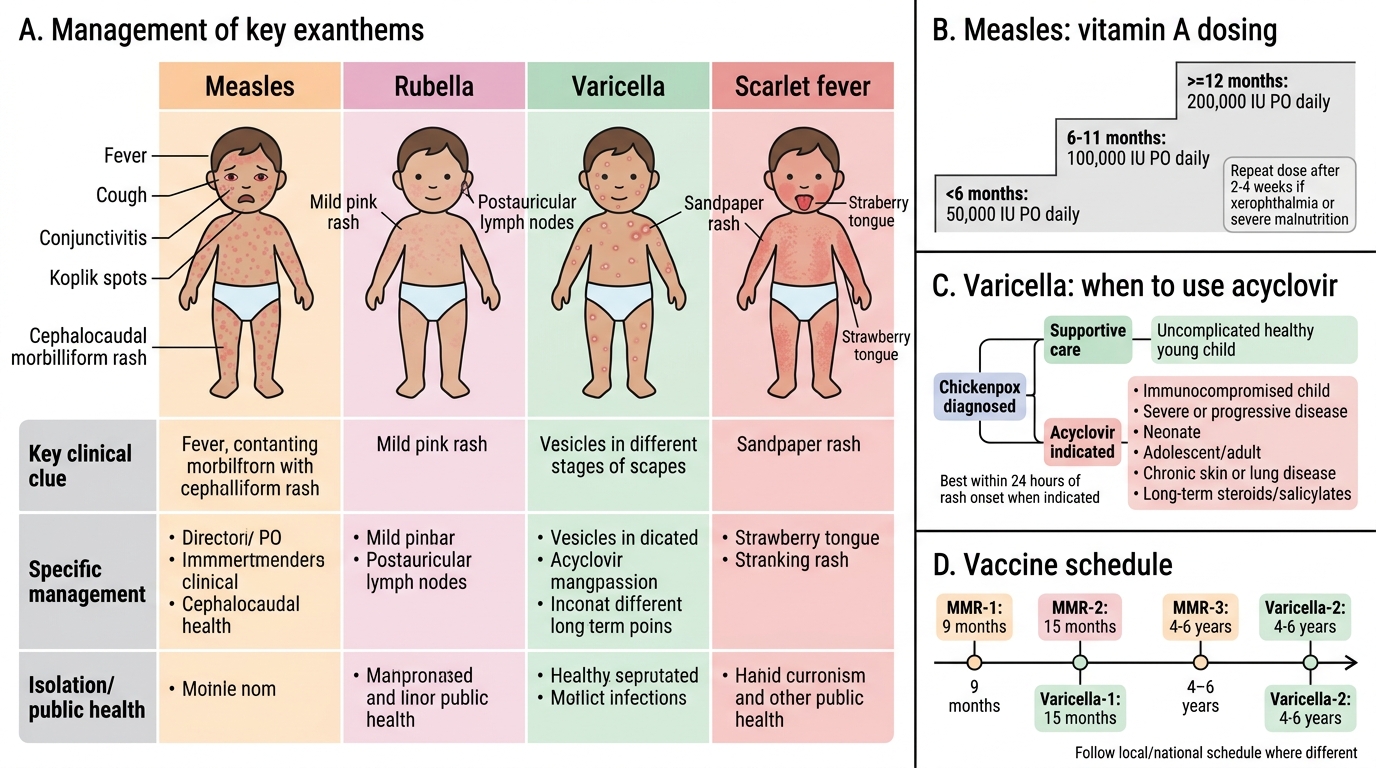
Management and Vaccination for Common Exanthems
Self-Assessment — Exanthematous Illnesses
Self-assessment in clinical medicine is most effective when it is case-driven rather than purely recall-based, because the diagnostic reasoning required at the bedside demands integration of multiple data streams — history, examination, epidemiological context, and immunisation status — rather than isolated facts. The three cases below are designed to test your ability to synthesise these elements. For each case, resist the urge to jump immediately to the diagnosis; instead, follow the clinical reasoning pathway: what is the most likely pathogen given the constellation of findings, what complications must be anticipated given the child's age and risk factors, and what specific — not just generic — management decisions follow from the diagnosis. Pay particular attention to the management questions: they are calibrated to test whether you know the specific doses, contraindications, and public health steps, not merely whether you can name the disease.
Case 1: A 3-year-old girl develops high fever (39.5°C), cough, runny nose, and red eyes for 4 days. On day 4, you find small white spots on her buccal mucosa and a red rash spreading from the face down the trunk. Her immunisation record shows she received OPV and pentavalent but NO MMR.
Questions:
- What is the diagnosis, and what specific finding confirms it?
- Which vitamin A dose should she receive, and for how many days?
- What post-exposure measures are needed for household contacts?
Case 2: A 6-year-old has chickenpox. The mother asks: 'My child has a fever — can I give aspirin?' She also asks whether her 10-year-old (who has acute lymphoblastic leukaemia, currently on chemotherapy) should be worried.
Questions:
- What is your advice about aspirin, and why?
- What is the risk to the sibling with ALL, and what management does the sibling require?
Case 3: A 14-year-old presents with sore throat, high fever (39°C), and a diffuse 'sandpaper' rash on the trunk and limbs. Examination reveals circumoral pallor, strawberry tongue, and linear petechiae in the antecubital fossa.
Questions:
- Identify the disease and the pathognomonic signs present.
- What antibiotic and duration would you prescribe?
- What is the most important preventable complication of untreated or inadequately treated disease?
SELF-CHECK
Which of the following is the MOST common cause of preventable blindness from an exanthematous illness in children in developing countries?
A. Congenital rubella — cataracts
B. Measles — corneal ulceration secondary to vitamin A deficiency
C. Varicella — ophthalmic herpes zoster
D. Scarlet fever — conjunctivitis
Reveal Answer
Answer: B. Measles — corneal ulceration secondary to vitamin A deficiency
Measles-associated corneal ulceration is the leading infectious cause of childhood blindness in the developing world. It occurs predominantly in children with vitamin A deficiency — measles depletes vitamin A stores, causing keratoconjunctivitis that can progress to corneal melting (keratomalacia) and permanent blindness. This is why WHO recommends routine vitamin A supplementation for ALL children diagnosed with measles in regions where vitamin A deficiency is prevalent, including India. Congenital rubella cataracts affect the neonate, not the child with acute illness.